Back to Home
Page of CD3WD Project or Back to list of CD3WD Publications
 |  |  | Disabled Village Children - A Guide for Community Health Workers, Rehabilitation Workers, and Families (Hesperian Foundation, 1999, 676 p.) |  |  | PART 1: WORKING WITH THE CHILD AND FAMILY: Information on Different Disabilities | |  | (introduction...) | | | Chapter 1: Introduction to PART 1: Making Therapy Functional and Fun | | | A. Where Do We Start? | | | Chapter 2: Ideas for Sharing Information from This Book | | | Chapter 3: Prevention of Disabilities | | | Chapter 4: Examining and Evaluating the Disabled Child | | | Chapter 5: Simple Ways to Measure and Record a Child’s Progress | | | B. Recognizing, Helping with, and Preventing Common Disabilities | | | Chapter 6: Guide for Identifying Disabilities | | | Chapter 7: Polio: Infantile Paralysis | | | Chapter 8: Contractures: Limbs That No Longer Straighten | | | Chapter 9: Cerebral Palsy | | | Chapter 10: Muscular Dystrophy: Gradual, Progressive Muscle Loss | | | Chapter 11: Club Feet, Flat Feet, Bow Legs, and Knock-Knees | | | Chapter 12: Common Birth Defects | | | Chapter 13: Children Who Stay Small or Have Weak Bones | | | Chapter 14: Erb’s Palsy: Arm Paralysis from Birth Injury | | | Chapter 15: Painful Joints | | | Chapter 16: Juvenile Arthritis | | | Chapter 17: Rheumatic Fever | | | Chapter 18: Hip Problems | | | Chapter 19: Bone Infections | | | Chapter 20: Spinal Curve and Other Back Deformities | | | Chapter 21: Tuberculosis of the Backbone: Pott’s Disease | | | Chapter 22: Spina Bifida | | | Chapter 23: Spinal Cord Injury | | | Chapter 24: Pressure Sores | | | Chapter 25: Urine and Bowel Management: With Spinal Cord Injury and Spina Bifida | | | Chapter 26: Leprosy: Hansen’s Disease | | | Chapter 27: Amputations | | | Chapter 28: Burns and Burn Deformities | | | Chapter 29: Fits: Epilepsy | | | Chapter 30: Blindness and Difficulty Seeing | | | Chapter 31: Deafness and Communication | | | Chapter 32: Mental Retardation: Down Syndrome, Cretinism, and Other Causes | | | Chapter 33: The Child with Several Severe Disabilities | | | C. Helping the Child Whose Mind and/or Body are Slow to Develop | | | Chapter 34: Child Development and Developmental Delay | | | Chapter 35: Early Stimulation and Development Activities | | | (introduction...) | | | 1) Head Control and Use of Senses | | | 2) Rolling and Twisting | | | 3) Gripping, Reaching, and Hand-eye Coordination | | | 4) Body Control, Sitting, and Balance | | | 5) Creeping and Crawling | | | 6) Standing, Walking, and Balance | | | 7) Communication and Speech | | | 8) Early Play Activities and Toys | | | D. Helping Children Develop and Become More Self-reliant | | | Chapter 36: Feeding | | | Chapter 37: Dressing | | | Chapter 38: Toilet Training | | | Chapter 39: Bathing (includes Care of the Teeth and Gums) | | | Chapter 40: Ways to Improve Learning and Behavior | | | Chapter 41: ‘Learning Disabilities’ in Children with Normal Intelligence | | | E. Exercises and Techniques | | | Chapter 42: Range-of-motion and Other Exercises | | | Chapter 43: Crutch Use, Cane Use, and Wheelchair Transfers |
|
Disabled Village Children - A Guide for Community Health Workers, Rehabilitation Workers, and Families (Hesperian Foundation, 1999, 676 p.)
PART 1: WORKING WITH THE CHILD AND FAMILY: Information on Different Disabilities
Figure
Photo by John Fago

Figure
Photo by John
Fago
Chapter 1: Introduction to PART 1: Making Therapy Functional and Fun
Most disabled people in the world live in villages and poor
communities where they never see a ‘rehabilitation expert’ or
‘physical therapist’. But this does not always mean that they have no
‘rehabilitation’ or ‘therapy’. In many villages and homes,
family members, local craftspersons, traditional healers, and disabled people
themselves have figured out ways for persons with disabilities to do things
better and move about more easily.
We have seen examples where local carpenters, tinsmiths,
leatherworkers or blacksmiths have put together simple crutches, carts, wooden
legs and other aids. We know parents who have figured out ways of adapting daily
activities so that their children can help do farm work or housework - and at
the same time get much of the exercise (therapy) they need.
|
Two words often used by people who work with disabled
persons are ‘rehabilitation’ and
‘therapy’.
Rehabilitation means returning of ability, or
helping a disabled person to manage better at home and in the community.
Therapy basically means treatment.
Physical therapy - or physiotherapy-is the art of
improving position, movement, strength, balance, and control of the body.
Occupational therapy is the art of helping a
disabled person learn to do useful or enjoyable activities.
We speak of ‘therapy’ as an art rather than a
science because there are many different beliefs and approaches, and because the
human feeling that goes into therapy is as important as the methods. |
Sometimes the ‘rehabilitation’ that families and
communities figure out by themselves works better in their situation than do
methods or aids introduced by outside professionals. Here are 2 examples:
1. In India, I met a villager who had lost a leg in
a house-building accident. Using his imagination, he had made himself an
artificial leg with a flexible foot out of strong wire with strips of an old
cotton blanket for padding. After several months, he had the chance to go to a
city where a professional ‘leg maker’ (prosthetist) made him a costly
modern fiberglass leg. The man tried using the new limb for a couple of months,
but it was heavy and hot. It did not let his stump breathe like his ‘wire
cage’ leg. And he could not squat to eat or do his toilet, as he could with
his homemade leg. Finally, he stopped using the costly new leg and went back to
the one he had made. For the climate and customs where he lived, it was more
appropriate.

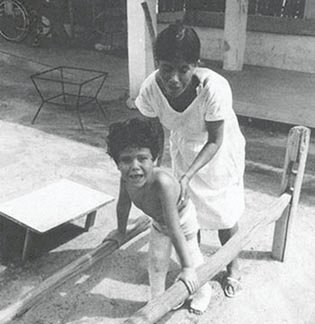
All children, as much as possible,
should get the exercise they need through daily work and play. (Morocco. Photo
by Charles Trieschmann)
2. In a small village in Mexico, over the years, the
community together with its deaf citizens has developed a simple but expressive
‘sign language’ using their hands, faces, mouths, and whole bodies to
communicate. As a result, children who are born deaf quickly and gracefully
learn to express themselves. They are well accepted in the community, and some
have grown up to become creative and respected craftspersons. This village
method of ‘total communication’ allows the deaf children to learn a
useful language more quickly, easily, and effectively than does the ‘lip
reading and speech’ method now taught in the cities. For children who are
born deaf, attempts to teach only lip-reading-and-spoken-language often end in
cruel disappointment. The ‘special educators’ in the cities could
learn a lot from these villagers.
Disabled children - if allowed - often show great imagination
and energy in figuring out ways to move about, communicate, or get what they
need. Much of what they do is, in effect, ‘therapy’, artfully adapted
for and by each child.
With a little help, encouragement, and freedom, the disabled
child can often become her own best therapist. One thing is certain: she
will make sure her therapy is ‘functional’ (useful), always changing
it to meet her immediate needs. A disabled child, like other children,
instinctively knows that life is to be lived NOW and that her body and her world
are there to be explored, used, and challenged. The best therapy is built
into everyday activities: play, work, relationship, rest, and adventure.
The challenge, then, for health workers and parents (as well as
for therapists), is to look for ways that children can get the
‘therapy’ they need in ways that are easy, interesting, and
functional.
This takes imagination and flexibility on the part of all those
working with disabled children. But mostly, it takes understanding. When family
members clearly understand the reasons for a particular therapy and the basic
principles involved, they can find many imaginative ways to do and adapt that
therapy.
‘Physical therapy’ to improve control of the head,
strength of the back, and use of both arms and hands together:

(a) in a city clinic
Photo: Cheyne Walk Spastic’s
Centre

(b) in a village home
Photo: PROJIMO, Ajoya, Mexico
|
Appropriate therapy helps the child to enjoy himself, be
useful, and take part with others, while mastering the skills for daily
living. |
Physical therapy and rehabilitation techniques have been
developed mostly in cities. Yet most of the world’s disabled children live
in villages and farms. Their parents are usually very busy growing the food and
doing the chores to keep the family fed and alive from day to day. In some ways,
this makes home therapy more difficult. But in other ways it provides a wide
range of possibilities for exciting therapy in which the child and his family
can meet life’s needs together.
Here is a story that tells how therapy can be adapted to village
life.

|
Maricela lives in a small village on a river. She has cerebral
palsy. When she was 4 years old, she was just beginning to walk.
But her knees bumped together when she tried to take steps. So
she did not try often. Also, her arms and hands were weak and did not work very
well.

Figure
Her family saved money and took Maricela to a rehabilitation
center in the city. After a long wait, a therapist examined her. He explained
that Maricela needed to stretch the muscles on the inner side of her thighs, so
her knees would not press together as much.
He recommended that her parents do special exercises with her,
and that they buy a special plastic seat to hold her knees wide apart.

Figure
He said she also needed exercises to strengthen and increase the
control of her hands and arms.

Figure
He suggested buying her some special toys, game boards, and aids
to practice handling and gripping things.
Maricela’s family could not afford these costly things. So
back in her village her father used whatever he could find to make similar aids
at low cost. First he made a special seat of sticks.

Figure
Later he made a better seat with pieces of wood, and an old
bucket to hold her legs apart.
Then, using a board, corn cobs and rings cut from bamboo, he
added a small table so that she could play games to develop hand control.

Figure

Figure
He also made a hand exerciser out of bamboo.

Figure
At first, while they were strange and new, Maricela used her
special seat and played with her special toys. But soon, she got bored and
stopped using them. She wanted to do the things that other children did. She
wanted to go with her father and brother to the cornfield. She wanted to help
her mother prepare food and wash the clothes. She wanted to be helpful and grown
up.
So she broke her special toys and refused - to sit in her
special seat. Her parents were furious with her - and she loved it! She would
sit for hours with her knees together and her legs bent back. Walking began to
get more difficult for her, so she did not walk much.

Figure
Her parents then visited a small rehabilitation center in a
neighboring village. The village team suggested that they look for new ways to
help Maricela keep her knees apart and improve control of her arms and hands -
ways that would be exciting and help her to develop and practice useful skills
together with the rest of her family. Here are some of the ideas that Maricela
and her parents came up with:
When she was good (and sometimes even if she was
not) her father would let her help shell corn with him and the other children.
Because she had trouble holding the corn and snapping off the grain with her
fingers, her father made a special holder and scraper.
Figure
The basket between her legs held her knees apart, and the
shelling of the corn strengthened her arms, gave her practice gripping, and
improved her coordination and control.

Figure
It was hard, important work that Maricela found she could do.
And she loved it!
Maricela’s mother sometimes invited her to help wash the
clothes at the river. Maricela would sit at the river’s edge with a big
‘washing rock’ between her legs. She would wash the clothes by
squeezing and beating them against the rock - just like her mother.

Figure
The rock kept her knees apart and the squeezing and banging
strengthened her hands and improved her control. But what mattered was getting
the clothes clean. It was hard work. But she found it easy - and fun!
Coming back from the river, Maricela just had to walk. It was
too far to crawl. And besides, she had to help her mother carry back the washed
clothes. This was hard, but she tried hard, and could - do it!

Figure
Carrying the pails of clothes helped her learn to walk without
bending and jerking her arms so much.
To help Maricela grip the handle of the pail easier, her father
wrapped a long strip of old bicycle inner tube very tightly around the handle.
But when Maricela’s hand sweated, the smooth rubber got slippery. So her
father wound a thin rope around the rubber. This way, Maricela could hold it
better.
Figure
As time passed she learned how to carry a bucket of clothes on
her head - then a bucket of water. To do this took a lot of practice with
balance and control of movement. She just had to keep her legs farther apart to
keep her balance.
Her mother was almost afraid to let her try carrying the water.
But Maricela was stubborn - and she did it! Maricela also discovered that if she
floated a gourd dipper (or a big leaf) on top of the water, it helped keep the
water from splashing out.

Figure
So, by trying different things, Maricela’s family, and
Maricela herself, learned ways to create therapy and aids that were effective,
useful, and enjoyable.
Maricela did learn to walk better, and to use her hands and arms
to do many things. But this took a long time. Sometimes she would try something
that was too hard, and almost give up. But when her little brother would say she
could not do it, she would keep trying until she succeeded.
Even when Maricela liked doing something, because she was a
child she would get bored and not keep doing it for long. Her parents always had
to look for new ways for her to get her therapy. It became a challenge and a
game for them, too.
Of course, Maricela loved horses. So her father made her a
rocking horse out of old logs, branches of trees, and a piece of rope for a
tail.

Figure
Her father noticed that she was beginning to walk on tiptoe, so
he made special stirrups for the rocking horse. With these, when she rocked, her
feet stretched up in a more normal position.

Figure
The rocking horse kept her knees apart, strengthened her hands,
and helped her improve her balance. Maricela loved her horse and sometimes
rocked for an hour or more. When she got off, it seemed she could walk better.
After Maricela had learned to ride the rocking horse, she wanted
to ride the real thing. She begged and begged. So one day her father let her
ride with him to the cornfield on his donkey. He suggested she ride in front of
him where he could hold her. But she insisted on riding behind, like other
children do.
So he fixed some stirrups and let her ride behind. Her legs were
spread wide and she hung on tightly. It was excellent therapy-but nobody called
it that.
Figure
In the cornfield she helped her father and brother clean the
weeds out from among the young corn plants. That was good for the young plants -
and for her, too! But after several trips to the cornfield on the donkey with
her father, Maricela begged him to let her ride alone. He was nervous, but he
let her try.
She could do it - and what confidence it gave her! Soon Maricela
was preparing lunch for her father and brother and taking it to them in the
cornfield - all by herself. Now she found she could do many other things she
never thought she could. Although she was still awkward, and at times had to
look for special ways to do things, she found she could do most anything she
wanted or needed to.

Figure
|
The example of Maricela’s ‘therapy’ cannot and
should not be copied - but instead, learned from. In fact, the story suggests
that no approach to rehabilitation should be copied exactly. Our
challenge is to understand each child’s needs, and then to look for ways
to adapt her rehabilitation to both the limitations and possibilities within
her family and community. We must always look for ways to make therapy
functional and fun.
Recently, some ‘appropriate technology’ groups have
tried to adapt standard ‘rehabilitation aids’ to poor rural
communities. However, many of their designs are modeled fairly closely after the
same old city originals, using bamboo and string instead of plastic and
aluminum. Some of these low-cost designs are excellent. But more effort is
needed to make use of the unique possibilities for rehabilitation and therapy
that exist in the village, farm, or fishing camp.
Maricela’s family did just this. The basket of corn, the
washing rock, the rocking horse, and the donkey all became ‘therapy
aids’ to help Maricela spread her spastic legs, and at the same time, to
take part in the life of her family and community.
But not every family shells corn in baskets, washes clothes on
rocks, or has a donkey. And not every disabled child has Maricela’s needs
and strengths. So we repeat:
|
We should encourage each family to observe the specific needs
and possibilities of their disabled child, to understand the basic principles of
the therapy needed, and then to look for ways to adapt the therapy to the
child’s and family’s daily life. |

Figure
A. Where Do We Start?
Chapter 2: Ideas for Sharing Information from This Book
Most of the information in this book will be
useful to health workers and village rehabilitation workers who see many
disabled children. Some of the information will also be useful for
the family of a disabled child. However, a family with one disabled child will
usually not need, or be able to afford this whole book. It has information about
so many different disabilities, that parents may have difficulty finding the
information that applies to their child.
Also, learning from a book is often not the best way to learn
something. A lot of methods, aids, and exercises can be learned more easily from
other persons, through watching and through guided practice. But after a village
worker has taught parents how to do certain exercises, or shown them an example
of a homemade aid, printed instruction sheets with clear drawings can be a
big help. Sometimes they can make the difference between whether the
recommendations are followed at home, or not.
There are certain pages or parts of this book that you may want
to give to families after you explain and teach to them selected exercises or
activities. For example, to the family of a girl with arthritis, you may want to
give some of the “Exercise Instruction Sheets” at the end of Chapter
42, and the “Information Sheet on Aspirin”. You may also want to give
them pages from Chapter 16 on arthritis, and to mark the exercises and
activities that are important to their child.
To the family of a young child who is slow to develop, you may
want to give pages from the chapters on child development and early stimulation
activities (Chapters 34 and 35). For a more advanced child you could give the
family material from the chapters on self-care (Chapters 36 to 39).
Depending on the interest and reading ability of the family, you
may want to give them a whole chapter (or chapters) about their child’s
disability. For example, the chapters on cerebral palsy (Chapter 9) or deafness
(Chapter 31). An older child who is paralyzed from a broken back might
appreciate having a copy of the chapter on spinal cord injury. Letting him and
his family take home the chapters on pressure sores and urine and bowel control
could even save his life! His family may also want to take home plans for making
a low-cost wheelchair, to see if the carpenter and blacksmith in their village
could make one.
In Project PROJIMO in Mexico, the village rehabilitation team
keeps a big file box with copies of the different pages and chapters that they
have found most useful for giving to families. (In fact, the exercise sheets at
the end of Chapter 42 were originally prepared separately to give to families.
Later, we decided to include them in this book.)

Suggestion: Keep a file of pages,
chapters, and information sheets to give to families.
Marking the information that applies to the child
On any page or chapter that you give to parents, some of the
information or suggestions will apply more than others to their child.
We suggest that you (1) circle the activities or suggestions
that would be most helpful to the child in his present condition or level of
development. You could also put an “X” through anything that
should not be done or might be harmful for that child.(2)

Figure
Here is an example. If the child is spastic and beginning to
sit, the first 3 activities can help her to improve balance and to develop
controlled body movement. So circle these. The next 3 activities will still be
too difficult and could increase spasticity. Put an “X”
through these so the family does not do them.
Making copies of pages can be costly. Or you may have to
go a long way for them. Also, there will be times when you want to give a family
written suggestions or drawings that you have not copied in advance.
Perhaps some of the children or young people who are at the
village center, either for rehabilitation or as learners-and-workers, can help
trace drawings from the book. If they have some artistic skill, they can make
the drawings larger, or make the child in the drawing look like the child that
they are to be used with.*
* Ideas for drawing and for copying drawings at
larger size are in Helping Health Workers Learn, p. 12-1 to
12-21.

Minerva, a girl with polio who is
working and learning at PROJIMO, helps adapt drawings from this book to the
needs of specific children.
If someone prepares a set of large drawings in advance, perhaps
a disabled child who visits the village center can trace the drawings of
exercises he needs to do at home. Giving the child this responsibility from the
start makes it more likely that he will do the exercises at home.
If you make your own ‘hand out’ sheets (instead of
just copying pages of this book) you can use the local language and
villagers’ way of saying things. You can also adapt the drawings to the
hair style and dress that people feel ‘at home’ with.
Whatever you do, try to keep both your language and drawings
simple and clear. Avoid unfamiliar words.
Also, try to think of ways of adapting exercises or
activities to the local situation.
For example, (1) suppose you live in a fishing
village, and want to make copies of a drawing showing an aid for
strengthening the wrist. Instead of just copying a method like this from a book,
(2) you might add a drawing like this one. This will encourage parents to think
of ways to do exercises that involve their child in the life and action of their
community.

Figure

Figure
Remember: Written pages and drawings can be a big help,
but they should not be a substitute for teaching and showing. To help a family
understand activities or exercises that are needed:
1. First show and explain.
2. Guide them in doing
it until they do it right and understand why.
3. Then, give them the
instruction sheet and explain the main points.
These steps are explained with examples and drawings.
|
As much as you can, try not to use this book for
giving exact instructions on how to do things. Instead, encourage everyone to
use it as a source of ideas, in order to figure out better ways to help their
children lead fuller lives and manage better in their communities.
|
REMEMBER...
One of the best ways to share information from this book is to:
1. SHOW other people how to do things.

Village rehabilitation workers
and family members learn in an outdoor class. Here they practice a
hip-stretching exercise. Behind them, drawings on the blackboard show which
muscles are stretched.
2. Then help them LEARN BY DOING it themselves - under
your guidance.

Teaching a village health worker
how to stretch a tight heel cord
3. And to help them remember, give them a DRAWING or
INSTRUCTION SHEET.

Figure
|
IMPORTANT: Try to help people to understand
not only what to do, but also why. Perhaps you can hold classes
using information from this book. Try to combine hands-on practice with
discussion of principles and reasons. |
Chapter 3: Prevention of Disabilities
Because this is a book on
‘rehabilitation’, it is mostly about children who are
already disabled. However, preventing disabilities is also very
important. For this reason, in most chapters on specific disabilities, we
include suggestions for preventing them.
Notice that we place the discussion of prevention at the end
of each chapter, not at the beginning. This is because people are usually
not concerned about disability until someone they love becomes disabled. Then
their first concern is to help that person. After we have helped a
family to do something for their disabled child, we can interest them in ways to
prevent disability in other members of the family and community.
We mention this because when health professionals design
community programs, often they try to put prevention first - and find that
people do not show much interest. However, when a group of parents comes
together to help their disabled children, after their immediate needs are being
met, they may work hard for disability prevention.
|
For a community program to be successful, start with what the
people feel is important, and work from there. |
To prevent disabilities, we must understand the causes. In most
parts of the world, many causes of disability relate to poverty. For
example:
· When mothers do
not get enough to eat during pregnancy, often their babies are born early or
underweight. These babies are much more likely to have cerebral palsy, which is
one of the most common severe disabilities. Also, some birth defects are related
to poor nutrition during the first months of pregnancy.
· When babies and young
children do not get enough to eat, they get infections more easily and more
seriously. Diarrhea in a fat baby is usually a mild illness. But in a very thin,
malnourished baby, diarrhea often leads to serious dehydration, high fever, and
sometimes brain damage with fits or cerebral palsy.
· Poor sanitation and crowded
living conditions, together with poor food, make diseases such as
tuberculosis - and the severe disabilities it causes - much more common.
· Lack of basic health and
rehabilitation services in poor communities makes disabilities more common
and more severe. Often secondary disabilities develop that could be prevented
with early care.
To prevent the disabilities that result from poverty, big
changes are needed in our social order. There needs to be fairer distribution of
land, resources, information, and power. Such changes will happen only when the
poor find the courage to organize, to work together, and to demand their
rights. Disabled persons and their families can become leaders in this
process. Only through a more just society can we hope for a long-term,
far-reaching answer to the prevention of disabilities caused by poverty.
Although the most complete prevention of disabilities related to
poverty depends on social change, this will take time. However, more immediate
actions at family, community, and national levels can help prevent some
disabilities. For example,
· Polio, in certain
situations, can be prevented through vaccination. (However, effective
vaccination depends on much more than good vaccine. See the box.)
|
Why, since a good vaccine exists, is there still so much polio
in so many countries?
EFFECTIVE VACCINATION DEPENDS ON MANY FACTORS:
TECHNICAL Production and supply of safe, effective,
vaccine.

Figure
ECONOMIC (Cost of vaccine and of getting it to the
children.) Leaders in poorer countries must decide that stopping polio is worth
the expense.

Figure
MANAGEMENT Knowledge of needs, planning, transportation,
and distribution of the vaccine.
KEEPING POLIO VACCINE FROZEN (In many countries, 1/3 of
vaccines are spoiled by the time they reach the children.)
EDUCATION People must understand the value of vaccination
and want to cooperate. Health workers must know how important it is to keep
polio vaccine frozen.
POLITICAL Vaccination programs are most successful where
the government fairly represents the people and has their full participation in
countrywide vaccination campaigns.
ETHICAL (Honesty and good will) Doctors, health workers,
and citizens must try to see that vaccine reaches all children. (In some
countries, some doctors throw vaccines away and fill out false reports, and
health inspectors do not care enough to try to stop what is happening.) |
In places where vaccination is not available or not fully
effective, families and communities can help to lower the chance of
paralysis from polio in other ways:
¨ by breast feeding
their children as long as possible.
¨ by not letting their children
get unnecessary injections.
· Brain damage and
fits can become less frequent if mothers and midwives take added
precautions during pregnancy and childbirth, and if they vaccinate children
against measles.
· Some birth defects
and mental retardation can be prevented if mothers avoid most
medicines during pregnancy, and spend the money they save on food.
· Spinal cord injury
could be greatly reduced if fathers would spend on education and community
safety what they now spend on alcohol and guns.
· Leprosy could mostly be
prevented if people would stop fearing and rejecting persons with
leprosy. By being more supportive and encouraging early home treatment, the
community could help prevent the spread of leprosy, since persons being treated
no longer spread it.
· Blindness in young
children in some countries is caused by not eating enough foods with vitamin
A. Again this relates to poverty. However, many people do not know that they
can prevent this blindness by feeding their children dark green leafy
vegetables, yellow fruits, or even certain weeds and wild fruit. Also, some
kinds of deafness and mental retardation can be prevented by
using iodized salt during pregnancy.
· Disability caused by
poisons in food, water, air, or workplace. The recent, common, worldwide use
of chemicals to kill insects and weeds has become a major health problem. Often
villagers use these pesticides without any knowledge of their risks, or of the
precautions they should take. As a result, many become paralyzed, blind, or
disabled in other ways.
To prevent these problems, people need to learn about the
dangers, not only to themselves and their children but to animals, birds, land,
and to the whole ‘balance of nature’. Less dangerous ways to control
pests give better results over time. Laws are also needed to prohibit the most
dangerous products and to provide clear warnings.
|
TO PROTECT AGAINST PESTICIDE POISONING
· Stand so that wind blows spray
away from you.
· Wear protective clothing,
covering the whole body.

Figure
· Wash whole body and change
clothes immediately after spraying.
· Wash clothes after spraying.
· Do not let wash water get into
drinking supply.
· Do not use spray containers
for food or water.
· Do not let children play with
spray containers.
CAUTION: Make sure that children, and
women who are pregnant or breast feeding, stay away from all pesticides. |
|
· Poisonous foods in some
areas are a major cause of disability. In parts of India, thousands of farm
workers who are paid with a poisonous variety of lentils suffer paralysis
from ‘lathyrism’. The poor know the danger but have nothing
else to eat. Fair wages and less corruption are needed to correct this
situation.
· Fluoride poisoning
(fluorosis), mainly from drinking water, is a common cause of bone deformities
(knock-knees) in parts of India and other places. Public health measures are
needed to provide safe water.*
* Note: Although too much fluoride is
harmful, some is necessary for healthy bones and teeth. In some areas fluoride
needs to be removed from drinking water; in other areas it needs to be
added.
|
The 4 biggest causes of ‘crippling’ in India,
affecting over 2 million people, are reported to be polio, iodine deficiency,
fluorosis, and lathyrism. Given the political will, all could be completely
prevented! |
· Dangerous work
conditions, poisons in the air, and lack of basic safety measures result in
many disabilities. These include burns, amputations, blindness, and back and
head injuries. In some countries, the use of asbestos for roofs or walls in
schools, work places, and homes causes disabling lung diseases. Strict public
health measures and an informed, organized people are needed to bring
improvements.
· Certain dangerous
medicines, known to sometimes cause disabilities, are now prohibited in the
countries that make them, but are still sold in other countries. For example,
diarrhea medicines containing clioquinol caused thousands of cases of blindness
and paralysis in Japan. (A good book discussing dangerous medicines in poor
countries is Bitter Pills by Dianna Melrose.)
The high cost, overuse, and misuse of medicines in
general adds greatly to the amount of poverty and disability in the world today.
Better education of both doctors and people, and more effective international
laws are needed to bring about more sensible supply and use of medicines.
WHO SHOULD BE RESPONSIBLE FOR DISABILITY PREVENTION
Notice that many of the specific preventive measures we have
discussed, just like the more general social measures, depend on increased
awareness, community participation, and new ways of looking at things. These
changes do not just happen. They require a process of education, organization,
and struggle led by those who are most deeply concerned.
Most able-bodied persons are not very concerned about disability
or trying to prevent it. Often people think, “Oh, that could never happen
to me!” - until it does.
Those who are most concerned about disability are usually
disabled persons themselves and their families. Based on this concern, they can
become leaders and community educators for disability prevention.
Disability can affect everybody,
and sometime in our lives it usually does.
They can do this in an informal, person-to-person way. For
example,

Figure
Or disabled children and families can join together to form
prevention campaigns. In one village, mothers put on short plays to inform the
whole community about the importance of breast feeding and vaccination. In
Project PROJIMO, Mexico, disabled rehabilitation workers have helped to
vaccinate children in remote mountain villages.
In PART 1 of this book, where we discuss different disabilities,
we also include basic information on prevention. We hope that those of you
who use this book for children who are already disabled, will also work actively
towards disability prevention.
PREVENTING SECONDARY DISABILITIES
So far we have talked mainly about preventing original or
‘primary’ disabilities, such as polio or spinal cord injury. But the
prevention of ‘secondary’ disabilities is also very important, and is
one of the main concerns of rehabilitation.
By ‘secondary’ disabilities we mean further
disabilities or complications that can appear after, and because of, the
original disability.
For example, consider a child with polio or cerebral palsy who
at first is unable to walk. She gradually loses the normal range-of-motion of
joints in her legs. Shortened muscles, called
‘contractures’, keep her legs from straightening. This
secondary disability may limit the child’s ability to function or to walk
even more than the original paralysis:

This child, after polio,
gradually developed contractures in her
The contractures (not the
original paralysis) kept her from being able to stand or walk.

If the contractures had been
prevented through early and continued range-of-motion exercises, the child would
have been able to stand and walk.
Most contractures can be corrected. But it may take a long time
and a lot of expense - perhaps even surgery It is far better to: PREVENT
CONTRACTURES BEFORE THEY START.
Because contractures develop as a common complication in many
disabilities, we discuss them in a separate chapter (Chapter 8). Range-of-motion
exercises to help prevent and correct contractures are described in Chapter 42.
Use of plaster casts to correct contractures is described in Chapter 59.
Many other secondary disabilities will also develop
unless preventive measures are taken. Some examples are pressure sores in
children with spinal cord injury (see Chapter 24), spinal curve in a
child with a weak back or with one leg shorter than the other (see Chapter
20), head injuries due to fits. Preventive measures for many other
secondary disabilities are discussed in the chapters on the specific
disabilities.
In several places we discuss problems or disabilities that
are commonly caused by medical treatment or orthopedic aids. For example,
· The medicine
for fits, phenytoin, produces serious swelling of the gums in some children.
This can partly be prevented by brushing the teeth regularly.
· Crutches that press
hard under the armpit can damage nerves and gradually paralyze the hands.
Shorter crutches, or lower-arm crutches (like those shown above) prevent this
problem.
· Surgery is sometimes
done to remove contractures that actually help a child to move or function
better. So worse difficulties result. The benefits or possible harm of surgery
should be carefully evaluated before it is done.
· Some braces or aids that help
a child at first, may later actually hold her back.
To prevent these mistakes, it is essential to evaluate the
needs of each child carefully, and repeat evaluations periodically. We must
take great care to prevent further disability caused by treatment.
|
The first responsibility of a rehabilitation worker or
parent, like the healer, should be to: DO NO HARM |
In addition to secondary disabilities that are physical, others
may be psychological or social (affecting the child’s mind, behavior, or
place in the community).
Some disabled children develop serious behavior problems.
This is often because they find their bad behavior brings them more attention
and ‘rewards’ than their good behavior. Chapter 40 discusses ways that
parents can help prevent tantrums and bad behavior in disabled children.
The biggest secondary handicap for many disabled children
(and adults) usually comes from the lack of understanding and acceptance by
other people. PART 2 of this book talks about how the community can be
involved in taking a more active, supportive role in relating to the disabled
and helping them to meet their needs. In PART 2 we also discuss what disabled
persons and their families can do, in the community, to promote better
understanding and prevent disability from becoming a serious handicap.
|
Prevention of secondary disability is a basic part of
rehabilitation. |
|
THE NEED FOR MORE SENSIBLE AND LIMITED USE OF INJECTIONS
|

|
The overuse and misuse of medicines in the world today has
become a major cause of health problems and disabilities. This is partly
because medicines are so often prescribed or given wrongly (for example, certain
medicines taken in pregnancy can cause birth defects). And it is partly because
both poor families and poor nations spend a great deal of money on overpriced,
unnecessary, or dangerous medicines. The money could be better spent on things
that protect their health - such as food, vaccinations, better water, and more
appropriate education. Some medicines, of course, when correctly used are of
great importance to health. But most are not. Of the 30,000 medicinal
products sold in most countries, the World Health Organization says that only
about 250 are needed.
In most of the world, doctors,
health workers, and the people make giving and getting injections too big a part
of health care.
In many countries, injections have become the ‘modern
magic’. People demand them because doctors and health workers often
prescribe them, and doctors and health workers prescribe them too often because
people demand them.

Figure
HOW INJECTIONS DISABLE CHILDREN
Giving injections with an unclean needle or syringe is a common
cause of infection. Sometimes these infections can lead to
paralysis, or spinal cord injury, or death.
Also, some injected medicines can do harm. Dangerous allergic
reactions, poisoning, and deafness are sometimes caused by injecting
certain medicines - often when they are not needed.
Overuse by doctors and midwives of injectable hormones to
speed up childbirth and ‘give force’ to the mother has become a major
cause of babies born with brain damage, cerebral palsy, and fits
in many countries.
This child was injected with a needle that was not sterile
(clean). The dirty needle caused an infected abscess (pocket of pus) that in
time burst and drained. The child had been injected for a cold. It would have
been better to give him no medicine at all.

Figure

Figure
The disability most often caused by injections is paralysis
from polio. Some experts say that each year up to 2 million children are
paralyzed by polio because of injections. Nearly all of these injections are
given when they are not needed.
It happens like this. Children who are infected by the polio
virus usually only have signs of a bad cold or ‘flu’. Most get well in
a few days, without developing paralysis. But the risk of paralysis increases if
the child’s muscles are injured or irritated. Injections of any kind of
medicine irritate the muscles. Messages from the irritated muscles travel up the
nerves to the spinal cord, and cause changes that let the polio
virus produce paralysis.

1 out of every 3 cases of
paralysis from polio is caused by injections.
Unfortunately, when children develop a cold or ‘flu’
caused by the polio virus, their parents often take them to a doctor or health
worker for an injection. Many times the result is paralysis, which is usually
worse in the leg on the side that was injected. Many people used to think that
paralysis in a leg after an injection was caused because the needle ‘hit a
nerve’. We now know that in most cases the paralysis was caused by polio.
Because it was brought on or ‘provoked’ by an injection, this is
called ‘provocation polio’.
It is very important that mothers - and doctors - remember
that children should not be given injections when they have signs of a cold
with fever or ‘flu’. It might be polio, and an injection could bring
on paralysis.
|
If injections are given to children only when they are
really needed, millions of cases of paralysis from polio could be prevented.
|
The worldwide epidemic of unnecessary injections each
year sickens, kills, or disables millions of persons, especially children. An
international campaign is needed to re-educate doctors, health workers,
traditional healers (many of whom also now overuse injections), and the people
themselves.
Combatting misuse and overuse of medicines is as important a
preventive measure as is vaccination, clean water, or the correct use of
latrines.
Health workers, schoolteachers, and community organizers should
all work to ‘de-mystify’ or take the magic out of injections, and to
help people always to weigh the possible risks and benefits before using
any medication.
For skits and ideas on teaching people about the danger of
unnecessary injections, see Helping Health Workers Learn,
Chapters 18, 19, and 27.
|
Note: When used correctly, certain injected medicines
are important to health. Vaccinations, including those that are injected,
are very important to protect a child’s health and prevent disability.
However, to avoid paralysis from polio, it is best not to give
vaccinations (immunizations) or any other injection when a child has a fever or
signs of a cold. This could be a mild polio infection, and giving an injection
could cause paralysis. |

AVOID UNNECESSARY
INJECTIONS
|
WAR AS A CAUSE OF CHILD DISABILITY
Armed violence is increasing. Since 1980, 45 countries have been
involved in 40 wars, with over four million soldiers. In today’s wars,
more civilians than soldiers are killed or disabled, and most are women and
children. In World War One, only 5 percent of persons killed or injured were
civilians. Today, 80 to 90 percent are civilians. At least 3 times as many
people are injured as are killed.
The increased poverty and ‘hard times’ caused by war
also lead to many disabilities. There are 25 to 30 million refugees, many living
under dangerous and unhealthy conditions. One-third of the world’s children
lack adequate food and basic health care. Millions are homeless. Yet in 1985,
world leaders spent 1,000 billion US dollars on war and arms - twice as much as
in 1981.

Nicaraguan child disabled by a
‘Contra’ bomb. The Contras are rebel troops supported by the United
States Government to overthrow the new government in Nicaragua. (Photo by Marc
Krizack, Links)
War, terrorism, and torture have become tools of the powerful
for economic, political and social control. When the peoples of poor countries
dare to get rid of their dictators and form popular governments that work toward
fairer distribution, the rich, powerful countries often try to destroy those new
governments. They pay for terrorism, long wars, and the destruction of schools,
health centers, and production. The result is still more poverty, disease, and
disability.
To help change this situation, we disabled persons of the
world must join with all who are disadvantaged or treated unfairly, to struggle
for a new, more truly human, world order.
|
Terrorism is too often fought with terrorism. During the U.S.
attack on Libya in April, 1986, bombs hit a school for disabled children. Such
actions do not stop terrorism; they merely kill and disable innocent persons.
“AN EYE FOR AN EYE WILL MAKE THE WHOLE WORLD
BLIND.”-Mahatma Gandhi. |
Chapter 4: Examining and Evaluating the Disabled Child
To decide what kind of special help, if any, a disabled child
may need, first we need to learn as much as we can about the child. Although we
may be concerned about her difficulties, we must always try to look at the
whole child. Remember that:

Figure
|
A child’s abilities are more important than her
disabilities. |
The aim of rehabilitation is to help the child to
function better at home and in the community. So when you
examine a child, try to relate all your observations to what the child can
do, cannot do, and might be able to do.
What a child is and does depends partly on other persons. So we
must also look at the child’s abilities and difficulties in relation to her
home, her family, and her village or neighborhood.
To evaluate a child’s needs, try to answer these questions:
· What can the
child do and not do? How does this compare with other children the same age
in your community?
· What problems does the
child have? How and when did they begin? Are they getting better, worse, or are
they the same?
· In what ways are the
child’s body, mind, senses, or behavior affected? How does
each specific problem affect what she does?
· What secondary problems
are developing? (Problems that result after and because of the original
problem.)
· What is the home
situation like? What are the resources and limitations within the family
and community that may increase or hold back the child’s possibilities?
· In what way has the child
adjusted to her disability, or learned to manage?
To find the answers to these questions, a health or
rehabilitation worker needs to do 3 things:
1. Observe the child carefully - including
her interaction with the family and with other persons.
2. Take a ‘history’. Ask the parents and child
(if old enough) for all information they can provide. Obtain medical records if
possible.
3. Examine the child to find out how well and in what way
different parts of her body and mind work, how developed they are, and how much
they affect her strengths, weaknesses or problems.
|
BE SURE TO LOOK AT THE WHOLE CHILD - NOT JUST THE
DISABILITY |
Observation of the child can begin from the first moment the
health worker or rehabilitation worker sees the child and her family. It can
begin in the waiting area of a village center, the home, or the street, and
should continue through the history-taking, examination, and follow-up visits.
Therefore, we do not discuss ‘observation’ separately, but include it
with these other areas.
It is usually best to ask questions BEFORE beginning to
examine the child - so that we have a better idea what to look for.
Therefore, we will discuss history-taking and then examination. But first a word
about keeping records.
RECORD KEEPING
For a village rehabilitation worker who helps many children,
writing notes or records can be important for following their progress. Also,
parents of a disabled child may find that keeping simple records gives them a
better sense of how their child is doing.
|
Sample RECORD SHEETS included in this book |
RECORD SHEET
number |
|
Child history |
1 |
|
Physical examination |
2 |
|
Tests of nervous system |
3 |
|
Factors affecting child development |
4 |
|
Evaluation of progress |
5 |
|
Child development chart |
6 |
Six sample RECORD SHEETS are on pages 37 to 41, 50, 292, and
293. You can use these as a guide for getting and recording basic information.
But you will want to follow with more detailed questions and examination,
depending on what you find.
Sheets 1 and 2 will be useful for most disabled children. Sheets
3, 4, and 6 are for children who may have brain damage or seem slow for their
age. Sheet 5 is a simple form for evaluating the progress of children 5 years
old or older.
HISTORY TAKING
On pages 37 and 38 you will find a record sheet for taking a
child’s history. You can use it as a guide for the kinds of questions it is
important to ask. (Of course, some of the questions will apply more to some
children than others, so ask only where the information might be helpful.)
When asking questions, we rehabilitation workers must always
remember that parents and family are the only real ‘experts’ on
their child. They know what she can and cannot do, what she likes and does
not like, in what ways she manages well, and where she has difficulties.
However, sometimes part of the parents’ knowledge is
hidden. They may not have put all the pieces of knowledge together to form a
clear picture of the child’s needs and possibilities. The suggestions in
this chapter, and the questions on the RECORD SHEETS, may help both
rehabilitation workers and parents to form a clearer picture of their
child’s needs and possibilities.
|
Rehabilitation workers and parents can work together to
figure out the child’s needs. |
EXAMINING THE DISABLED CHILD
After finding out what we can by asking questions, our next step
is to examine the child. In as friendly a way as possible, we carefully observe
or test what parts of the child work well, what parts work poorly, and how this
affects the child’s ability to do things and respond to the world around
him.
|
CAUTION: Although we sometimes examine separately
different aspects of the child’s body and mind, our main purpose is to
find out how well the child’s body and mind work together as a whole: what
can the child do and not do, and why? This information helps us decide how
to help the child to do things better. |
In examination of a disabled child, we may check on many things:
· The senses:
How well does the child see?  hear?
hear?  feel?
feel? 
· Movement: How well does
the child move or control her movements? 
· Form and structure: How
well formed, deformed, or damaged are different parts of the body: the joints,
 the backbone,
the backbone,  and skin?
and skin? 
· Mind, brain, and nervous
system: How much does the child understand? How well do different parts of
the body work together? For example, balance or eye-to-hand coordination. 
· Developmental level:
How well does the child do things, compared to other local children her
age?
In addition, a complete physical examination would
include checking the health of systems inside the body. Although this
part of the examination, if needed, is usually done by health workers,
rehabilitation workers need to know that with certain disabilities inner body
systems may also be affected. Depending on the disability, these may include:
|

|
the breathing system (respiratory system) |

|
the body’s cleaning system (urinary tract) |

|
the heart and blood system (circulation system) |

|
the food processing system (digestive system) |
|
Rehabilitation workers need to work in close cooperation
with health workers. |
A detailed examination of all a child’s parts
and functions could take hours or days. Fortunately, in most children this is
not necessary. Instead, start by observing the child in a general way.
Based on the questions you have already asked and your general observations, try
to find anything that seems unusual or not quite right. Then examine
in detail any body parts or functions that might relate to the disability.
Part of the art of examining a child is KNOWING WHEN TO
STOP. It is important to check everything that might help us understand the
child’s needs. But it is equally important to win the child’s
confidence and friendship. Too much examining and testing can push any child to
the point of fear and anger. Some children reach their limit long before others.
So we must learn how much each child can take - and try to examine the child in
ways that she accepts.
Some children require a much more complete examination than
others. For example:
|
Juan lost one hand in an accident 2 years ago, but otherwise
seems normal. Probably he will need little or no physical examination other than
to see how he uses his arms, stump, and hand. You will also want to check how
much he can do with his other hand, with only his stump, and when using both
together.

Figure
The Physical Examination Form (RECORD SHEET 2) is probably the
only examination form you need to fill out.
However, it would be wise to learn about how Juan’s family
and others treat him now, and how he feels about himself and his ability to do
things. Does he keep his stump hidden when he is with strangers? With family
members? What are his hopes and fears? You can write this information on the
back of the form. |
|
Ana is 2 years old and still does not sit by herself. She has
strange uncontrolled movements. She does not play with toys or respond much to
her parents.

Figure
Ana seems to have many problems.
We will need to check:
· how well she sees
and hears.
· how strong, weak, or stiff
different parts of her body are.
· in what
ways her development is slow (what she can do and not do).
· how much she understands.
· signs of brain damage, and how severe.
· her sense of balance and position.
· what positioning or support gives her better control
and function.
It may take weeks or months of repeated examining and testing to
figure out all of Ana’s difficulties, and how to best help her to function
better. It could be a mistake to try to do all the needed examining at one time.
To record all the useful information on a child like Ana, you
will find RECORD SHEETS 1, 2, 3, 4, and 6 helpful. |
Examining techniques: Winning the child’s confidence
Depending on how you go about it, the physical examination can
help you become a child’s friend or turn you into his enemy. Here are a few
suggestions:
· Dress as one of
the people, not as a professional. White uniforms often scare a child -
especially if at some time he was injected by a nurse or doctor.
· Before starting the
examination, take an interest in the child as a person. Speak to him in a
gentle, friendly way. Help him relax. Touch him in ways that show you are a
friend.
· Approach the child from the
same height, not from above. (Try to have your head at the same level as his.)
· Start the examination with the
child sitting or lying on mother’s lap, on the floor, or wherever he
feels most safe and comfortable.
Figure
· If the child seems
nervous about a stranger touching or examining her, have the parent do as
much of it for you as possible. This will let the mother know that you
respect and want to include her. And she may learn more.

Figure
· Make the waiting
area and place where you do the examining as pleasant and as much like
home as you can. Have lots of toys, from very simple to complex, where the
children can choose and play with them. By watching if, how, for how long,
with what, and with whom a child plays, you can learn a lot about what a
child can and cannot do, his level of physical and mental development, the types
of problems he has, and the ways he has (or has not yet) adapted to
them.

Figure
|
|
Watching how a child plays - by herself, with people, and
with toys - is an essential part of evaluating the child. |

|
· Try to make the
examination interesting and fun for the child. Turn it into a game whenever
possible. For example:
When you want to test a child’s
‘eye-to-hand coordination’ (for possible balance problems or brain
damage) you might make a game out of having the child touch the nose of a doll.
Or have her turn on a flashlight (torch) by pushing its
button

Figure
Also, when he begins to get restless,
stop examining for a while and play with him, or let him
rest.
|

|
It is best to examine a child when he is well-rested,
well-fed, and in a ‘good mood’ - and when you are, too.
(We know this will not always be possible.) |
· When a child is
weaker or has less control on one side than the other, (a) first test the
stronger side, (b) and then the weaker side.
Figure (a)
Figure (b)
By testing the good side first, you start by giving
the child encouragement with what he can do well. Also, if the child does not
move the weaker side, you will know it is because he cannot, and not because he
does not understand or is not trying.
· As you examine the child,
give her lots of praise and encouragement. When she tries to do something
for you and cannot, praise her warmly for trying.

Figure
Ask her to do things she can do well and not just
the things she finds difficult, so that she gains a stronger sense of
success.
TESTING RANGE OF MOTION OF JOINTS AND STRENGTH OF MUSCLES
Children who have disabilities that affect how they move often
have some muscles that are weak or ‘paralyzed’.
As a result, they often do not move parts of their bodies as much as is normal.
Loss of strength and active movement may in time lead to a
stiffening of joints or shortening of muscles (contractures, see
Chapter 8). As a result, the affected part can no longer be moved through
its complete, normal range of motion.
|
ACTIVE MOVEMENT |
PASSIVE MOVEMENT |
|
|
|
|
|
Normally the shoulder muscles can raise the arm until it is
straight up.

Figure
Lifting the arm like this with the arm’s own muscles is
called ACTIVE MOTION. |
When the shoulder muscles are paralyzed, the child can no longer
actively lift his arm.

Figure
|
At first the paralyzed arm can be lifted straight up with help.
This is called PASSIVE MOTION.

Figure
|
Unless the normal range of motion is kept through daily
exercises, the passive range of motion will steadily become less and less.

Figure
Now the arm cannot be raised straight up, even with help. |
In the physical examination of a child with any weakness or
paralysis of muscles, or joint pain, or scarring from injuries or burns, it is a
good idea to test and record both RANGE OF MOTION and MUSCLE STRENGTH of all
parts of the body that might have contractures or be affected. There are 2
reasons for this:
· Knowing which
parts of the body have contractures or are weak, and how much, can help us to
understand why a child moves or limps as she does. This helps us to decide
what activities, exercises, braces, or other measures may be useful.
· Keeping accurate records of
changes in muscle strength and range of motion can help tell us if certain
problems are getting better or worse. Regular testing therefore helps us
evaluate how well exercises, braces, casts, or other measures are working,
and whether the child’s condition is improving, and how
quickly.
For testing range of motion and muscle strength, it helps to
first know what is normal. You can practice testing non-disabled, active
persons. They should be of the same ages as the disabled children
you will test. Age matters because babies are usually weaker and have much more
flexible joints than older children. For example:
|
|

|

|

|
|
A baby’s back and hips bend so much he can lie across his
straight legs. |
A young child bends less but can usually touch his toes with his
legs straight. |
Around 11 to 14 it is harder to touch toes. His legs grow faster
and become longer than his upper body. |
Later, upper body growth catches up with legs. He can again
touch toes more easily. |
In different children (and sometimes in the same child) you may
need to check range of motion and strength in the hips, knees, ankles, feet,
toes, shoulders, elbows, wrists, hands, fingers, back, shoulder blades, neck,
and jaw. Some joints have 6 or more movements to test: bending, straightening,
opening, closing, twisting in, and twisting out. See, for example, the different
hip movements (range-of-motion exercises) in Chapter 42.
To test both ‘range of motion’ and
‘strength’, first check ‘range of motion’. Then you will
know that when a child cannot straighten a joint, it is not just because of
weakness.
Range-of-motion testing: Example:
|
Knee |
|
|
|
|
|
1. Ask the child to straighten it as much as she can. |

Figure
|
2. If she cannot straighten it all the way, gently see how far
you can straighten it without forcing. |
With your hands, support the joint on each side as you
straighten it. |
|
|
|

Figure
|
|
3. If at first the joint will not
straighten, keep trying with gentle continuous pressure for 2 or 3
minutes. |

Figure
|
If it still does not straighten, the range of motion is reduced.
This is usually because of a contracture (see Chapter 8). |
|

Figure
|
If it gradually straightens, spasticity (muscle
spasms) may be what makes it difficult. (If it stops before it straightens
completely, contractures may also be developing.) |
|
4. If a joint will not straighten completely, try with the
child in different positions. |

Figure
|
For example, a knee often does not straighten as much with the
hips bent as with the hips straight. |
Figure
|
For this reason, each time you test range of motion to measure
changes, be sure the child is in the same position. |
|
Position affects how much certain joints
straighten or bend. This is true in any child, but especially in a child with
spasticity. |
|
5. In addition to checking how much a joint straightens,
check how much it bends. |

Figure
|
If joints are kept straight and never bent, they may stiffen or
develop contractures that do not let them bend. (This can happen with joint
infection, arthritis, and other conditions, or when a joint is kept in a cast
for a long time.) |
|
6. Also check for too much range of motion. |
A child who walks on a weak leg often ‘locks’ her knee
backward to keep from falling. In time, the knee stretches back more and more,
like this. |

Figure
|
The same thing can happen to the child with weak arms who uses
crutches (or crawls). |
Usually the best positions for checking range of motion are the
same as those for doing range-of-motion and stretching exercises. These are
shown in Chapter 42.
For methods of measuring and recording range of motion, see
Chapter 5.
Precautions when testing for contractures
Testing range of motion of the ankles, knees, and
hips is important for evaluating many disabled children. We have already
discussed knees. Here are a few precautions when testing for contractures of
ankles and hips.
Ankle
|

Figure
|
Test the range of motion with the knee as straight as it will
go. |
With the knee bent, the foot will usually bend up more. But for
walking, we need to know how far it bends with the knee straight. |
|

Figure
|

Figure
|
|
Note: To check ankle range
of motion in a child with spasticity: |
|
With his body and knee straight, it may be hard to bend the
ankle. |
So first bend his neck, body, and knees and then slowly bend up
the ankle. |
Then slowly straighten his knee while keeping the ankle bent.
|
|

Figure
|

Figure
|

Figure
|
|
Other precautions for testing ankle range of motion are in
Chapter 42 |
Hip
To check how far the hip joint straightens, have the child hold
his other knee to his chest, like this, so that his lower back is flat against
the table. If his thigh will not lower to the table without the back lifting, he
has a bent-hip contracture.
Figure
|
CAUTION The hips will often straighten more at an
angle to the body. So be sure to lower the leg in a straight line with the body,
or you can miss contractures that need to be corrected before the child can
walk.

Figure
|
Muscle testing
Muscle strength can be anywhere between normal and
zero. Test it like this:
|
If the child can lift the weight of leg all the way, press down
on it, to check if she can hold up as much weight as is normal for a girl her
age. If she can, her strength is NORMAL.

Figure
|
If she can hold some extra weight, but not as much as is
normal, she rates GOOD.
Figure
|
|
|
|
|
If she can just hold up the weight of her leg, but no added
weight, she rates FAIR.

Figure
|
If she cannot hold up the weight of her leg, have her lie on her
side and try to straighten it. If she can, she rates POOR.

Figure
|
If she cannot straighten her knee at all, put your hand over the
muscles as she tries to straighten it. If you can feel her muscles tighten, rate
her TRACE.

Figure
|
Test the strength of all muscles that might be affected. Here
are some of the muscle tests that are most useful for figuring out the
difficulties and needs of different children.
|
Note: These tests are simple and mostly test the
strength of groups of muscles. Physical therapists know ways to
test for strength of individual muscles. |
Ankle and Foot

Figure
Note: Sometimes when the muscles that normally
lift the feet are weak, the child uses his toe-lifting muscles to lift his foot.
|
If he lifts his foot with his toes bent up, like this, |
see if he can lift it with his toes bent down, like this. |
|

Figure
|

Figure
|
Also notice if the foot tips or pulls more to one side. This may
show ‘muscle imbalance’.
If the child can walk, see if she can stand and walk on her
heels and her toes.

Figure
|
EXAMPLES OF REASONS FOR TESTING |
|
1. If strength to lift up the foot is WEAK and strength to push
down is STRONG, tiptoe contractures may develop - unless steps are taken to
prevent them. |

|
|
2. An ankle with POOR or very uneven strength may be helped by
an ankle brace. But if strength is FAIR, exercise may strengthen it - and a
brace may weaken it more! |

|
|
3. Lifting the foot with only the toe muscles may lead to a
high-arch deformity. |

|
|
To learn about which muscles move body parts in different
ways, as you test muscle strength, feel which muscles and cords tighten.
|
Knee

STRAIGHTEN
You can fell the muscle tighten on top of the thigh (1).

BEND
Feel the muscles tighten on the back of the thigh (2).
Feel the tight cords pull here (3).
|
EXAMPLES OF REASONS FOR TESTING |
|
|

BEND
|
1. POOR or NO strength for straightening knee may mean an
above-knee brace is needed. |
|
2. Stronger muscles in back of the thigh than in front can lead
to a bent-knee contracture. |

Figure
|
Hips

OPENING

CLOSING
ROTATING HIP OUT (and leg in)
ROTATING HIP IN (and leg out)

BENDING

STRAIGHTENING
If the hip has contractures, test
with legs off end of table.

SIDEWAYS LIFT
Note: Weak hip muscles sometimes lead to
dislocation of the hip. Be sure to check for this, too.
Testing side-of-hip muscles is important for evaluating why a
child limps or whether a hip-band may be needed on a long-leg brace.
|
TEST FOR WEAK SIDE-OF-HIP MUSCLES IN THE CHILD WHO CAN
STAND
Have the child stand on the weaker leg. |
|
NORMAL |
NOT NORMAL |
|
The child stands straight. The hip tilts up on the lifted
leg.

Figure
|
The hip tilts down on the lifted side.
Figure
|
Or the child shifts his whole weight so it balances over the
weak hip.

Figure
This child dips to the side on each step of the weak leg. (This
is often seen with polio.) |
|
Note: Dipping to one side when walking is
caused more by weak side-of-hip muscles than by a shorter leg. But a shorter leg
can make dipping worse. |
Stomach and Back
To find out how strong the stomach muscles are, see if the child
can do ‘sit ups’ (or at least raise his head and chest).
To test the back muscles, see if he can bend backward like this.
|
Sitting up with knees bent uses (and tests) mainly the stomach
muscles. Feel stomach muscles tighten. |
Sitting up with knees straight uses the hip-bending muscles and
stomach muscles. |
Feel the muscles tighten on either side of the backbone. Notice
if they look and feel the same or if one side seems stronger. |
|

Figure
|

Figure
|

Figure
|
You can check a child’s trunk control and
strength of stomach, back, and side muscles like this. Have him hold his
body upright over his hips, then lean forward and back, and side to side, and
twist his body.

Figure
If a child’s stomach and back muscles are weak, he may need
braces with a body support - or a wheelchair.

Figure
|
IMPORTANT: Be sure to check for
curvature of the spine - especially in children with muscle imbalance or
weakness of the trunk. |
Shoulders, Arms, and Hands
When a child’s legs are severely paralyzed but she has FAIR
or better trunk strength, she may be able to walk with crutches if
her shoulders, arms, and hands are strong enough.
Therefore, an important test is this.
Can she lift her butt off the seat like this?
Figure
If she can, she has a good chance for walking with crutches.
If she cannot lift herself, check the strength in her shoulders
and arms:

Figure
If the shoulder pushes down strongly but her elbow-straightening
muscles are weak, she may be able to use a crutch with an elbow support.

Figure
Or, if her elbow range of motion is normal, she may learn to
‘lock’ her elbow back like this. However, this can lead to elbow
problems.

Figure
You may want to make a chart something like this and hang it in
your examining area, as a reminder.
|
EVALUATING STRENGTH OR WEAKNESS OF MUSCLES |
|
CAUTION: To avoid misleading results, check range of
motion BEFORE testing muscle strength. |
|
|
Strength rating |
|
Test with the child positioned so that he lifts the weight of
the limb. |
|
In muscle testing, it is especially important to note the
difference between FAIR and POOR. |
Strong enough to be useful. |
NORMAL
(5) |
lifts and holds against strong resistance |

Figure
|
|
|
GOOD
(4) |
lifts and holds against some resistance |

Figure
|
|
|
FAIR
(3) |
lifts own weight but no more |

Figure
|
|
|
|
|
Test with the child positioned so that he can move the limb
without lifting its weight (by lying on his side). |
|
This is because FAIR is often strong enough to be fairly useful
(for standing, walking, or lifting arm to eat). POOR is usually too weak to be
of much use. |
Too weak to be of much use for lifting or bearing weight. |
POOR
(2) |
cannot lift own weight but moves well without any weight |

Figure
|
|
|
TRACE
(1) |
barely moves |

Figure
|
|
|
ZERO
(0) |
no sign of movement |

Figure
|
Sometimes with exercise POOR muscles can be strengthened to
FAIR; this can greatly increase their usefulness. It is much less common for a
TRACE muscle to increase to a useful strength (FAIR), no matter how much it is
exercised. (However, if muscle weakness is due to lack of use, as in severe
arthritis, rather than to paralysis, a POOR muscle can sometimes be strengthened
with exercise to GOOD or even NORMAL. Also, in very early stages of recovery
from polio or other causes of weakness, POOR or TRACE strength sometimes returns
to FAIR or better.)
Other things to check in a physical examination
Difference in leg length. When one leg is weaker, it
usually grows slower, and becomes shorter than the other leg. An extra thick
sole on the sandal might help the child stand straighter, limp less, and avoid
curving of the spine. A short leg may also be a sign of a dislocated hip. So it
helps to check for, and to measure, difference in leg length.
|
If the child can stand, |
|
Figure
|
look for a tilt of the hip bones, |
|
|
then raise the foot of the short leg until the hips are level.
|

Figure
|
|
|
|
and measure the difference |
|
|
If she cannot stand, |
|
have her lie as straight as she can. Feel and then mark, on both
sides of her body, the bony lumps |
|
at the top front corner of the hip bone |
and on the inner ankle. |
|
|

Figure
|
Pass tape along inner side of knee. |
|
Then measure from here to here with a tape measure or string.
Measure each leg and record the difference. If you used a string, just draw
lines on your record sheet showing the actual difference in leg length. |

Figure
|
Curve of the spine
Especially when one leg is shorter or there are signs of muscle
imbalance in the stomach or back, be sure to check for abnormal curve of the
spine (back bone). The 3 main types of spinal curve (which may occur separately
or in combination) are:
|
Sideways curve (scoliosis) |
|

Figure
|
shoulder higher on side of short leg
Check for weaker muscles on this side of spine. |
Figure
|
Have the child bend over. Check for a rib hump on outer side of
curve. |
|
Hunch back, rounded back (kyphosis) |
|
May result from weak back muscles, or poor posture. |

Figure
|
|
Sway back (lordosis) |
|

Figure
|
May result from weak stomach muscles or bent-hip contractures.
(Be sure to check for these.) |
Some spinal curves will straighten when a child changes her
position, lies down, or bends over. Other spinal curves will not straighten, and
these are usually more serious. For more information about examining spinal
curve and deformities of the back, see Chapter 20.

Normal position of spine showing
the 3 main divisions of the backbone.
EXAMINING THE NERVOUS SYSTEM
Sometimes physical disability results from problems in the
muscles, bones, or joints themselves. But often it comes from a problem in, or
damage to, the nervous system.
Depending on what part of the nervous system is affected, the
disability will have different patterns.
For example, polio affects only certain action
nerves at points in the spinal cord (or brain stem). It therefore affects
movement. It never affects sensory nerves, so sight, hearing, and feeling
stay normal. (See Chapter 7.)
|
THE NERVOUS SYSTEM
The nervous system is the body’s communication
system. The ‘central switchboard’ is the brain, from which electrical
messages run back and forth, to all parts of the body, through ‘wires’
called nerves.
Sensory nerves bring messages from parts of the body
about what the body sees (eyes), hears (ears), smells (nose), and feels (skin).
Action nerves (motor nerves) carry messages to parts of
the body, telling muscles to move.

Figure
The brain (1) is the main control center of the nervous
system.
The ‘trunk line’ (2) of the nerves is the spinal cord.
It runs from the brain down the middle of the spine. Nerves come out from
between each back bone and communicate to a part lower down in the body. |
A spinal-cord injury, however, can damage or cut both the
sensory and action nerves, so that both movement and feeling are lost. (See
Chapter 23.)
Unlike polio and spinal-cord injury, which come from damage to
nerves in the spine, cerebral palsy comes from damage to the brain
itself. Because any part or parts of the brain may be damaged, any or all parts
of the body may be affected: movement, sense of balance, seeing, hearing,
speech, and mental ability. (See Chapter 9.)
Therefore, how completely you examine the workings of the
nervous system will depend partly on what disability the child appears to have.
If it is fairly clear the disability comes from polio, little examination of the
nervous system is needed. But sometimes polio and cerebral palsy can be
confused. If you have any suspicion that the disability might be caused by brain
damage, you wilt want to do a fairly complete exam of nervous system
function. Damage to the brain or nervous system can cause problems in any of
these areas:
· seeing (See
Chapter 30.)
· eye movement or position
· fits or seizures (epilepsy)
(See Chapter 29.)
· balance, coordination, and
sense of position
· hearing (See Chapter 31.)
· use of mouth and tongue, and
speech
· mental ability; level of
development
· feeling (pain and touch)
· unusual or strange behaviors;
signs of self-damage
· muscle tone (patterns of
unusual floppiness, tightness, spasms, or movements). (See Chapter 9.)
· reflexes; muscle jerks
· urine and bowel control (See
Chapter 25.)
Methods for testing some of these things are included on the
next few pages and on the RECORD SHEETS 2, 3, and 4. Other tests that you will
need less often, we include with specific disabilities. Refer to the page
numbers listed above.
EVALUATION OF A CHILD WHOSE DEVELOPMENT IS SLOW
For the child who cannot do as much as other children do at the
same age, a special developmental evaluation may be helpful. Additional
information about the child’s mother during pregnancy, or any difficulties
during or after birth may explain possible causes. Measurement of the distance
around the head may show possible causes of problems or other important factors.
Repeated head-size measurements (once a month at first) may tell us even more.

For example, a child who has had meningitis (brain infection) at
age 1, and whose head almost stops growing from that age on, will probably
remain quite retarded. We should not expect a lot. However, if the child’s
head continues to grow normally, the child may have better possibilities for
learning and doing more (although we cannot be sure).

A child who is born with a ‘sack on the back’ (spina
bifida) may have a head that is bigger than average. If the head continues to
grow rapidly, this is a danger sign. Unless the child has surgery, she may
become severely retarded or die. If, however, the monthly measurements show that
the head has stopped growing too fast, the problem may have corrected itself.
She may not need surgery.
RECORD SHEET 4, on page 41, covers additional questions relating
to child development, and includes a chart for recording and evaluating head
size.
To help the child who is developmentally delayed, you will
first want to evaluate her level of physical and mental development. Chapter 34
explains ways to do this.
You can use the Child Development Chart on pages 292 and 293 to
find a child’s developmental level, to plan her step-by-step activities,
and to evaluate and record her progress. We have marked this 2-page chart,
RECORD SHEET 6.
RECORD SHEETS
On the next 5 pages are the sample RECORD SHEETS that we
discussed. You are welcome to copy and use them. However, they are not perfect.
They were developed for use by the village rehabilitation team in Mexico, and we
are still trying to improve them. Before you make copies, we suggest that you
adapt them to meet the needs of your area.
|
Be sure you have copies made of the RECORD SHEETS you will
need before you need to use them. |
In addition to the 4 RECORD SHEETS here, you may also want
copies of RECORD SHEET 5 “Evaluation of Progress,” page 50, and RECORD
SHEET 6, “Child Development Chart,” pages 292 and 293.
|
Note on RECORD SHEET 1 (CHILD
HISTORY):
The box at the top of RECORD SHEET 1 is to be filled out
after you examine the child. It gives brief, essential
information. This will make it easier to find out which disabilities you have
seen most often, and to check on what you still need to do for different
children.
The last few questions on page 2 of RECORD SHEET 1 are for a
study PROJIMO is doing on medical causes of disability. Adapt them to study
special concerns in your area. |

RECORD SHEET 1 (page 1)
RECORD SHEET 1 (page 2)

RECORD SHEET 2

RECORD SHEET 3

RECORD SHEET 4

Figure
Chapter 5: Simple Ways to Measure and Record a Child’s Progress
It is important to keep records of each child’s progress.
Careful records help workers and parents to follow the change in the
individual child, and to evaluate the effectiveness of advice, therapy, and
aids.
We need a clear view of the progress of the whole child in
all areas - physical, mental, and social. The Child Development Chart will
help us to do this for younger children. For children over 5, at the end of this
chapter there is a simple chart (RECORD SHEET 5) for evaluating a child’s
increasing ability to do things.
When the parents and child themselves regularly measure and
record a child’s progress, they become more aware of gradual improvements.
This encourages them to continue with important exercises, aids, and activities.
Unfortunately, the standard way of recording physical
deformities and contractures requires knowledge of angles,
degrees, and symbols that many people do not understand. For evaluation to
become a family tool, we need a way to measure, record, and interpret
information that is as simple, clear, and enjoyable as possible. Here are
some ideas.
MEASURING JOINT POSITIONS AND CONTRACTURES
You can make a simple measuring tool using 2 flat pieces of
wood, plastic, or cardboard. (Tongue depressors work well.)
Other simple methods for recording joint positions are in
Chapter 9.
1. Rivet the pieces together on one end.

Figure
2. Line them up exactly with the joint.

Figure
3. Trace the angle on paper.
Figure
4. Do this again every 1 or 2 weeks to see if the joint is
straightening with exercise.
Figure
The ‘flexikin’ - an aid to measure and encourage
progress
Flexikins are cardboard dolls with joints. Disabled and
non-disabled children can make and play with them. They are so easy to use
that even parents who cannot read can measure and record their children’s
contractures. Because the periodic measurements are recorded as a line of
pictures, anyone can see the child’s progress at a glance.
Flexikins - front and side view
models
We have found that when families follow their child’s
progress using flexikins, both the child and parents are more likely to keep
doing stretching exercises. As a result, many contractures can be partly or
completely straightened in the home, and there is less need for casting and
surgery.

Children making and playing with
flexikins. In the PROJIMO village rehabilitation center, all the flexikins used
are made by disabled children and the local school children.
Examples of how flexikins are used
|

Figure

Figure
Village rehabilitation workers have just made a brace for a
child with polio whose leg bends back severely. They want to know if the leg
will gradually get better (bend back less). So they ask the mother to measure it
every month. |
|

Figure
The mother places the flexikin’s leg in the same position
as her son’s leg, bent back as far as it goes. She then traces it onto a
large sheet of paper.

Figure
|

Figure
Each month she does the same and records the date. (In April her
son did not use the brace for 2 weeks and she saw the knee was getting worse.
This convinced both mother and boy of the importance of using the brace.)
The flexikins can be used to record a wide variety of positions,
deformities, contractures, and limitations in range of motion, mainly of the
arms and legs but also of the neck, back, hips, and body:

Figure

Figure

Figure

Figure
Figure
You can draw both arms and legs. First one and the other, like
this:

Figure

Figure
In addition to using the small flexikins for record keeping, you
can make large flexikins for group teaching. Or use them to keep body
proportions correct when making drawings for instruction sheets.
|
Note: For recording contractures, we have found
the side-view flexikin more useful than the front-view one. The side-view
flexikin is also easier to make. It is probably the only one you will need for
evaluating a child’s progress. |
How to make the flexikins
1. Trace the patterns of different pieces onto very thick paper
or thin, firm cardboard. Or use old X-ray film.
You can do this using carbon paper. (Make your own
carbon paper by completely blackening a sheet of paper with a soft-leaded
pencil.)
 Or you can glue a copy of the
pattern sheet directly to the cardboard.
Or you can glue a copy of the
pattern sheet directly to the cardboard.
Figure
(If your program plans to make many flexikins, or have children
make them, we suggest you have the patterns printed or mimeographed directly on
sheets of thin, firm cardboard.)
2. Cut out the pieces with strong scissors, shears, or a piece
of razor blade.

Figure
3. Place the pieces together as shown in the drawings. Make sure
the pieces that overlap with dotted lines go behind those with complete lines.

Figure

Figure
4. Fasten the pieces together at the black dots with rivets,
pins or thread.
Use the smallest rivets you can find.

Figure
Or string the joints together with thread or yarn (this does not
work as well).

Figure
Or use thin wire or string and tie knots.
Figure
Or use sewing pins;

Figure
Rivets usually work best. First punch a hole through each
black dot. Put the rivets through and hammer them just enough so that the
cardboard joints are tight enough to hold their positions but can be moved
without tearing.
You can copy this sheet, or one like it, and give it to parents
together with a flexikin. Be sure that you also show them how to use it
and then watch them use it.
|
INSTRUCTIONS FOR USING THE FLEXIKIN |
|
We have given you a ‘flexikin’ so that you can measure
and see the progress that your child is making with his exercises or aids. |
|
We suggest you take a new measurement every
_____________________________________ |
|
Do it like this: |
|
1. Have your child take the position you want to measure (for
example, straighten his knee as much as he can). |

Figure
|
|
2. Put the flexikin in exactly the position the child is in. To
do this hold the flexikin at a distance between your eye and the child so
that it appears the same size as the child. This will let you line it up
exactly. |
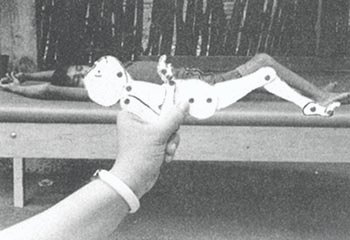
Figure
|

Figure
|
|
3. Without moving the position of the flexikin, trace it onto a
large piece of paper. The first time trace the whole body. Each time measure the
child in the same posture. |

Figure
|
This example shows how exercises have helped straighten a
contracted knee. |
|
For later recordings, you only need to trace the part or parts
you are measuring. Each time you record a measurement, write the date. |
|
In certain cases you may want to measure how far the child can
straighten an arm or leg by herself, and how far you are able to straighten it
for her (little by little without forcing). |
Make 2 columns. In one, record how far the child can move it by
herself. In the other column record how far she can move it with help. |

Figure
|
|

Figure
|
Here you see the progress of a leg until it became straight and
a brace could be made for it. |
|

SIDE-VIEW FLEXIKIN - Patterns of
pieces for making it
FRONT-VIEW FLEXIKIN - Patterns of
pieces for making it
EVALUATING THE PROGRESS OF THE WHOLE CHILD
A simple way for rehabilitation workers and parents to evaluate
how a child is progressing as a whole is to keep a record of her ability to do
different things. Each month, or during each visit to the community
rehabilitation center, the child’s different abilities are reviewed,
tested, or observed. Any changes are recorded.
For children under 5 years old, one way of evaluating a
child’s development is to use the RECORD SHEET 6. This chart shows the
developmental levels (‘milestones’) for different skills and
activities. The first time the child is evaluated, circle the drawing that shows
what the child can do in each area.
Each time the child is evaluated, on the same sheet, again
circle the appropriate drawing, but use a different color (or a dotted,
dashed, or zigzag line). This way, you can see where the child is moving ahead
well and where he is behind.

Figure
For evaluating the progress of children over age 5, the charts
on the next page may help. Two different approaches are used. Chart A is more
objective (requires less personal judgment or opinion) but does not allow
for small improvements. Chart B is more subjective (is based more on
personal judgments). It considers quality of improvement, not just
quantity. You can try both and see which you think gives truer, more useful
results.
To use Chart A: For each skill, circle whether the child
can do it “without help,” “with a little help,” or
“with lots of help.” Add all the numbers you circle. Compare the
scores of the first and second visits. For example:
|
First visit |
Second visit |
|
without help |
little help |
lots of help |
without help |
little help |
lots of help |
|
How does the child eat? |
4 |

|
0 |

|
2 |
0 |
|
How does the child drink? |
4 |
|
0 |
4 |
|
0 |
Here we see the child has improved his eating skills but not his
drinking skills.
To use Chart B: In each area, on the second visit, circle
whether the child is doing a lot better, a little better, or the same. Add it
all up. The higher the score, the more the child has improved.
|
NOTE: We question whether the use of
numbers may not be misleading. But we think the questions themselves may be a
useful guideline. None of these evaluation forms will show all areas of change
or improvement. They are not substitutes for detailed notes, drawings,
and a good memory! |

RECORD SHEET
5
B. Recognizing, Helping with, and Preventing Common Disabilities
Chapter 6: Guide for Identifying Disabilities
This chapter has a chart, 7 pages long, to help you find out
what disability a child possibly has, and where to look up that
disability in this book.
In the first column of the chart, we list the more
noticeable signs of different disabilities. Some of these signs are found in
more than one disability. So in the second column we add other signs that
can help you tell apart similar disabilities. The third column names the
disability or disabilities that are most likely to have these signs. And the
fourth column gives the page numbers where you should look in this book.
(Where it says WTND and then a number, this refers to the page in
Where There Is No Doctor.)
If you do not find the sign you are looking for in the first
column, look for another sign. Or check the signs in the second column.
This chart will help you find out which disabilities a child
might have. It is wise to look up each possibility. The first page of each
chapter on a disability describes the signs in more detail.
|
IMPORTANT: Some disabilities can easily be
confused. Others are not included in this book. When you are not sure, try to
get help from someone with more experience. At times, special tests or X-rays
may be needed to be sure what the problem is. |
Fortunately, it is not always necessary to know exactly what
disability a child has. For example, if a child has developed weakness in
his legs and you are not sure of the cause, you can still do a lot to help him.
Read the chapters on disabilities that cause similar weakness, and the chapters
on other problems that the child may have. For this child, you might find useful
information in the chapters on polio, contractures, exercises,
braces, walking aids or wheelchairs, and many others.
Sometimes it is important to identify the specific
disability. Some disabilities require specific medicines or foods - for
example, night blindness, rickets, or cretinism. Others urgently need surgery -
for example, spina bifida or cleft lip and palate. Others require special ways
of doing therapy or exercises - for example, cerebral palsy. And
others need specific precautions to avoid additional problems - for example,
spinal cord injury and leprosy. For this reason, it helps to learn as much about
the disability as you can. Whenever possible, seek information and advice from
more experienced persons. (However, even experts are not always right. Do not
follow anyone’s advice without understanding the reasons for doing
something, and considering if and why the advice
applies to the individual child.)

In addition to this chart, 2 other guides for identifying
disabilities are in this book:
GUIDE FOR IDENTIFYING CAUSES OF JOINT PAIN
GUIDE
FOR IDENTIFYING AND TREATING DIFFERENT FORMS OF FITS (EPILEPSY)
GUIDE FOR IDENTIFYING DISABILITIES
SIGNS PRESENT AT OR SOON AFTER BIRTH
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
born weak or ‘floppy’

Figure
slow to begin to lift head or move arms

Figure
|
· often a difficult
birth
· delayed breathing
· born blue and limp
· or born before 9 months and very small |
· cerebral palsy
· developmental delay |
|

Figure
· round face
· slant eyes
· thick
tongue |
· Down syndrome
(mongolism)
· cretinism |
|

Figure
small head, or small top part of head |
microcephalia (small brain) mental retardation |
|
none of above |
developmental delay for other reasons |
|
does not suck well or chokes on milk or food

Figure
|
· pushes milk back out with
tongue
· or will not suck |
cerebral palsy |
|
· cannot suck well
· chokes or milk comes out nose |
· check for cleft palate

Figure
· possibly severe retardation
|
|
one or both feet turned in or back
Figure
|
no other signs |
club foot |
|
· hands weak, stiff or
clubbed
· some joints stiff, in bent or
straight positions

Figure
|
arthrogryposis |
|
dark lump on back |
spina bifida |
|
‘bag’ or dark lump on back

Figure
|
· clubbed feet
· or feet bend up too far

Figure
· or feet lack movement and
feeling |
spina bifida (sometimes no ‘bag’ is seen, but foot
signs may be present) |
|
head too big: keeps growing
Figure
|
may develop:
· eyes like ‘setting
sun’

Figure
· increasing mental and/or
physical disability
· blindness |
hydrocephalus (water on the brain)
At birth, this is usually a sign of spina bifida.
in an older child, possibly tapeworm in brain, or a brain tumor
|
|
upper lip and/or roof of mouth incomplete

Figure
|
· difficulty feeding
· later, speech difficulties

Figure
|
cleft lip (hare lip) and cleft palate |
|
birth deformities, defects, or missing parts

Figure
|
(may or may not be associated with other problems) |
See
· birth defects
· amputations
· Down
syndrome
· developmental delay |
|
abnormal stiffness or position

Figure
|
· from birth
· some muscles weak
· some joints stiff
· head control and mind normal |
arthrogryposis
Figure
|
|
· Muscles tighten more in
certain positions.
· may grip thumb tightly

Figure
|
spastic cerebral palsy
Note: muscle tightness (spasticity) usually does
not appear until weeks or months after birth. |
|
one arm weak or in strange position

Figure
|
does not move the arm much

Figure
|
Erb’s palsy (weakness from damage to nerves in shoulder
during birth) |
|
leg on same side often affected |
hemiplegic (one-sided) cerebral palsy |
|
dislocated hip at birth

Figure
|
On opening legs like this, leg ‘pops’ into place or
does not open as far.

Figure

Figure
|
dislocated hip from birth (often both hips)
may be present with:
· spina bifida
· Down syndrome
·
arthrogryposis |
|
slow to respond to sound or to look at things

Figure
|
(may be due to one or a combination of problems) |
Check for signs of:
· developmental delay
· cerebral palsy
·
blindness
· deafness |
SIGNS IN CHILDREN
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
slower than other children to do things (roll, sit, use hands,
show interest, walk, talk)
Figure
|
slow in most or all areas: |
Developmental delay, check for signs of: |
|
· round face
· slant eyes
·
single deep crease in hand
Figure
|
Down syndrome (mongolism) |
|
· movements and response
slow
· skin dry and cool
· hair often low on forehead
· puffy eyelids

Figure
|
cretinism |
|
has continuous strange movements or positions, and/or stiffness
Figure
|
cerebral palsy also check for:
· blindness
· deafness
·
malnutrition |
|
does not respond to sounds, does not begin to speak by age 3

Figure
|
may respond to some sounds but not others
Check for ear infection (pus). |
Check for:
· deafness
· severe developmental delay (with or without
deafness)
· severe cerebral palsy |
|
does not turn head to look at things, or reach for things until
they touch her

Figure
|
Eyes may or may not look normal. |
· blindness and/or
· severe mental retardation
· severe cerebral palsy |
|
Eyelids or eyes make quick, jerky, or strange movements.

Figure
|
Check for one or a combination of these. |
· blindness
· fits
· too much
medicine
· cerebral palsy
· other problems affecting or damaging the brain |
|
All or part of body makes strange, uncontrolled movements.

Figure
|
· begins suddenly, child may
fall or lose consciousness
· child is normal
(or more normal) between ‘fits’ |
epileptic fits (Pattern varies a lot in different children - or
even in the same child.) |
|
slow, sudden, or rhythmic movements; fairly continuous (except
in sleep); no loss of consciousness

Figure
|
athetoid cerebral palsy
(Note: Fits and cerebral palsy may occur in the
same child.) |
|
Body, or parts of it, stiffens when in certain positions: poor
control of some or all movements. |
· different positions in
different children
· Body may stiffen
backward and legs cross.

Figure
|
spastic cerebral palsy |
PARTS OF BODY WEAK OR PARALYZED
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
floppy or limp weakness in part or all of body
no loss of feeling in affected parts
no spasticity (muscles that tighten without control)
normal at birth |
· usually began with a ‘bad
cold’ and fever before age 2
Figure
· irregular pattern of parts
weakened. Often one or both legs - sometimes arm, shoulder, hand, etc. |
polio |
|
· begins little by little and
steadily gets worse
· about the same on both
sides of body
· often others in the family
also have it

Figure
|
· muscular dystrophy
· muscular atrophy |
|
Figure
· Paralysis starts in legs and
moves up: may affect whole body.
· or,
pattern of paralysis variable |
tick paralysis

Figure
Guillain-Barr� paralysis (usually temporary)
paralysis from pesticides, chemicals, foods (lathyrism) |
|
lump on back |
tuberculosis of spine |
|
floppy or limp weakness
usually some loss of feeling |
· one or both hands or feet

Figure
· develops slowly in older
child. Gets worse and worse. |
leprosy |
|
· born with bag on back (Look
for scar.)

Figure
· feet weak, often without
feeling |
spina bifida

Figure
|
|
· usually from back or neck
injury
· weakness, loss of feeling below
level of injury
· may or may not have muscle
spasms
· loss of bladder and bowel control
|
spinal cord injury

paraplegia (lower body)

quadriplegia (upper and lower
body)
|
|
injury to nerves going to one part of body |
hand weakness sometimes caused by using crutches wrongly |
|
weakness usually with stiffness or spasticity of muscles
no loss of feeling |
usually affects body in one of these patterns

Figure
|
· 1: cerebral palsy (or stroke,
usually older persons)
· 2 and 3: cerebral
palsy
· occasional other causes |
|
Muscles tighten and resist movement because of joint pain. |
JOINT PAIN
(many causes - see below) |
JOINT PAIN
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
one or more painful joints |
· begins with or without
fever
· gradually gets worse, but there are
better and worse periods

Figure
|
juvenile arthritis |
|
|
other causes of joint pain See chart on joint pain. |
WALKS WITH DIFFICULTY OR LIMPS
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
dips to one side with each step

Figure
|
one leg often weaker and shorter |
Check for:
· polio
· cerebral palsy
·
dislocated hip |
|
· usually begins age 4 to
8
· may complain of knee pain |
damaged hip joint |
|
walks with knees pressed together

Figure
|
· muscle spasm and
tightness
· upper body little affected |
spastic diplegic or paraplegic cerebral palsy |
|
stands and walks with knees together and feet apart

Figure
no other problems |
feet less than 3”
apart at age 3
Figure
|
normal from ages 2 to 12 |
|
feet more than 3”
apart at age 3

Figure
|
knock-kneed |
|
walks awkwardly with one foot tiptoe

Figure
|
muscle spasms and poor control on that side. Hand on that side
often affected. |
hemiplegic cerebral palsy
(stroke in older persons) |
|
walks awkwardly with knees bent and legs usually separated

Figure
|
· jerky steps, poor
balance
· sudden, uncontrolled movements that
may cause falling |
athetoid cerebral palsy |
|
· slow ‘drunken’ way
of walking
· learns to walk late and falls
often |
· poor balance (ataxia) - often
with cerebral palsy
· Down syndrome
(mongolism)
· cretinism |
|
walks with both feet tiptoe

Figure
|
· weakness, especially in legs
and feet
· gradually gets worse and worse
|
muscular dystrophy |
|
legs and feet stiffen (spasticity of muscle) |
spastic cerebral palsy |
|
no other problems |
normal? (some normal children at first walk on tiptoes) |
|
walks with hand(s) pushing thigh(s) or with knee(s) bent back

Figure
|

Figure
difficulty lifting leg |
· polio
· muscular dystrophy
· arthritis (joint pain)
· other causes of muscle weakness |
|
Foot hangs down weakly (foot drop).

Figure
|
Child lifts foot high with each step so that it will not drag.

Figure
|
· polio
· spina bifida
·
muscular dystrophy
· muscular
atrophy
· nerve or muscle injury
· other cause of weakness |
|
dips from side to side with each step
Figure
|
due to muscle weakness at side of hips, or double dislocated
hips, or both |
· polio
· cerebral palsy
·
spina bifida
· Down syndrome
· muscular dystrophy
· child who stays small
· arthrogryposis
·
dislocated hips (may occur with any of the above) |
|
walks with one (or both) hip, knee, or ankle that stays bent
Figure
|
joints cannot be slowly straightened when child
relaxes |
· contractures (shortened
muscles)
· joined or fused joints
may be secondary to:
· polio
· joint infection
·
other causes |
|
Joints can gradually be straightened when child
relaxes. |
spasticity, often cerebral palsy |
|
Knees wide apart when feet together (bow legs). Waddles or dips
from side to side (if he walks).

Figure
|
under 18 months old |
often normal |
|
Any combination of these:
· Joints look big or
thick.
· Child is short for age.
· Bones weak, bent, or break easily.
· Arms and legs may seem too short for body, or
‘out of proportion’.
· Belly and
butt stick out a lot.

Figure
|
Consider:
· rickets (lack of vitamin D and
sunlight)
· brittle bone disease
· children who stay very short (dwarfism)
· cretinism
· Down
syndrome
· dislocated hips |
|
flat feet
Figure
|
no pain or other problems |
normal in many children |
|
· Pain may occur in arch of
foot.
· Deformity may get worse. |
may be problems in:
· cerebral palsy
· polio
· spina
bifida
· Down syndrome |
BACK CURVES AND DEFORMITIES
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
sideways curve of backbone

Figure
|
When child bends over, look for a lump on one side.
Figure
|
‘scoliosis’ - may occur alone or as complication of:
· polio
· cerebral palsy
·
muscular dystrophy
· spina bifida
· other physical disability |
|
sway back
Figure
|
· belly often sticks
out
· may be due to (1) contractures here, or
weak stomach muscles |
‘lordosis’ - may occur in:
· polio
· spina bifida
·
cerebral palsy
· muscular dystrophy
· Down syndrome
·
cretinism
· child who stays small
· many other disabilities |
|
rounded back

Figure
|
|
‘kyphosis’ - often occurs with:
· arthritis
· spinal cord injury
· severe polio
·
brittle bone disease |
|
(1) hard, sharp bend of or bump in backbone

Figure
|
· starts slowly and without
pain
· often family history of
tuberculosis
· may lead to paralysis of lower
body |
tuberculosis of the spine |
|
dark soft lump over backbone

Figure
|
· present at birth
· sometimes only a soft or slightly swollen area over
spine
· weakness and loss of feeling in feet
or lower body |
spina bifida (‘sack on the back’) |
OTHER DEFORMITIES
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
missing body parts |
born that way

Figure
|
born with missing or incomplete parts |
|
accidental or surgical loss of limbs (amputation)

Figure
|
amputations |
|
gradual loss of fingers, toes, hands, or feet, often in persons
who lack feeling

Figure
|
· osteomyelitis (bone
infections) sometimes seen with;
· leprosy
(hands or feet)
· spina bifida (feet only)
|
|
hand problems |
· floppy paralysis (no
spasticity)

Figure
· without care may lead to
contractures so that fingers cannot be opened |
may occur with:
· polio
· muscular dystrophy
· muscular atrophy
·
spinal cord injury (at neck level)
·
leprosy
· damage to nerves or cords of arms
All may lead to contractures. |
|
· uncontrolled muscle tightness
(spasticity)
· strange movements
· or hand in tight fist

Figure
|
spastic cerebral palsy
may lead to contractures |
|
burn scars and deformities

Figure
|
burns |
|
clubbing or bending of feet |
may begin as floppy weakness and become stiff from contractures,
if not prevented

Figure
|
may occur with many physical disabilities, including:
· polio
· cerebral palsy
·
spina bifida
· muscular dystrophy
· arthritis
· spinal
cord injury |
DISABILITIES THAT OFTEN OCCUR WITH OR ARE SECONDARY TO
OTHER DISABILITIES
|
IF THE CHILD HAS THIS |
AND ALSO THIS |
HE MAY HAVE |
|
Developmental delay: child slow to learn to use her body
or develop basic skills

Figure
|
caused by slow or incomplete brain function or by severe
physical disability, or both |
often seen in:
· mental retardation
· cerebral palsy
·
severely or multiply disabled children |
|
caused by overprotection: treating children like babies when
they could do more for themselves |
some delay can occur with almost any disability |
|
Contractures
joints that no longer straighten because muscles have shortened

Figure
|
· usually due to muscle weakness
or spasticity
· Often, muscles that pull a
joint one way are much weaker than those that pull it the other way (muscle
imbalance). |
often secondary to:
· polio
· cerebral palsy
·
spina bifida
· arthritis
· muscular dystrophy
· Erb’s palsy
·
amputations
· leprosy |
|
sometimes due to scarring from burns or injuries |
burns |
|
Behavior problems

Figure
|
may come from:
· brain damage
· difficulty understanding things
· overprotection
·
difficult home situation
(Some children with epilepsy from brain damage may pull out
hair, bite themselves, etc.) |
behavior problems common with:
· mental retardation
· fits (epilepsy)
·
cerebral palsy
and for emotional reasons, with:
· spinal cord injury
· muscular dystrophy
· deafness
·
learning disability |
|
Slow to learn certain things only; otherwise intelligent.
|
· often over-active or
nervous
· sometimes behavior problems |
learning disability |
|
Speech and communication problems |
· often, but not always, due to
deafness or retardation (or both)
· Some
children can hear well and are but still cannot speak.

Figure
|
may occur with:
· deafness
· developmental delay
· cerebral palsy
·
Down syndrome
· cretinism
· children who stay small
· brittle bone disease
· cleft lip and palate
(Deafness may occur together with these and other disabilities.)
|
|
other problems that sometimes occur secondary to
other disabilities
(Some of these we have already included in this chart.) |
Main disability
· cerebral palsy |
Common secondary disabilities
· blindness
· deafness
· fits
|
|
· many disabilities with
paralysis |
· spinal curve |
|
· persons who have lost feeling:
leprosy, spinal cord injury, spina bifida |
· pressure sores
· osteomyelitis (bone infection)
· loss of urine and bowel control |
Chapter 7: Polio: Infantile Paralysis
HOW TO RECOGNIZE PARALYSIS CAUSED BY POLIO
MUSCLES COMMONLY WEAKENED BY
POLIO
· Paralysis
(muscle weakness) usually begins when the child is small, often during an
illness like a bad cold with fever and sometimes diarrhea.
· Paralysis may affect any
muscles of the body, but is most common in the legs. Muscles most
often affected are shown in the drawing.
· Paralysis is of the
‘floppy’ type (not stiff). Some muscles may be only partly
weakened, others limp or floppy.
· In time the affected limb may
not be able to straighten all the way, due to shortening, or
‘contractures’, of certain muscles.
· The muscles and bones of the
affected limb become thinner than the other limb. The affected limb does not
grow as fast, and so is shorter.
· Unaffected arms or legs often
become extra strong to make up for parts that are weak.
· Intelligence and the
mind are not affected.
· Feeling is not
affected.
· ‘Knee jerks’ and
other tendon reflexes in the affected limb are reduced or absent.
(In cerebral palsy, ‘knee jerks’ often jump more than normal.) Also,
the paralysis of polio is ‘floppy’; limbs affected by cerebral palsy
often are tense and resist when straightened or bent.
Figure
· The paralysis does not get
worse with time. However, secondary problems like contractures, curve of the
backbone and dislocations may occur.
|
Of children who become paralyzed by polio:
30% recover completely in the first weeks or months.

Figure
30% have mild paralysis.

Figure
30% have moderate or severe paralysis.

Figure
10% die (often because of difficulty breathing or swallowing).

Figure
|
BASIC QUESTIONS AND ANSWERS ABOUT POLIO
How common is it? In many countries, polio - or
‘poliomyelitis’ - is still the most common cause of physical
disability in children. In some areas, at least one of every 100 children may
have some paralysis from polio. Where vaccination programs are
effective, polio has been greatly reduced.
What causes it? A virus (infection). The
infection attacks parts of the spinal cord, where it
damages only the nerves that control movement. In areas with poor
hygiene and lack of latrines, the polio infection spreads when the stool (shit)
of a sick child reaches the mouth of a healthy child. Where sanitation is
better, polio spreads mostly through coughing and sneezing.

Paralysis in one leg
Do all children who become infected with the polio virus
become paralyzed? No, only a small percentage become paralyzed. Most only
get what looks like a bad cold, with fever. However, if a child with a
‘cold’ caused by the polio virus is given an injection of any
medication, the irritation caused by the injection can bring on
paralysis.
Is the paralysis contagious? No, not after 2 weeks from
when a child first gets sick with polio. In fact, most polio is spread through
the stool of non-paralyzed children who have ‘only a
cold’ caused by the polio virus.

Severe paralysis
At what age do children get polio? In areas with poor
sanitation, polio most often attacks babies from 8 to 24 months old, but
occasionally children up to age 4 or 5. As sanitation improves, polio tends to
strike older children and even young adults.
Who does it most often affect? Boys, a little more than
girls. Unvaccinated children much more often than vaccinated children. Young
children who are given injections unnecessarily are paralyzed by polio more
often those who are not.
How does the paralysis begin? It begins after signs of a
cold and fever, sometimes with diarrhea or vomiting. After a few days the neck
becomes stiff and painful and parts of the body become limp. Parents may notice
the weakness right away, or only after the child recovers from the acute
illness.
Once a child is paralyzed, what changes or improvements can
be expected? Often the paralysis will gradually go away, partly or
completely. Any paralysis left after 7 months is usually permanent. The
paralysis will not get worse. However, certain secondary problems may develop -
especially if precautions are not taken to prevent them.
What are the child’s chances of leading a happy,
productive life? Usually very good-provided the child is encouraged to do
things for himself, to get the most out of school, and to learn useful skills
within his physical limitations.
Can persons with polio marry and have normal children?
Yes. Polio is not inherited (familial) and does not affect ability to have
children.
SECONDARY PROBLEMS TO LOOK FOR WITH POLIO
By secondary problems, we mean further disabilities or
complications that can appear after, and because of, the original disability.
CONTRACTURES OF JOINTS
A contracture is a shortening of muscles and tendons (cords) so
that the full range of limb movement is prevented.
Unless preventive steps are taken, joint contractures will form
in many paralyzed children. Once formed, often they must be corrected before
braces can be fitted and walking is possible. Correction of advanced
contractures, whether through exercises, casts, or surgery (or a combination),
is costly, takes time and causes discomfort. Therefore early prevention of
contractures is very important.
A full discussion of contractures, their causes, prevention, and
treatment is in the next chapter (Chapter 8). Methods and aids for correcting
contractures are described in Chapter 59.
|
TYPICAL CONTRACTURES IN POLIO
A child with paralysis who crawls around like this and never
straightens her legs will gradually develop contractures so that her hips,
knees, and ankles can no longer be straightened.

Figure
|
|
TYPICAL DEFORMITIES OF ANKLE AND FOOT |
|

|

|

|

|
|
bending down at ankle (tiptoe contracture) |
bending down at mid-foot |
bending out at ankle |
bending in at ankle |
OTHER COMMON DEFORMITIES
Weight bearing (supporting the body’s weight) on weak
joints can cause deformities, including:
|
OVER-STRETCHED JOINTS |
DISLOCATIONS |
|

Figure
|

Figure
|
partly or completely dislocated
joints (especially knee, foot, hip, shoulder, elbow, thumb)
|

partly dislocated foot
|
|
WARNING:
Dislocations like these are sometimes caused by
stretching contractures incorrectly. |
SPINAL CURVE
Minor curve of spine can be caused by tilted hips, as a result
of a short leg.

Figure
More serious curve of the spine is caused by
muscle weakness of the back or body muscles. The curve can become so severe that
it endangers life by leaving too little room for the lungs and heart.

a severely paralyzed child
At first, the spinal curve straightens when the child is
positioned better. But in time the curve becomes more fixed (will not straighten
any more). For information on spinal curves, see Chapter 20.
WHAT OTHER DISABILITIES CAN BE CONFUSED WITH POLIO?
· Sometimes cerebral
palsy can be mistaken for polio - especially cerebral palsy of the
‘floppy’ type.
However, cerebral palsy usually affects the body in
typical patterns:
CEREBRAL PALSY
Polio has a more irregular pattern of paralysis:

POLIO
In cerebral palsy, usually you can find other signs of brain
damage: over-active knee jerks and abnormal reflexes, developmental delay,
awkward or uncontrolled movement, or at least some muscle tenseness
(spasticity).
· In muscular dystrophy,
paralysis begins little by little and steadily gets worse.

Figure
· Hip problems can cause
limping, and muscles may become thin and weak. Check hips for pain or
dislocations. (Note: Dislocated hip may also occur
secondary to polio.)

Figure
· Clubbed foot is present
from birth.
Figure
|
Note: Polio can occur before or after a child has
any of these other problems. Check carefully. |
· ‘Erb’s
palsy’, or partial paralysis in one arm and hand, comes from birth
injury to the shoulder.
Figure
· Leprosy. Foot and hand
paralysis begins gradually in older child. Often there are skin patches and loss
of feeling.

Figure
· Spina bifida is present
from birth. There is reduced feeling in the feet, and often a lump (or scar from
surgery) on the back.
Figure
|
ALWAYS EXAMINE THE BACK IN A CHILD WITH PARALYSIS OF THE LEGS,
AND CHECK FOR FEELING. |
· Injuries to the spinal
cord or to particular nerves going to the arms or legs. There is usually a
history of a severe back or neck injury, and loss of feeling in the paralyzed
part.
Figure
· Tuberculosis of the
spine can cause gradual or suddenly increasing paralysis of the lower body.
Look for typical bump on spine.

Figure
· Other causes of paralysis
or muscle weakness. There are many causes of floppy paralysis similar to
polio. One of the most common is ‘Guillain-Barr�’ paralysis.
This can result from a virus infection, from poisoning, or from unknown causes.
It usually begins without warning in the legs, and may spread within a few days
to paralyze the whole body. Sometimes feeling is also reduced. Usually strength
slowly returns, partly or completely, in several weeks or months.
Rehabilitation and prevention of secondary problems are basically the
same as for polio.
WHAT CAN BE DONE?
DURING THE ORIGINAL ILLNESS, when the child first becomes
paralyzed:
· No medicines help,
either during the first illness, or later.
· Rest is important.
Avoid forceful exercise because this may increase paralysis. Avoid
injections.
· Good food during
recovery helps the child become stronger. (But take care that the child does not
eat too much and get fat. An overweight child will have more problems with
walking and other movements.) For suggestions about good food, see Where
There Is No Doctor, Chapter 11.
· Position the child to
be comfortable and to avoid contractures. At first the muscles will be painful,
and the child will not want to straighten his joints. Slowly and gently try to
straighten his arms and legs so that the child lies in as good a position as
possible. (See Chapter 8.)

GOOD POSITION
Arms, hips, and legs as straight as possible. Feet supported.

BAD POSITION
Bent arms, hips, and legs. Feet in tiptoe position.
Note: To reduce pain, you may need to put
cushions under the knees, but try to keep the knees as straight as you can.
FOLLOWING THE ORIGINAL ILLNESS:
· Continue with good food
and good positions.
· As soon as the fever drops,
start exercises to prevent contractures and return strength.
Range-of-motion exercises are described in Chapter 42. Whenever possible,
make exercises fun. Active games, swimming, and other activities to
keep limbs moving as much as they can are important throughout the
child’s rehabilitation.
· Crutches, leg braces
(calipers), and other aids may help the child to move
better and may prevent contractures or deformities.
· In special cases,
surgery may be needed to correct contractures, or to change the place where
strong muscles attach, so that they help do the work of weak ones. When a foot
is very floppy or bends to one side, surgery to join certain bones of the foot
may help. But because bone surgery stops the growth of the foot, usually it
should not be done before age 12 or 13.

Figure
· Encourage the child to use
his body and mind as much as possible, to play actively with other children,
to take care of his daily needs, to help with work, and to go
to school. As much as possible, treat him like any other child.
REHABILITATION OF THE CHILD WITH PARALYSIS
All children paralyzed by polio can be helped by certain basic
rehabilitation measures - such as exercise to keep a full range of motion in the
affected limbs.
However, each child will have a different combination and
severity of paralyzed muscles, and therefore will have his own special
needs.
For some children, normal exercise and play may be all that are
needed. Others may require special exercises and playthings. Still others may
need braces or other aids to help them move about better, do things more easily,
or keep their bodies in healthier, more useful positions. Those who are severely
paralyzed may be helped most by a wheelboard (trolley) or wheelchair.

For this child, walking provides
exercise that stretches his legs and feet, and prevents contractures. (Tilonia,
India)
Every child needs to be carefully examined and evaluated in
order to best meet his or her particular needs. The earlier you evaluate a
child’s needs, and take steps to meet them, the better.
Unfortunately, in most areas where polio is still common,
village rehabilitation programs do not exist or are just beginning. Many
children (and adults) who have been paralyzed for a long time already have
severe deformities or joint contractures. Often these must be corrected before a
child can use braces or begin to walk.

This child, who had polio as a
baby, already had severe contractures in the hips, knees, and feet.
(PROJIMO)

It took several months of
exercises at home and then a series of plaster casts in the village
rehabilitation center to straighten the contractures so he could walk with
braces.
Because contractures are such a common problem, not only with
polio but with many other disabilities, we discuss them separately in the next
chapter. Before evaluating a child with polio, we strongly suggest you read
Chapter 8 on contractures.
|
WARNING: Before deciding on any aid or
procedure, carefully consider its advantages and disadvantages. For example,
some deformities may be best left uncorrected because they actually help the
paralyzed child stand straighter or walk better. And some aids or braces may
prevent a child from developing strength to walk without aids. Before
deciding what aid or procedure to use, we suggest you read Chapter 56,
“Making Sure Aids and Procedures Do More Good Than Harm.” |
PROGRESS OF A CHILD WITH POLIO: THE CHANGING NEEDS FOR
AIDS AND ASSISTANCE
1. exercises to keep full range of motion, starting
within days after paralysis appears and continuing throughout rehabilitation

Figure
2. supported sitting in positions that help prevent
contractures

Figure
3. active exercises with limbs supported, to gain
strength and maintain full motion

Figure
4. exercise in water-walking, floating, and swimming, with
the weight of the limbs supported by the water
Figure
5. wheelboard or wheelchair with supports to prevent or
correct early contractures.
Figure
Note: These also provide good arm exercise in
preparation for walking with crutches.
6. braces to prevent contractures and prepare for walking

Figure
7. parallel bars for beginning to balance and walk
Figure
8. walking machine or ‘walker’

Figure
9. crutches modified as walker for balance and extra
support
Figure
10. under arm crutches

Figure
11. forearm crutches

Figure
and perhaps in time...
12. a cane or no arm supports at all

Figure
Note: These pictures are only an example - but
most of the steps are necessary for many children. Children who begin
rehabilitation late may also have contractures or deformities requiring
corrective steps not shown here.
EVALUATING A CHILD’S NEEDS FOR AIDS AND PROCEDURES
Step 1: Start by learning what you can through talking
with the child and family (see Child’s History). As you do this, watch
the child move about. Observe carefully which parts of the body seem strong,
and which seem weak. Look for any differences between one side of the body and
the other - such as differences in the length or thickness of the legs. Are
there any obvious deformities, or joints that do not seem to straighten all the
way? If the child walks, what is unusual about the way she does it? Does she dip
forward or to one side? Does she help support one leg with her hand? Is one hip
lower than the other? Or one shoulder? Does she have a humpback, a swayback, or
a sideways curve of the back?
These early observations will help you know what parts of the
body you most need to check for strength and range of motion. Often, by watching
a child you can begin to get an idea about what kind of aids or assistance may
help. For example:
|
Carmen appears to have severe paralysis affecting both legs and
her right arm. Weakness in her trunk (main part of the body)
appears to have caused a severe S-shaped curve of the spine.

Figure
She will probably never walk, and will need a wheelchair or
wheel board.

Figure
You may want also to make her a body brace (1), or help her in
other ways to sit more upright and try to keep the spine from bending more.
|
|
Pedro appears to have severe paralysis in his legs and hips. It
looks as if his hips, knees, and feet cannot straighten (contractures). Weak
stomach muscles and severe hip contractures may be the cause of his swayback.

Figure

Figure
(1) Because his arms look strong, Pedro will probably be able to
walk with crutches and leg braces. But first his contractures must be
straightened.
(2) strap to gradually straighten hips
(3) casts to straighten knees and ankles
If the contractures cannot be straightened by gradual
stretching, he may need surgery.

Figure
Because of hip weakness, he may need long leg braces with a hip
band. |
|
Manuel walks with the help of a stick. He appears to have
paralysis mainly in his right leg and foot. Because of weak thigh muscles, he
‘locks’ his knee backward in order to bear weight on it. This
‘back-kneeing’ has become more and more extreme as the cords behind
the knee stretch. The foot is very unstable and flops to one side. The weaker
leg looks somewhat shorter - and for walking is much shorter because of the
bent-back knee and bent-over foot.

Figure
He might be able to walk without the stick if he uses a
below-knee brace to stabilize his foot.
Figure
But the back-knee would become worse and worse until he could
not walk. So probably he should have a long-leg brace. The brace might allow his
knee to bend backward just a little for stability - so that no knee lock is
needed. |
|
Afia leans forward and pushes her weak left thigh with her hand
when she walks. Her left knee cannot quite straighten. Her weak leg looks a
little shorter than the other.

Figure
Exercises to get her knee straighter or so it can bend very
slightly backward may be all that is needed for Afia to walk without using her
hand.

Figure
Or she may need an above-knee brace with a strap to pull the
knee back.
Figure
Or she may only need a below-knee brace that helps push her knee
back.
Figure
The brace bends the foot down just a little, so that by bearing
weight on toes (rather than heel) her knee is pushed back.
To get a better idea about which of the three solutions may work
best for Afia, you will need to do a careful physical examination, testing range
of motion and muscle strength of the hip, knee, and ankle joints. |
Step 2: This is the physical examination. It
should usually include:
1. Range-of-motion testing, especially where
you think there might be contractures. (See “Physical Examination”,
and “Contractures”)
2. Muscle testing, especially of muscles that you think
may be weak. Also test muscles that need to be strong to make up for weak ones
(such as arm and shoulder strength for crutch use).
3. Check for deformities: contractures; dislocations
(hip, knee, foot, shoulder, elbow); difference in leg length; tilt of hips; and
curve or abnormal shape of the back.
Step 3: After the physical exam, again observe how the
child moves or walks. Try to relate her particular way of moving and
walking with your physical findings (such as weakness of certain muscles,
contractures, and leg length).
Step 4: Based on your observations and tests, try to
figure out what kind of exercises, aids, or assistance might help the child
most. Consider the advantages of different possibilities: benefit, cost,
comfort, appearance, availability of materials, and whether the child is likely
to use the aid you make. Ask the child and parents for their opinions and
suggestions.
Step 5: Before making a final brace or aid to fit the
child, if possible test to see how well it may work by using a temporary
aid or old brace from another child. For example,

If a child’s ankle bends
over to the outside like this...

...a lift on the outer side of
the sole like this, may help to keep the foot straighter.
But before nailing and glueing in the lift,
quickly make a trial one of cardboard or something else and fasten it
temporarily to the sandal or shoe with tape or string. Then have the child walk.

Figure
Note: For a few children, a lift like this
will help. For many it will not.
|
Ask the child what she thinks. |
Step 6: After the child, her parents, and you have
decided what kind of brace or aid might work best, take the necessary
measurements and make the brace or aid. When making it, once again it is
wise to put it together temporarily so that you can make adjustments before you
rivet, glue, or nail it into its final form.
Step 7: Have the child try the brace or aid for a few
days to get used to it and to see how well it works. Ask the child and
parents if it seems to help. Does it hurt? Are there any problems? How could it
be improved? Is there something that might work better? Make what adjustments
are necessary. But remember that no brace or aid is likely to meet the needs of
a child perfectly. Do the best you can.

Mari and Chelo making a
child’s brace
Here is a story of how workers in a small village rehabilitation
program figured out what kind of aids a child needed. How many of the steps
we have just discussed did they follow? Was each step important?
|
A STORY: A BRACE FOR SAUL

Figure
One day a mother from a neighboring village arrived at the
village center with her 6 year old son, Saul. Mari and Chelo, 2 of the village
rehabilitation workers, welcomed them warmly. Learning that Saul had polio as a
baby, they asked him to walk, and then to run, while they watched carefully.
Saul limped a lot and one leg looked thinner and shorter. With each step it bent
back at the knee.
“He walks quite well, really,” said Mari. “But he
has to ‘lock’ his knee back in order to put weight on it. That knee is
going to keep stretching back and some day it will give out.”
“A long-leg brace would protect his knee,” suggested
Chelo.
“Oh, please, no!” said Saul’s mother. “A
year ago we took Saul to the city and the doctors had a big metal brace made for
him. It cost so much we are still in debt! Saul hated it! He would always take
it off and hide it. We tried and tried to get him to use it, but he
wouldn’t.”

Figure
“That’s not surprising,” said Mari. “Often a
child who can walk without a brace will refuse to use one - even if he walks
better with it. We could make him a long-leg brace out of plastic. It would be
much lighter. What do you say, Saul?” Saul began to cry.
“Don’t worry, Saul. Maybe we can do something
simpler,” said Mari. “But first let’s examine you, okay?”
Saul nodded.
On muscle testing Saul, they found he could not straighten his
knee at all. But he had fair strength for bending his knee back and his hip
forward, and good strength for bending his hip back,
Figure
and his hip forward,

Figure
and good strength for bending his hip back,
Figure
“With the hip and thigh strength he has, he should almost
be able to stand on that leg without the knee bending back,” said Mari.
“Saul, let’s see you try it like this. Pretend you’re a
stork!” For a moment Saul could do it. “Good!” said Mari.
“Every day stand like that and see how high you can count without letting
your knee go back. Every day try to beat your old record! Okay?”
“Okay,” said Saul. “Sounds like fun!”

Figure
“The stork exercises may help,” said Chelo. “But
I still think he needs a brace. At I east at first.”
“We must weigh the advantages against the
disadvantages,” said Mari. “A long-leg brace would keep his knee
straight. But it could weaken the muscles he needs to strengthen. Since the
brace would keep his leg from bending back, he wouldn’t have to use his
muscles to do it”.
A long-leg brace might weaken the
muscles Saul needs to strengthen.
“On the other hand, we might try a short-leg brace that
holds his foot at almost a right angle. Then, to step flat he will have to keep
his knee nearly straight. It could help him strengthen his behind-the-thigh
muscles.”
“Let’s try it!” Everyone agreed, except Saul.

short-leg plastic brace
Chelo brought someone’s old, lower-leg plastic brace and
showed it to Saul. “See how it will fit right around your leg. It
isn’t heavy at all. Lift it! And no metal joints to get in the way! What do
you say? Do you want to try it?”
“I guess so,” said Saul.
When the brace was made, they tested it. Saul said he liked it.
At first, when he tried hard, he could walk without bending his knee back. But
after a few days, his mother complained that often he would walk, or even stand,
with his knee bent way back as before, and his toes in the air, like this.

“WE THOUGHT IT WOULD WORK
LIKE THIS...”
“BUT IN FACT IT WORKED LIKE
THIS.”
“I have an idea,” said Chelo. “Why don’t we
let the heel stick out behind the shoe. That way, when he steps, his weight will
come well forward of the back of his heel. This should help bring his foot down
and his knee forward.”
They tried it, and most of the time (especially when he was
reminded) Saul walked without letting his knee bend back much.

Figure
At home Saul’s mother encouraged him to do his stork
exercises. As his muscles grew stronger, he began to walk without bending his
knee far back - even in active play!
Figure

Figure
|
“WILL MY CHILD EVER BE ABLE TO WALK?”
This is often one of the first questions asked by the parents of
a disabled child. It is an important question. However, we must help parents
realize that other things in life can be more important than walking.

Figure
If the child whose legs are severely paralyzed by polio is to
walk, generally she will need at least 2 things:
1. fairly strong shoulders and arms for
crutch use
2. fairly straight legs (hips, knees, and feet). (It is
important to correct contractures so that the legs are straight or nearly
straight before trying to adapt braces for walking.)
To evaluate a child’s possibility for walking, always
test arm and shoulder strength:
Have her try to lift her body weight off the ground with her
arms, like this.
If she can easily lift up and down several times, she has a GOOD
chance of being able to walk using crutches.
If her arms and shoulders are so weak she cannot begin to lift
herself, her chances for crutch-walking are POOR.

Figure
If her shoulder and arm strength is FAIR, and the child can
almost lift herself, dally exercise lifting her weight like this may increase
strength enough to make crutch use possible

Figure
Having the child lift herself while holding a bar like this (1)
will also help strengthen her hands and wrists for crutch use.
Figure
Pushing herself in a wheelchair or wheelboard (trolley) (2) is a
practical way to strengthen shoulders, arms, and hands.
If the child cannot lift herself because of weak elbows, put
simple splints on her arms to see if she can lift herself with these.
Figure
If she can lift herself with the elbow splints, maybe she can
use crutches that give elbow support.

Figure
If she is fat, she should lose weight. This will make
walking on weak limbs much easier.
Figure
Now check how straight the legs will go. (See range-of-motion
testing)
If the hips, knees, and feet can be placed in fairly straight
positions, chances for walking soon with braces are good (if arm strength is
good).

Figure
But if the child has much contracture of the hips, knees, or
feet, these will need to be straightened before she will be able to walk.

Figure
Sometimes, if contractures are severe in one leg only the child
can learn to walk on the other leg only, with crutches. But it is best with both
legs, whenever possible.

Figure
For correction of contractures, see Chapters 8 and 59.
After checking arm strength and leg straightness, the next thing
to check is the strength in the ankles, knees, and hips. This will help
you decide if the child needs braces, and what kind.
A child with a foot that hangs down (foot drop), or
flops to one side may be helped by a below-knee brace of plastic or metal.
For foot drop, you can make a brace that lifts the foot with a
spring or rubber band.

Foot drop: he cannot lift his
foot.

Foot flops to one side.

PLASTIC

METAL

Figure
The kind of brace you choose will depend on various factors,
including cost, available skills and materials, and what seems to work best for
the particular child. Advantages and disadvantages of different kinds of
braces, and how to make them, are discussed in Chapter 58.
A child with a weak knee may need a long-leg brace of
plastic or metal.

Figure

Figure

Figure
Upper-leg braces may be made with or without a knee joint that
locks straight for walking and bends for sitting. Different models are discussed
in Chapter 58.
Note: Not all children with no strength to straighten
the knee need long-leg braces: A child with strong butt muscles may be able
to walk without a brace.

Figure

Figure
STRONG butt muscles (1) pull the thigh back and keep the knee
from bending.
Figure
A child who has FAIR butt strength and a straight knee may be
helped enough by a lower-leg brace (2) that pushes the knee back.
brace pushes knee back(3)
Slightly downward angle of a stiff brace causes it to push the
knee backward when weight bearing (4).

Figure
A child with weak butt muscles may walk with one hand pushing on
the weak thigh (5).

Figure
Or he may walk by bending the knee back to ‘lock’ it
for weight bearing (6).
|
CAUTION: A stiff foot with a moderate
tiptoe contracture may help push the knee back, just like a stiff brace.
Correcting the contracture may make walking more difficult or impossible, so
that a brace is needed where none was needed before. (See Chapter 56.)

Figure
|
If a child has a contracture and cannot walk with his knee
straight, correcting the contracture until his knee bends very slightly backward
may allow him to walk better.
A child with very weak hip muscles may find his leg flops
or twists about too much with a long-leg brace.

Figure

or if he cannot turn his leg in
and out like this,

it may flop and twist with a
brace like this.
He may need a brace with a hip band to help stabilize the leg at
the hip.

BETTER
A hip band that sits on the butt (1) often provides better
posture than a higher waistband.
joint for sitting (with a lock if necessary) (2)
A plastic hip band is less stable but more flexible and allows
better stepping in some children.

WORSE
A hip band that passes above the butt often lets the butt stick
way out and causes swayback (3).
A child with weak body and back muscles, who cannot hold
up her body well, may need long-leg braces attached to a body brace or body
jacket.
If she has difficulty holding her
body up like this,
she may need a brace with body
support.
Note: Often a child at first may need a hip
band or body jacket to help stabilize her for walking. A few weeks or months
later she may no longer need it. Removing it may help the child gain more
strength and control. It is important to re-evaluate the child’s needs
for bracing periodically.
|
Take care to use no more bracing than is needed. |
A child whose backbone is becoming seriously curved may
benefit from a body brace (or in severe cases, she may need surgery).

Figure
If necessary, the body brace can be attached to long-leg braces
as shown above.
More information on spinal curve can be found in Chapter 20. For
information on how to make body braces and jackets, see Chapter 58.
PREVENTION OF POLIO
· Vaccinate babies with
polio vaccine. Be sure they get the vaccine 3 times by the time they are 8
months old. It is usually best to give the first polio vaccination around 3
months of age.
|
POLIO VACCINE, the best protection - IF it has been kept
cold continuously!
Figure
|
· Vaccinate as many children
as possible. The vaccine given by mouth is alive. So, if most of the
children are vaccinated, the live vaccine will spread to children who have not
been vaccinated, and protect them also.
· Try to keep the live polio
vaccine frozen until shortly before it is used. For up to 3 months it can be
thawed and refrozen. But it must be kept cold or it will spoil.
· Seek community help
with vaccination and in keeping vaccine cold. Sometimes vaccines do not
reach villages because health posts lack refrigeration. But often storekeepers
and a few families have refrigerators. Win their interest and cooperation.

Figure
· To give best protection,
vaccinate the child when she does not have a fever or a cold or diarrhea.
But if by 6 months of age, the child still has not been vaccinated, give her the
polio vaccine even if she is a little sick. However, there is a chance that the
vaccine may not work if it is given when the child is sick (with a virus
infection). Therefore, still try to give the complete series of 3 vaccinations
and one booster later, when the child is not sick.
It is estimated that in poor countries at least one-third of
vaccines are spoiled by the time they reach the children. Therefore, even
in children who have been vaccinated, additional precautions are needed:
· Breast feed your baby
as long as possible. Breast milk contains ‘antibodies’ that may help
protect against polio. (Babies rarely get polio before 8 months old because they
still have their mothers’ antibodies. Breast feeding may make this
protection last longer.)

BREAST MILK PROTECTS AGAINST
INFECTIONS-INCLUDING POLIO
· Do not give injections of
any medicine to babies or children, except when absolutely necessary.
Irritation caused by injected medicine can turn a mild, undiagnosed polio
infection into paralysis. It is estimated that today 1 out of 3 cases of
paralysis from polio is brought on by injections.
|
DANGER!

Figure
INJECTIONS CAN CAUSE PARALYSIS FROM POLIO |
· Organize the people and
help out in popular campaigns to encourage vaccination, breast feeding,
and limited, sensible use of injections. Community theater and
puppet shows are good ways to raise awareness on these issues. See Chapter
48.
PREVENTION of secondary problems
We have already discussed some ways to prevent new problems or
complications in a child with paralysis. In summary, important measures include:
· Prevent contractures and
deformities. Begin appropriate range-of-motion exercises as soon as
the paralysis appears.
· At the first sign of a joint
contracture, do stretching exercises 2 or 3 times a day - every day.
|
Stretching exercises work better if you stretch the joint firmly
and continuously for a few moments, |
instead of ‘pumping’ the limb back and forth. |
|

CORRECT
|

WRONG
We emphasize this point because in many countries parents are
taught the pumping method - which does very little good. |
For more details, see “Contractures,” Chapter 8.
· Evaluate the child’s
needs regularly, and change or adapt aids, braces, and exercises to meet
her changing needs. Too little or too much bracing can hold the child back
or create new problems.
· Be sure crutches do not
press hard under the arms; this can cause paralysis of the hands.
Figure
· Try not to let the
child’s physical disability hold back her overall physical, mental, and
social development. Provide opportunities for her to lead an active life and
take part in games, activities, school, and work with other children. PART 2 of
this book discusses ways to help the community meet the needs of disabled
children.
|
OTHER PARTS OF THIS BOOK THAT MAY BE USEFUL IN MEETING NEEDS
OF A CHILD AFFECTED BY POLIO
*Especially important chapters are marked with a
star:*
Physical examination, Chapter 4
Measurement of contractures and progress, Chapter 5
* Contractures, Chapter 8
Dislocated hips, Chapter 18
Spinal curve, Chapter 20
* Range-of-motion and other exercises, Chapter 42
Crutch use, wheelchair transfers, etc., Chapter 43
Community needs, social adjustment, growing up, PART 2,
especially Chapters 47, 48, 52, 53
Making sure aids and procedures meet the child’s needs,
Chapter 56
* Braces and calipers, Chapter 58
* Correcting contractures, Chapter 59 Correcting club feet,
Chapter 60
Special seating and wheelchairs. Chapters 64, 65, 66
* Aids for walking, Chapter 63
For more information on polio, see References. |
|
A BOY WITH POLIO BECOMES AN OUTSTANDING HEALTH AND
REHABILITATION WORKER
Marcelo Acevedo was disabled by polio. He and his family lived
in a village 2 days from the closest road. Village health workers from Project
Piaxtla helped Marcelo get surgery for his knee contractures. After surgery he
got braces and Went to school. Then they trained him as a village health worker,
and he returned to serve his village.

Marcelo at age 4, sitting with
his older brother who was temporarily disabled when a tree fell on his leg.

Marcelo training at Project
Piaxtla.
When PROJIMO was formed, Marcelo joined as a village
rehabilitation worker. He studied brace-making as an apprentice in 2 brace shops
in Mexico City.

Marcelo making a plastic leg
brace.

Marcelo and other villagers make
a plaster body mold of a young boy’s chest. The child had polio and has a
severe curve of the spine.

With his plastic body brace, made
by Marcelo, the child can sit much straighter.
Marcelo is now one of the leaders in PROJIMO, and has gained the
respect of the whole village. He has recently married a village woman. |
Chapter 8: Contractures: Limbs That No Longer Straighten
WHAT ARE CONTRACTURES?
When an arm or leg is in a bent position for a long time, some
of the muscles become shorter, so that the limb cannot fully straighten. Or
shortened muscles may hold a joint straight, so it cannot bend. We say the joint
has a ‘contracture’. Contractures can develop in any joint of the
body. For example:
1. Miguel spent the first years of his life crawling
because one leg was paralyzed.

Figure
Because he could not stand, he kept his hip and knee
bent and his foot in a tiptoe position, like this (1).
2. In time, he could not straighten his hip or knee, or bend his
foot up. He had developed a:

Figure

Figure
3. Because of the contractures, Miguel could not
stand or walk, even with a brace.

Figure
shortened muscles causing hip contracture (1)
Shortened calf muscles cause a tight heel cord that keeps the
foot in a ‘tiptoe’ position (2).
Shortened muscles-that-bend-the-knee cause tight cords behind
the knee. This keeps it bent (3).
Contractures develop whenever a limb or joint is not moved
regularly through its full range of motion. This is likely when:
· a very weak or sick child is
in bed for a long time.

Figure
· a paralyzed limb
is kept bent or hanging.

Figure
· a child with an
amputation keeps joints bent.

Figure
· a child has joint
pain that prevents her from straightening her joints.

Figure
contractures in:
- neck
- shoulders
- back
-
elbow
- wrists
- finger
- hips
- knees
- ankles
- feet
-
toes
Why is it important to know about contractures?
· Most contractures can be
prevented through exercise and other measures. Yet in many communities, at
least half of the physically disabled children already have contractures.

hand paralysis with
contractures
· Contractures make
rehabilitation more difficult. Often they must be corrected before a child
can walk or care for himself.
· Correction of contractures
is slow, costly, and often very uncomfortable or painful.
· It is best not to let
contractures develop, and if they do begin to develop, to correct them as soon
as possible. Early contractures often can be easily corrected at home, with
exercises and positioning. Advanced, old contractures are much more
difficult to correct, and may require gradual stretching with plaster casts, or
surgery.
For all these reasons...
|
Every family with a disabled child should understand how
contractures develop, how to prevent them, and how to recognize and correct them
when they first begin. |
Muscle imbalance - a major cause of contractures
When the muscles that bend or pull a limb
in one direction are much stronger than those that pull it in the opposite
direction, we say there is a ‘muscle imbalance’. When paralysis,
painful joints, or spasticity cause a muscle imbalance, contractures are much
more likely to develop.
|
WITHOUT MUSCLE IMBALANCE-CONTRACTURES LESS
LIKELY |
WITH MUSCLE IMBALANCE-CONTRACTURES MORE LIKELY
|
|
A leg that is completely paralyzed is not very likely to develop
contractures. The knee may even straighten more than normal. |
If the muscles that straighten the knee (1) and lift the foot
(2) are very weak, and the muscles that bend the knee and lower the foot are
strong, |
Muscle imbalance causing contractures can result from spasms, or
spasticity, that increase the pull of certain muscles
(cerebral palsy and spinal cord injury). |
|

Figure
|

Figure
contractures are very likely to develop. |
For example, the bent elbow and crossed legs of this child with
spastic cerebral palsy can lead to contractures so that his legs cannot be
spread apart or his elbow straightened.

Figure
|
To check for muscle imbalance, test and compare the strength of
the muscles that bend a joint, and of the muscles that straighten it. (See
muscle testing)
EXAMINING THE CHILD FOR CONTRACTURES
This is done through testing the ‘range of
motion’ of different joints. Most contractures will be obvious when you
test for them. But hip contractures can easily be missed.

Figure
(1) This child can lie with his right leg almost flat...
(2) ... by arching his back. You might think he has little or no
hip contracture.

Figure
(1) But if you test him with his other knee bent up to his
chest...
(2) ... his back flattens and you can see the amount of
contracture.
Be sure to test for contractures with the leg lined up straight.

Figure
Also be sure joints do not dislocate when you test for
contractures, because this can fool you, too. For example:

This child’s foot can rest
on the ground,

Figure

Figure
If you hold the foot so it does not dislocate, you will see that
the ankle has a severe contracture.
How to tell contractures from spasticity
Spasticity (muscle tightening that
the child does not control) is common when there is damage to the brain or
spinal cord. It is sometimes mistaken for contractures. It is important to know
the difference.
|
SPASTICITY of ankle joint

If at first it resists under
steady pressure,

and then it slowly yields, it is
probably spasticity.
|
|
CONTRACTURES of ankle joint

If it resists under steady
pressure,
and does not yield, it is
probably a contracture.
|
Spasticity often leads to contractures.
MEASURING CONTRACTURES
This can be done by folding a paper and measuring the angle, as
shown here,

Figure
and then tracing that angle onto a record sheet.

Figure
You can record your measurements with stick figures.

Figure
Or an easier, more fun way is to use a flexikin.

Figure
Or use a ‘compass’.

Figure
Or make a simple instrument of 2 thin pieces of wood joined by a
bolt or rivet, tight enough so that they move stiffly.
Figure
By keeping a record of their child’s progress, a family can
see the results and is more likely to keep working hard at exercises to correct
a child’s contractures.

Figure
Can a contracture be straightened in the village?
Contractures usually begin with shortening of muscles, causing
tight cords (tendons). Later, the nerves, skin, and ‘joint
capsule’ also can become tight. (A ‘joint capsule’ is the tough
covering around a joint.)
When a contracture is only in the muscles and cords, it can
usually be straightened by exercises and casts at a village rehab center,
although sometimes this may take months. But if the contracture also involves
the joint capsule, it is often much more difficult or impossible to correct,
even with many months of using casts. Surgery may be needed.
|
Note: If you find the information on this page
hard to understand, do not worry. Come back to it later, when you meet very
stubborn contractures. |
TO TEST THE KNEE JOINT:
Check the range of motion of the knee with the hip straight and
then bent.

Figure
Explanation: One of the main muscles that causes a knee
contracture is the ‘hamstring muscle’, which runs all the way from the
hip bone to the bone of the lower leg. This means that when the hip is bent, the
tight muscles will bend the knee more.

Figure
|
If the knee straightens more when the hip is straight |

hip straight
|
|
than when the hip is bent, |

hip bent
|
|
probably this is a muscle contracture (a short hamstring
muscle). |
|
|
This can often be corrected in the village. |
THE KNEE BENDS MORE: MUSCLE CONTRACTURE |
|
But if the knee straightens equally when the hip is straight or
bent, |

Figure
|
|
probably there is contracture of the joint capsule. |

Figure
|
|
This often requires surgery. |
THE KNEE BENDS THE SAME: JOINT CAPSULE CONTRACTURE |
TO TEST THE ANKLE JOINT:
Check the range of motion of the ankle with the knee straight
and then bent.

Figure
Explanation: One of the main muscles that pulls the foot
to a tiptoe position runs from the thigh bone all the way to the heel. This
causes the heel cord to pull more when the knee is straight than when the knee
is bent.

Figure
|
If the foot pushes down more when the knee is straight |

knee straight
|
|
than when the knee is bent, it is a muscle contracture.
|
knee bent
|
|
This can often be corrected in the village. |
THE FOOT BENDS UP MORE: MUSCLE CONTRACTURE |
|
But if the foot angle is the same when the knee is straight or
bent, |
Figure
|
|
there probably is a contracture of the joint capsule.
|

Figure
|
|
This often requires surgery. |
THE FOOT BENDS THE SAME: JOINT CAPSULE CONTRACTURE |
JOINTS THAT DO NOT MOVE AT ALL
If a joint moves only a little, the joint capsule may be very
tight, or there may be a deformity in the bones. With exercises, try to
gradually increase the movement.
If a joint does not move at all, the bones may be
‘fused’ (joined together). This often happens when there is a lot of
pain and damage in the joint. When a joint has fused, exercise will usually not
bring back motion. The only surgery that might help return joint motion is to
put in an ‘artificial joint’ of metal or plastic. This surgery is very
costly, and if the person is very active, the joint may not last more than a few
years.
PREVENTION AND EARLY MANAGEMENT OF CONTRACTURES
Contractures can often be prevented by
(1) positioning, and (2) range-of-motion exercises.
POSITIONING
If a child is likely to develop contractures or has begun to
develop them, try to position her to stretch the affected joints. Look for ways
to do this during day-to-day activities: lying, sitting, being carried, playing,
studying, bathing, and moving about.
During a severe illness (such as acute polio), or a recent
spinal cord injury, contractures can develop quickly. Therefore, early
preventive positioning is very important:
|
CORRECT |
CORRECT |
WRONG |
|
Figure
Lying and sleeping straight helps prevent contractures. |
Figure
Also use pillows for side-lying to keep a good position. |

Figure
Lying and sleeping with the legs in a twisted or bent position
causes contractures. |
|
(1) Lying part of the time face down helps stretch hips
backward.
(2) Letting feet hang over edge helps prevent ankle
contractures.
(3) A pillow here helps stretch knees.

Figure
|

Figure
A foot board helps to prevent ankle contractures. |

Figure
The foot support can be leaned forward a little So that the
child can stretch his feet by pushing against it. (Be sure to pad it.) |
|
Support feet at right angles.
If knee contractures might develop, keep the knees straight as
much as possible. |

Figure

Figure
A child who spends most of the time sitting should spend part of
the day lying or standing (on a frame if necessary). This will help prevent
contractures of the hips and knees. |
|
WRONG |
BETTER |
BEST |
|
Figure
|
Figure
Figure out ways to help the child stay in contracture-preventing
positions. |
child-sized furniture
|
|
For a child with spasticity whose legs press together or cross,
look for ways to sit, lie, or carry him with his legs separated. Here are a few
examples.

Figure
|
For more ideas about special seating and positioning, see
Chapter 65.
Exercises to prevent contractures
Just as cats, dogs, and many other animals stretch their bodies
after they wake up, children often enjoy stretching their limbs and testing
their strength. This is one of the purposes of play.

Figure
|
Daily stretching keeps the joints able to move smoothly and
freely through their full range of motion. |
Unfortunately, some children, because of illness, paralysis or
weakness, are not able to stretch all parts of their bodies easily during their
play and daily activities. If some part of their body is not regularly stretched
or moved through its full range, contractures may develop.
To maintain full, easy movement of their joints and limbs, these
children therefore need daily exercises that move the affected parts of their
bodies through their full range of motion.

Range-of-motion exercises for the
shoulder.
Range-of-motion exercises for each body joint are discussed
in Chapter 42.
As much as possible, the child herself should try to move the
affected part through its range of motion. Often the limb will be too weak and
help is needed. But be sure the child moves it as much as she can
herself.

Figure
|
Have the child move the part as far as she can without help.
Then help her to move it the rest of the way. |
Where there is muscle imbalance, strengthening the weaker
muscles can help prevent contractures.
As much as possible, try to make exercises fun.

A child whose feet tend to bend
inward like this,

may benefit from exercises that
bend them outward, like this.
Walking on boards in a V-shape may provide similar stretching
and be more fun.
Figure
But going with father on the V-shaped paths to the bean fields
may be even more fun - and it stretches his ankles more, because it is a long
way.
Figure
FOUR WAYS TO APPROACH STRETCHING EXERCISES: To prevent
(or help correct) contractures, exercises can be done in 4 different ways,
depending on the needs and ability of the child. These 4 ways, shown on the next
page, progress from exercises where the child depends completely on help, to
exercises that she does on her own as a part of everyday activity.
FOUR WAYS TO DO EXERCISES THAT STRETCH A TIGHT HEEL CORD
Figure
|
1. Someone else moves the limb.
Often necessary - but not much fun.
Figure
2. The child does his own exercises, but without using the
muscles in the affected part.
(This may help to prevent a contracture but will not help much
to correct it.)

Figure
Here the child does his own stretching with some help from his
mother.

Figure
Leaning against a wall stretches the feet more than standing
upright does.
Figure
If the child is strong enough, bending the knees or touching the
- toes is a good way to stretch the muscles that cause a tight heel cord.
Figure

Figure
CAUTION: When doing these exercises, carefully
check to see that the foot is not dislocating to the side.
If so, you should use Method 1, being careful to hold the foot
in such a way that it does not ‘cave in’ to the side.
Figure
3. The child does the exercise-using muscles of the affected
part.
WITH ASSISTANCE:
If the child has some strength to raise his foot, have him raise
it as far as he can. Then help him to raise it as far as it will stretch.
Developing the muscles that lift the foot may help prevent
contracture.

Figure
AGAINST RESISTANCE:
If the child has enough strength to raise his foot against
resistance, he should do so. But be sure that the foot comes all the way
up.
Figure

Figure
4. The child does the exercise - during normal daily
activities.
Figure out ways or aids so that the child can take part in
ordinary activities that stretch muscles and prevent contractures.

standing and walking uphill to
stretch heel cords

picking vegetables

Figure

Sewing on a machine can exercise
foot and combat contractures.

bar that permits child to squat
and bend ankles
|
DIFFERENT METHODS TO CORRECT CONTRACTURES
· When contractures
are just beginning to develop, stretching exercises and simple
positioning may be all that is needed to correct them.
· When contractures are more
advanced, stretching must be done steadily over a long time, using fixed
positions, casts, braces, or special equipment that keep a continuous
pull on the affected joints.
· When contractures are old
and severe, correction by surgery may be needed.
Even when contractures are advanced, it is usually best to try
to correct them as much as possible using simpler, less harsh methods first.
If a contracture is advanced:

Figure
First, correct it as far as you can with stretching
exercises and positioning.

Figure
Second, correct it as much as possible with a series of
casts or special braces.
Figure
Third, if more correction is still needed, consider
surgery.
Figure
Instructions for correcting contractures using plaster
casts or braces are in Chapter 59.
|
CAUTION: Some orthopedic surgeons
are quick to recommend surgery. However, we have found that many contractures
often said to need surgery can be corrected in the village or home by exercise
and casting or braces. In any case, stretching exercises and bracing are
often needed for a long time after surgery (or forever) to prevent the
contractures from coming back.
Also, some contractures are best left uncorrected (see Chapters
42 and 56). When in doubt, consult an experienced physical therapist. |
Exercises to correct contractures - ‘stretching
exercises’
These are similar to the range-of-motion exercises used to
prevent contractures, except that steady, gentle but firm stretching is
required:
1. Hold the limb in a steady, stretched position
while you count slowly to 25.
2. Then gradually stretch the joint a little more, and again
count slowly to 25.
3. Continue increasing the stretch in this way, steadily for 5
or 10 minutes. Repeat several times a day.

Figure
|
CAUTION: To avoid damaging the limb, hold it near the
joint, as shown. It is acceptable if the stretching hurts the child a
little, but it should not hurt him a lot. If you want faster results, do not
apply more force. Stretch the limb for longer and more times each day.
In children who do not feel in their legs, take special care
not to stretch forcefully. You could cause injuries. |
STRETCHING EXERCISE INSTRUCTION SHEETS
Some stretching exercises are done best using special
techniques. Often they need to be done at home for weeks or months. You will
find instruction sheets for the most frequently needed stretching exercises in
Chapter 42, “Range-of-motion and Other Exercises.” They include:
Stretching exercise for a tight heel cord.

Figure
Stretching exercise for a bent knee.

Figure
Stretching exercise for a bent hip.

Figure
HOLDING A CONTRACTED JOINT IN A STRETCHED POSITION FOR LONG
PERIODS
Chapter 59 discusses the use of casts, braces, and other
aids to stretch difficult contractures. These include:
|
a series of plaster casts and wedges |
adjustable braces |
elastic stretching devices |
|

Figure
|

of metal and plastic

of wood
|
Figure

Figure
|
|
Advantages: |
Advantages: |
Advantages: |
|
· Holds leg in exactly the
position you want it.
· Child (or parents) cannot
easily remove it.
· Especially useful for
difficult deformities that bend in different directions. |
|
· Can be adjusted by family at
home.
· Can be easily removed to check
for sores, for bathing, and exercise. |
|
· Same as for adjustable braces,
and also:
· Does not need frequent
adjustment because it keeps pulling as joint stretches. |
|
Disadvantages: |
Disadvantages: |
Disadvantages: |
|
· Cannot be easily removed to
check for sores, to bathe, and to exercise. (Therefore, casts should usually not
be used on children with arthritis or children without feeling in their legs.)
· Hot in warm weather.
· Expensive (plaster bandage).
· Adjustments require trip to
clinic or rehabilitation center. |
|
· More difficult to make and to
fit well.
· Difficult to use on child with
various deformities that go in different directions.
· Child (or parents) may remove
and not use it. |
|
· Clumsy - gets in the way.
· Difficult to make so they work
well.
· Often not good with
spasticity. |
HIP CONTRACTURES
Hip ‘flexion’ contractures (in which the thighs stay
bent forward at the hips) are often difficult to straighten and require special
techniques.
|
Advanced hip contractures like this often require
surgery.

Figure
|
|
Less advanced hip contractures like this can sometimes be
straightened using positioning and straps.

Figure
The child lies face down with a wide strap pulling his butt
down.

Figure
The child should spend as many hours as possible each day in
this position. And if possible, also at night. Knees should be checked for early
signs of pressure sores every hour or so. (See Chapter 24.) |
Life can be made more interesting for the child during the weeks
or months of stretching by using a lying frame on which she can move about.

Figure
(1) A rack bookholder so she can play or read.
(2) large bicycle wheels
(3) extra strong axles and hubs
(4) ‘caster’ rear wheels, for turns
(5) A bar fastened between the 2 leg casts helps keep them in a
stable position (and also helps prevent contractures that pull the legs
together).
(6) casts to straighten knees and ankles
|
CAUTION: When stretching contractures this way, be
careful to prevent pressure sores (bed sores), especially on the knees. If the
child complains a lot, loosen the strap a little. For eating, bathing, toilet,
and exercise she can be unfastened and moved into convenient positions. But it
is best that she remain strapped down about 20 out of each 24 hours. |
The child with more severe contractures at the hips may need to
be strapped on an angled frame.

Figure
For children with different angles of contracture in each hip,
the 2 leg boards can be adjusted differently.
Figure
For additional information on contractures relating to different
disabilities, aids, and equipment, see the INDEX under ‘Contractures’.
For methods to correct contractures, see Chapter
59.
Chapter 9: Cerebral Palsy
WHAT IS CEREBRAL PALSY?
Cerebral palsy means ‘brain
paralysis’. It is a disability that
affects movement and body position. It comes from brain damage that happened
before the baby was born, at birth, or as a baby. The whole brain is not
damaged, only parts of it, mainly parts that control movements. Once damaged,
the parts of the brain do not recover, nor do they get worse. However, the
movements, body positions, and related problems can be improved or made worse
depending on how we treat the child and how damaged his or her brain happens to
be. The earlier we start, the more improvement can be made.
In many countries cerebral palsy is the most frequent cause of
physical disability. In other countries it is second only to polio. About 1 of
every 300 babies is born with or develops cerebral palsy.
How to recognize cerebral palsy
EARLY SIGNS:
· At birth a baby with
cerebral palsy is often limp and floppy, or may even seem normal.

NORMAL
Child hangs in upside down ‘U’ with little or no
movement.

FLOPPY
· Baby may or may not breathe
right away at birth, and may turn blue and floppy. Delayed breathing is a common
cause of brain damage.
· Slow development
Compared to other children in the village, the child is slow to hold up his
head, to sit, or to move around.

Figure
· He may not use his hands. Or
he only uses one hand and does not begin to use both.
Figure
· Feeding problems The
baby may have difficulties with sucking, swallowing and chewing. She may choke
or gag often. Even as the child gets bigger, these and other feeding problems
may continue.

Figure
· Difficulties in taking care
of the baby or young child. Her body may stiffen when she is carried,
dressed, or washed, or during play. Later she may not learn to feed or dress
herself, to wash, use the toilet, or to, play with others. This may be due to
sudden stiffening of the body, or to being so floppy she ‘falls all over
the place’.
The baby may be so limp that her head seems as if it will
fall off. Or she may suddenly stiffen like a board, so that no one feels able to
carry or hug her.
Body stiffens like a board.
· The baby may cry a lot and
seem very fussy or ‘irritable’. Or she may be very quiet (passive) and
almost never cry or smile.
· Communication
difficulties The baby may not respond or react as other babies do. This may
partly be due to floppiness, stiffness, or lack of arm gestures, or control of
face muscles. Also, the child may be slow in beginning to
speak. Later some children develop unclear speech or other speaking
difficulties.
Although parents find it hard to know exactly what the child
wants, they gradually find ways of understanding many of his needs. At first the
child cries a lot to show what he wants. Later he may point with his arm, foot
or eyes.

Figure
· Intelligence Some
children may seem dull because they are so limp and slow moving. Others move so
much and awkwardly they may appear stupid. Their faces twist, or they may drool
because of weak face muscles or difficulty swallowing. This can make an
intelligent child appear mentally slow.
About half of the children with cerebral palsy are mentally
retarded, but this should not be decided too soon. The child needs to be given
help and training to show what she is really like. Parents can often tell that
she understands more than she can show.
Figure
|
With help and training, some children who have been
considered retarded prove to be quite intelligent. |
· Hearing and sight are
sometimes affected. If this problem is not recognized, the family may think that
the child lacks intelligence. Observe the child carefully and test him to find
out how well he can hear and see.
Even if a child can hear loud banging, he may not hear well
enough to understand words.

Figure
· Fits (epilepsy,
seizures, convulsions) occur in some children with cerebral palsy. (See Chapter
29.)
· Restless behavior
Sudden changes of mood from laughing to crying, fears, fits of anger, and other
difficult behavior may be present. This may partly be due to the child’s
frustration of not being able to do what he wants with his body. If there is too
much noise and activity the child can become frightened or upset. The brain
damage may also affect behavior. These children need a lot of help and patience
to overcome their fears and other unusual behavior. (See Chapter 40.)
· Sense of touch, pain, heat,
cold, and body position are not lost. However, the children may have trouble
controlling movements of their bodies and trouble with balance. Because
of their damaged brains they may have difficulty learning these things. Patient
teaching with lots of repetition can help.
· Abnormal reflexes
Babies have certain ‘early reflexes’ or automatic body movements that
normally go away in the first weeks or months of life. In children with brain
damage, they may last much longer. However, these are only important if they
affect how the child moves. ‘Knee jerk’ and other tendon-jump
reflexes are usually over-active (jump higher than normal). If you are not
sure, testing for abnormal reflexes may help you tell cerebral palsy from polio.
TYPES OF CEREBRAL PALSY
Cerebral palsy is different in every child. Different
experts have worked out different ways of describing it. But do not worry about
labeling a child’s particular type of cerebral palsy. This does not usually
help his treatment.
It is helpful, however, to recognize 3 main ways that cerebral
palsy can appear. In a particular child, it may appear in one or another of
these ways - but usually in some sort of combination.
1. MUSCLE STIFFNESS OR ‘SPASTICITY’
The child who is ‘spastic’ has muscle
stiffness, or ‘muscle tension’. This causes part of his body to be
rigid, or stiff. Movements are slow and awkward. Often the position of the head
triggers abnormal positions of the whole body. The stiffness increases when the
child is upset or excited, or when his body is in certain positions. The
pattern of stiffness varies greatly from child to child.
TYPICAL SPASTIC POSITIONS WHEN LYING ON THE BACK:
Figure
Stiffness, with the knees bent or with legs separated, occurs
more commonly in the child with spasticity and athetosis combined (see below).

Figure
Less commonly the head and shoulders may stiffen forward...

Figure
... or the arms may stiffen straight across the body, with the
head pressed back.
Figure

Figure
When you try to stand the child the legs often stiffen or
cross like scissors (1).

Figure
The child who learns to walk may do so in a stiff,
awkward position, with the knees pulled together and bent (1). Feet often turn
in.
2. UNCONTROLLED MOVEMENTS OR ‘ATHETOSIS’
These are slow, wriggly, or sudden quick movements of the
child’s feet, arms, hands, or face muscles. The arms and legs may seem
jumpy and move nervously, or just a hand or the toes may move for no reason.
When he moves by choice, body parts move too fast and too far. Spastic movements
or positions like those shown above may continually come and go (constantly
changing muscle tension). His balance is poor and he falls over easily.
Most children with athetosis have normal intelligence, but if
the muscles needed for speech are affected, it may be hard for them to
communicate their thoughts and needs.
Typical athetoid arm and hand movements may be as a regular
shake or as sudden ‘spasms’. Uncontrolled movements are often worse
when the child is excited or tries to do something.

Figure
This child has severe
athetosis.
3. POOR BALANCE OR ‘ATAXIA’
The child who has ‘ataxia’, or poor balance, has
difficulty beginning to sit and stand. She falls often, and has very clumsy use
of her hands. All this is normal in small children, but in the child with ataxia
it is a bigger problem and lasts longer (sometimes for life).
Because children who have mainly a balance problem often appear
more clumsy than disabled, other children are sometimes cruel and make fun of
them.
To keep her balance the child with ataxia walks bent forward
with feet wide apart. She takes irregular steps, like a sailor on a rough sea or
someone who is drunk.

Figure
|
TEST FOR ATAXIA:
Hold a finger or a toy in front of the child and ask him to
touch it on the first try. The child with ataxia cannot do it.
Figure
|
Many children who have spasticity or athetosis also have
problems with balance. This may be a major obstacle in learning to walk.
However, much can often be done to help a child improve her balance.
|
NOTE: Children with any type of cerebral
palsy as babies are often mainly limp or floppy. Stiffness or
uncontrolled movements begin little by little. Or the child may be limp in some
positions and stiff in others. |
Parts of the body affected
DEPENDING ON WHICH LIMBS ARE INVOLVED, THERE ARE 3 TYPICAL
PATTERNS:

ARM AND LEG ON ONE SIDE
(HEMIPLEGIC)

BOTH LEGS ONLY (PARAPLEGIC) or
with slight involvement elsewhere (DIPLEGIC)

BOTH ARMS AND BOTH LEGS
(QUADRIPLEGIC)
Although most cerebral palsy children fit one or another of
these patterns, check also for minor problems in other parts of the body.
QUESTIONS ABOUT CEREBRAL PALSY
1. What causes it?
In each child with cerebral palsy, the parts of the brain that
are damaged are different. The causes are often difficult to find.
· Causes before birth:
· Infections
of the mother while she is pregnant. These include German measles and
shingles (herpes zoster).
· Differences between the blood
of mother and child (Rh incompatibility).
· Problems of the mother, such
as diabetes or toxemia of pregnancy.
· Inherited. This is
rare, but there is a ‘familial spastic paraplegia’.
· No cause can be found
in about 30% of the children.
· Causes around the time of
birth:
· Lack of oxygen
(air) at birth. The baby does not breathe soon enough and becomes blue and
limp. In some areas, misuse of hormones (oxytocics) to speed up birth narrows
the blood vessels in the womb so much that the baby does not get enough oxygen.
The baby is born blue and limp - with brain damage.
· Birth injuries from
difficult births. These are mostly large babies of mothers who are small or very
young. The baby’s head may be pushed out of shape, blood vessels torn, and
the brain damaged.
· Prematurity. Babies
born before 9 months and who weigh under 2 kilos (5 pounds) are much more likely
to have cerebral palsy. In rich countries, over half the cases of cerebral palsy
happen in babies that are born early.
· Causes after birth:
· Very high
fever due to infection or dehydration (water loss from diarrhea). It is more
common in bottle-fed babies.
· Brain infections
(meningitis, encephalitis). There are many causes, including malaria
and tuberculosis.
· Head injuries.
· Lack of oxygen from
drowning, gas poisoning, or other causes.
· Poisoning from lead
glazes on pottery, pesticides sprayed on crops, and other poisons.
· Bleeding or blood clots in
the brain, often from unknown cause.
· Brain tumors. These
cause progressive brain damage in which the signs are similar to cerebral palsy
but steadily get worse.
2. Is cerebral palsy contagious? No! It cannot be passed
from one child to another.
3. Can persons with cerebral palsy marry and have
children? Yes. And the children will not have the condition (except maybe in
a very rare type of cerebral palsy).
4. What medical or surgical treatment is there?
Except for drugs to control fits, medicines usually do not help.
(Although medicines to reduce spasticity are often prescribed, they usually do
no good, and may cause problems.) Surgery is sometimes useful for correcting
severe, stubborn contractures. However, surgery to weaken or release spastic
muscles is less often effective and sometimes makes things worse. Careful
evaluation is needed. Surgery usually should be considered only if the child
is already walking and has increasing difficulty because of contractures. In
a child who cannot balance well enough to stand, surgery usually will not help.
Sometimes surgery to separate the legs can help make cleaning and bathing
easier.
5. What can be done?
The damaged parts of the brain cannot be repaired, but often the
child can learn to use the undamaged parts to do what she wants to do. It is
important for parents to know more or less what to expect:
|
The child with cerebral palsy will become an adult with
cerebral palsy. Searching for cures will only bring disappointment. Instead,
help the child become an adult who can live with her disability and be as
independent as possible. |
Families can do a lot to help these children learn to function
better. Generally, the child who is more intelligent will learn to adapt
successfully to her condition. However, intelligence is not always
necessary. In fact, some intelligent children become more easily frustrated and
discouraged, so they stop trying. Extra effort is needed to find new and
interesting ways to keep them progressing. Even severely retarded children
can often learn important basic skills. Only when mental damage is so great
that the child does not respond at all to people and things is there little hope
for much progress. However, before judging the child who does not respond, be
sure to check for deafness or loss of eyesight.
|
IMPORTANT: Rather than try to treat the
symptoms of cerebral palsy, we can do more for the child if we help her with
development of movement, communication, self-care and relationships with
others. Sometimes we can partly correct the symptoms through helping the
child develop basic skills. |
Family members can learn to play and do daily activities with
the child in ways that help her both to function better and to prevent secondary
problems such as contractures.
Most important is that the parents (and grandparents!) learn
not to do everything for the child. Help her just enough that she can learn to
do more for herself.
By standing on her knees as she paints a sign, this girl is
improving her balance to help her (possibly) stand and walk.

Figure
For example, if your child is beginning to hold up her head, and
to take things to her mouth,

instead of always feeding her
yourself

look for ways to help her begin
to feed herself.
6. Will my child ever be able to walk?
This is often one of the biggest concerns of parents. Walking is
important both functionally and socially. But in terms of the
child’s needs, other skills may be more important. For the child to lead as
happy, independent a life as possible, necessary skills and accomplishments (in
order of importance) are:
1. Having confidence in yourself and liking
yourself
2. Communication and relationship with others
3. Self-care
activities such as eating, dressing, toileting
4. Getting from place to
place
5. (And if possible) walking
We all need to realize that walking is not the most important
skill a child needs - and it is certainly not the first. Before a child can
walk he needs reasonable head control, needs to be able to sit without help, and
to be able to keep his balance while standing.
Most children with cerebral palsy do learn to walk, although
often much later than normal. In general, the less severely affected the
child is and the earlier she is able to sit without help, the more likely she is
to walk. If she can sit without assistance by age 2, her chances for walking may
be good - although many other factors are involved. Some children begin to walk
at age 7, 10, or even older.
Hemiplegic and diplegic children usually do learn to walk,
although some may need crutches, braces, or other aids.
Many severely affected children may never walk. We need
to accept this, and aim for other important goals. Whether or not the child
may someday walk, he needs some way to get from place to place. Here is a
true situation that helped us to realize that other things are more important
than walking.
|
The legs stiffen and the feet go into a rigid tiptoe position.
This child is not almost ready to walk.

Figure
A COMMON MISTAKE
When a child with severe brain damage is held like this, her
legs may automatically stiffen and her feet point down - the so-called
‘tiptoe reflex’. Because the feet sometimes take jerky
‘steps’, parents think the child is ‘almost ready to walk’.
This is not so. The tiptoe reflex must be overcome before the child can begin to
learn to walk. Do not hold the child in this position or make her try to walk.
It will only strengthen this disabling reaction. |
In a Mexican village, we know 2 brothers, both with cerebral
palsy.
Petronio walks but with great difficulty. Walking tires him and
makes him feel so awkward that he stays at home and does not play or work. He is
unhappy.
Figure
His brother, Luis, cannot walk. But since he was small, he has
loved to ride a donkey. He uses a wall to get off and on by himself. He goes
long distances and earns money carrying water. He is happy.

Figure
(Not only does the donkey take Luis where he wants to go, but by
keeping his legs apart, it helps prevent knock-knee contractures. This way
‘therapy’ is built into daily activity.)
There are many different ways to help children who cannot walk,
or who walk with difficulty, get where they want to go. These include
wheelboards, wagons, wheelchairs, special walkers, and hand-pedal
tricycles. Many of these are described in PART 3 of this book (see the
Index).
How can we help?
First, with the help of parents and family we observe the child
carefully to see:
· what the child
can do.
· what he looks like when
he moves and when he is in different positions.
· what he cannot do, and what prevents
him from doing it.

A village worker and father
examine a child with severe cerebral palsy.
WHAT THE CHILD CAN DO
Can the child:
· lift her head?
hold it up? sit? roll over?
· pull herself
along the floor in any way possible? crawl? walk?
How does the child use her hands?
· Can she grasp
things and hold on; let go; use both hands together (or only one at a
time)?
· Can she use her fingers to pick up
small stones or pieces of food?
How much can the child do for herself?
· Can she feed
herself; wash herself; dress herself? Is she ‘toilet
trained’?
What can the child do in the home or in the fields to help the
family?
After observing and discussing what the child can do, we
must expect him to do these things. If the parents are used to doing
almost everything for the child, at first this may be difficult (for both
parents and child). But soon it will help the child have more confidence. The
parents, also, will be encouraged by seeing what he can do for himself, and they
will think less about what he cannot do. Here a grandmother helps her grandchild
became more self-reliant:

Figure

Figure
It was difficult for the grandmother not to bring her grandson a
cup of water - especially when he begged her. But she understood that in the
long run it would do him more good to manage for himself. For more ideas about
how a family can help a child with cerebral palsy, read the story of Maricela on
pages 5 to 7 and the story of Enrique.
HELPING THE CHILD ACHIEVE BETTER POSITIONS
Due to abnormal pull of muscles, children with cerebral palsy
often spend a lot of time in abnormal positions. These abnormal positions of the
limbs and body should be avoided as much as possible, or the child can become
deformed. For example,

Figure
A wrist (1) or elbow (2) that is always bent can lead to
contractures (muscle shortening) that make it impossible to straighten the arm
or hand.
Hips (3) that are continually bent forward, or to one side, or
knees (4) that are always held together, or never completely straightened, or
feet (5) that are always ‘tiptoe’, can lead to contractures that
prevent the normal range of movement. This can make washing, dressing,
toileting, and moving about much more difficult.

Figure
A twisted position can lead to curvature of the
spine and tilting of the hips (6).
If the head is always turned or bent to one side (7), in time
the neck may become permanently twisted.
An arm that is held tightly to the side will in time become
difficult to raise away from the side (8).
Whenever possible the child should be in positions that prevent
rather than cause these problems. Whatever the child is doing (lying, sitting,
crawling, standing) try to encourage positions so that:
· her head is
straight up and down.
· her body is straight
(not bent, bowed, or twisted).
· both arms
are straight and kept away from the sides.
·
both hands are in use, in front of her eyes.
· she bears weight equally on both sides of her body -
through both hips, both knees, both feet or both arms.

sitting

crawling

lying

standing
Encourage positions that the child can manage at her stage of
development. Play with her, talk with her, give her interesting things to do in
these positions.
Not all children will be able to stay in these positions without
some kind of support. Special chairs, tables, wedges, pads, or bags of clean
sand may be needed to keep a good position.
For example, the child at the top of the page might need a chair
like this.
Figure
Note: Remove straps and supports as soon as the child is
able to stay in a good position.
|
WARNING: Do not leave a child in any one
position for many hours as his body may gradually stiffen into that position.
Change his position often. Or better, encourage him to change it. If he can
change his own position effectively, then chairs, seats, and other aids must not
prevent him from moving.
AIDS SHOULD RESTRICT A CHILD’S MOVEMENT AS LITTLE AS
POSSIBLE. |
When the child with cerebral palsy moves she may do so in a very
strange or abnormal way. To some extent this should be allowed, as long as the
child is able to do things as best she can. But also show the child other ways
to move in order to correct some of the abnormal positions that she repeats
again and again. For example,
If her arm repeatedly bends up,

Figure
encourage her to reach out and hold objects.

Figure
Or she may need a post to hold on to.
Figure
If she bends backward a lot,
Figure

Figure
she needs actions that bend her head, body, and shoulders
forward, like these (1).
Corrective actions and positions can be found while
working in the fields, in the home, or while playing with brothers and sisters.
Here are some more suggestions for corrective positions (from physical
therapists Nancy Finnie and Sophie Levitt).
Lying and sleeping
Try to find ways for the child to be in positions that
correct or are opposite to his abnormal ones.
Figure

Figure

Figure
If the child’s body often arches backward,

Figure
try positioning him to lie and play on his side.

Figure
Look for ways to break the spasticity by bending him forward,
Figure
or over a barrel (or beach ball or big rock, etc.),

Figure
or in a car tire swing.
Figure
If the child does not have enough control to reach out in this
position,

Figure
help position him so he can lift his head using his arms.
Figure

Figure
If the child’s head always turns to the same side,
Figure
do not have him lie so that he turns his head to
that side to see.

WRONG
Instead, have him lie so that he has to turn his head to the
other side to see the action.

RIGHT
Rolling and twisting
A child with cerebral palsy is often very stiff when it comes to
twisting or rotating the main part of her body. However, such twisting is
necessary for learning to walk. Rolling also helps develop body twisting.
If the child is very stiff, first help her ‘loosen up’
by swinging her legs back and forth.

Figure
Then help her learn to twist her body and roll.

Figure
Figure out games so that the child wants to
twist, and does it without help.

Figure

Figure
Sitting
The way that you help position a child for sitting also depends
on the type of abnormal body positions he has. For example,
If his legs push together and turn in, and if his shoulders
press down and his arms turn in,

Figure
sit him with his legs apart and turned outward.
Also lift his shoulders up and turn his arms out.

Figure
Look for simple ways to help him stay and play in the improved
position without your help.

Figure
Sitting with the legs in a ring helps turn hips outward.

Figure
For the child with spasticity who has trouble sitting, you can
control his legs like this. This leaves your hands free to help him control and
use his arms and hands. Help the child feel and grasp parts of his face.

Figure
Sit the child on your belly with his legs spread and feet flat.
Give support with your knees as needed. As he begins to reach for his face, help
his shoulders, arms, and hands take more natural positions. Make a game out of
touching or holding parts of his face. MAKE IT FUN!
Figure
As the child develops, encourage her to put her arms and body in
more normal positions through play and imitation.

Figure
Children who have trouble with balance (from cerebral palsy,
polio, or other disability) often sit with their legs in a ‘W’ in
order not to fall over.

Figure
Sitting in a “W” should usually be discouraged
because it can increase contractures and loosen or damage hips and knees.
However, if it is the only way a child can sit and use her hands, it should be
allowed.

Figure
Look for ways for the child to sit with legs spread forward.
Here are 2 examples.
The pot or log keeps the knees apart. The holes for heels help
too.

Figure
Figure
If the child’s legs stay apart, his butt sticks out, and
his shoulders are pulled back,

Figure
first sit him with his body bent forward and his legs together.
Then bend his shoulders forward and turn them in.

Figure
A sack of grain provides a roll to hold this child’s legs
apart. Her father pushes down on her knees. This helps her to hold her feet flat
and sit up straighter. (PROJIMO)

Figure
Look for ways that the child will sit and play in the improved
position without help.
Play with her at a table. Sit across from her to have her reach
forward for toys with both hands.

Figure
Be sure her feet are on a flat surface.

Figure
For ideas on special seats and sitting positions to prevent
‘knock-knee’ contractures, see below.
Moving about
Because children with cerebral palsy are usually delayed in
walking, they need other ways to get from place to place. The methods used will
depend on both the needs and abilities of the child - also the resources,
skills, and imagination of family, friends, and local craftspersons.
Aids for ways to get from place to place should provide
corrective positions. The following examples are all designed to help
prevent ‘knock-knee’ contractures. They also provide other types of
corrective positioning.
Figure

Figure

Figure
Wheel boards
Adapting wheel boards for travel on rough surfaces

Figure
By placing large wheels (1) near the middle, if the smaller
front caster gets stuck, the child can lift with his arms and go on. Or if a
fixed front wheel is used, he can lift it off the ground to make turns.
For dirt or bamboo floors, larger wheels will be needed.
Some children will need wheelchairs. For wheelchair designs,
see Chapters 64, 65 and 66.
Figure
Standing
Many children with cerebral palsy stand and walk in strange
positions. A child’s unsure balance often increases the uncontrolled
tightening of certain muscles and makes balance even more difficult.
As a result the child stands in an awkward position that can
lead to deformities and contractures.
Figure
When you help the child keep her balance, she is less tense and
can stand straighter.

Figure
Look for ways to provide similar assistance during play and
other activities.
Here a cart provides easier balance and keeps the arms straight.
Figure

Miguelito began to walk at age 8
- first on parallel bars.

Soon he learned to use crutches.
Here he races another child who is learning to walk.

And now he can walk alone.
Two sticks can help the child once she develops some standing
balance. At first you can hold the tops of the sticks. But let go as soon as
possible.

Figure
|
CAUTION: Be sure sticks are taller than
child so that she will not injure herself if she falls. |
The child who cannot yet stand alone can be placed in a standing
frame for an hour or 2 each day.
Figure
Figure

Figure
Even for the child who may never stand alone or walk, standing
in a frame helps prevent deformities. It also helps the leg bones grow and stay
strong. Start at about the age normal children begin to stand - around one year
old.
Hand use
Try to find ways that the child can play or do things using her
hands while she is in the corrective positions of sitting, standing or lying.
Encourage her to touch, feel, and handle as many different
shapes and surfaces as possible: things that are big, small, hot, cold, sticky,
smooth, prickly, hard, soft, thin, and thick.
This girl in the rehabilitation center of the Khao-i-dang
refugee camp in Thailand develops hand control by sliding colored rings on a
pole.

Figure

A boy with cerebral palsy at the
PROJIMO rehabilitation center helps paint a chair frame.
CORRECTIVE CARRYING POSITIONS
As in other activities, try to carry a child in positions that
work to correct abnormal positions.
If the child usually lies with arms bent and legs straight,

Figure

do not carry him like this.
Carry him in ways that straighten his arms and bend his knees
and hips.

Figure
As the child gains more control, you can carry him with less
support.

Figure
|
The child with spasticity who is usually curled up,

Figure
can be carried like this.
Figure
|
The child with severe spasticity who tends to straighten and
arch backward can be carried like this.
Figure
For play, you can swing the child in the air in this position.

Figure

Figure
CONTRACTURES IN CEREBRAL PALSY
Abnormal muscle tightness often leads to contractures (muscle
shortening and reduced motion of joints, see Chapter 8). In time, the muscles
that keep a limb bent become shortened so that the limb cannot straighten even
when the muscles relax. But with care, contractures can often be prevented.
|
Without care to prevent it: |
|
SPASTICITY
(Uncontrolled tightening of muscles) |
leads to
® |
CONTRACTURE
(Fixed shortening of muscles) |
The typical contractures of cerebral palsy are similar to
the abnormal positions of cerebral palsy. They can include:

Figure
(1) neck contractures that pull the head back
or to one side
(2) sway back
(3) bent-hip contracture
(4)
bent-knee contracture
(5) ‘tiptoe’ contracture
(6)
An arm and hand that are always bent may cause contracture of elbow
and wrist.
(7) ‘knock-knees’ contracture
(8) Ankle and
toot contractures may bend IN, DOWN, UP or OUT depending on the
spasticity.
Stretching the knees apart you can see and feel the very tight
cord in the groin.

Figure
Chapter 8 discusses contractures, and ways to prevent and
correct them. Page 79 explains how to tell spasticity from contractures.
Spasticity and contractures combined
Decreased range of motion may be caused partly by spasticity and
partly by contractures. Therefore, whenever a child has spasticity, check to see
if contractures are also forming, and if so, how much.
This girl with cerebral palsy has spastic muscles that hold her
knees tightly together.

Figure

Figure
When she is helped to relax and her legs are slowly separated,
they will only open this far (1).
Normally her legs should open this far (2). This means she has
contractures on the inner side of her thighs (groin).
One way to record spasticity and contractures:

Normal
With Contracture

With Spasms
You can use a flexikin to record the positions.

Figure
PREVENTING CONTRACTURES
In cerebral palsy, it is important that steps to prevent
contractures be included in activities that help the total development of the
child. Many of the corrective positions we have already suggested for
activities such as lying, sitting, standing, and moving about are helpful in
preventing contractures. When there are signs of developing contractures, give
even more time and care to corrective positions.
Range-of-motion exercises
Although the reasons contractures form in cerebral palsy and
polio are different, many of the stretching and holding exercises discussed in
Chapter 8, “Contractures,” and in Chapter 42, “Range-of-Motion
and Other Exercises,” will be helpful. However, in cerebral palsy, take
care to do exercises in ways that do not increase spasticity, but help to
relax the spastic muscles.
RELAXING SPASTIC MUSCLES
To help relax spastic muscles, before beginning
range-of-motion exercises try the following to see what works best for your
child:
1. Apply warm soaks to spastic muscles or have the
child sit or lie in warm water.

Figure
2. Slowly twist or help the child to twist his body
from side to side. This reduces spasticity throughout the body, and is a good
first stretching exercise: Make it into a game.

Figure
|
CAUTION
ABOUT MASSAGE
In some countries, people and even therapists use massage, or
rubbing, to try to relax spastic muscles. Although massage often helps relax
muscle spasms, cramps, or tight muscles from other causes, in spasticity,
massage usually increases the muscle tightness. As a general rule. DO NOT
MASSAGE SPASTIC MUSCLES. |
Pulling or pushing directly against spastic muscles causes
them to tighten more. To correct abnormal positions, sometimes you can use
‘tricks’ to release or ‘break’ the muscle spasms.
Muscle tension in any part of the body is affected by the
position of the head and body. Spasms that straighten the legs and pull the
knees together can be partly relaxed by bending the head and back forward.
Do not pick up the child like this. Her head will bend back and
her whole body and legs stiffen more.

WRONG
If you roll her a little to one side, it will be easier to bend
her head and back forward, This relaxes her hips and legs so that they also
bend.
RIGHT
Whatever you do with the child, look for ways that will help
relax and stretch the tight muscles. Here are some examples.
Rosa’s body stiffens backward, while her knees straighten
stiffly and press together.
To wash between her legs, do not try to
pull her legs apart at the ankles.
This will make her legs pull together more tightly

WRONG
Instead, put something under her head and shoulders to bend them
forward. This helps to relax the stiffness in her whole body.
Then bend the legs and slowly separate them. If you hold them
above the knees, they will open more easily

Figure
Washing will be easier with her knees bent. After washing her
(with warm water, if possible) you can help stretch the tight muscles.
Slowly open her legs as wide as they will go, and then gradually
straighten her knees.

Figure
When you try to feed the child, if her head and shoulders
stiffen backward,
Figure
do not try to pull her head forward. It
will push back more.

WRONG
You may find that her head relaxes more if you put your arm
across the back of her neck and push her shoulders forward.

Figure
Or, you may find that raising the front of the chair seat keeps
her hips bent, relaxes her in general, and gives her much more control.
Figure
When you want to help your child dress, if her arms press
against her chest,

Figure
do not try to pull them straight. They will
stiffen more.
WRONG
Try holding her arms above her elbows, and gently turning her
arms out and straighten them at the same time.
Figure
Note: These suggestions will work for some children
but not for others. Keep trying different ways until you find what works
best.
DEVELOPING EARLY SKILLS
Most children with cerebral palsy develop basic skills and
abilities more slowly than other children. This is partly because of their
difficulty with balance and movement. Also, in some children, mental slowness or
problems with seeing or hearing make learning more difficult. Because slow
development occurs with many different disabilities, we discuss activities for
child development in a separate section of this book.
In this chapter, therefore, we give only a few suggestions for
assisting a child with cerebral palsy to learn new skills.
|
VERY IMPORTANT:
To understand better how to help a child with cerebral palsy
develop early skills, you also need to read other chapters. Chapters 34
and 35 are about helping the child whose mind and/or body are slow to
develop. Chapters 36 to 41 discuss ways of helping children develop and
become more self-reliant.
Although Chapters 34 to 41 are written to help any children who
are slow to develop, many suggestions are included for the specific needs of the
child with cerebral palsy. These are marked with in the
margin. |
To help a child develop new skills, first observe all the things
that she can and cannot do. Like a normal baby who progresses stage by stage in
a certain order, the child with cerebral palsy must do the same. Charts showing
the normal ‘developmental milestones’ are on pages 292 and 293. You
can use them to help decide the next steps or skills that the child may be ready
to learn.
Help the child advance slowly, at her own speed, in small steps.
If we try to go too fast because of her age, she can become discouraged by
failure. Also, her progress can be held back. This happens when we stand a child
and try to make him walk before he is ready.
|
Move ahead at a speed that fits your child - not too fast and
not too slow. |
To help a child with cerebral palsy develop skills takes a lot
of time, energy, patience, and love. The whole family needs to help, and also,
if possible, others in the community. (See Chapter 33.)
Remember that positioning is very important. When the
child has been helped to lie, sit, and stand in ways that give him better
positions and control, he will start learning to do things he could not do
before.
Good balance is one of the most important goals for the
development of the child with cerebral palsy. It is important to help a child
improve her balance from as young an age as possible. At each stage of the
child’s development - lying, sitting, creeping, standing, and walking -
better balance is needed to progress to the next stage.
Helping improve balance
Detailed suggestions of activities to improve balance are
included in Chapter 35, “Early Stimulation Activities,” especially
pages 306 to 312. Here we give you a brief look at some of the basic suggestions
explained in more detail in that chapter.
|
TESTING A CHILD’S BALANCE |
|
POOR BALANCE
|

BETTER BALANCE
|

GOOD BALANCE
|
|
If when you sit a child over 10 months old, she falls stiffly to
one side with no effort to ‘catch’ herself, her balance is poor. |
If she can balance using her arms when you gently push her, her
balance is fair. |
If she can do it by bending her body, without using her arms,
her balance is good. |
When lying
Encourage the child to shift weight from one arm to the other by
reaching for objects,
reaching forward,
Figure
and reaching sideways.

Figure
Lie him on your body and tip a little from side to side so that
he begins to catch himself.
Figure
When sitting
Let her start to fall so that she begins to catch herself.
Figure
Sit her across your knees. Raise one knee so she has to balance.

Start with hands high.

Then lower your hands.
As the child improves, use a tilting board.

Figure
Encourage the child to twist and reach to the side.

Figure
Use as little sitting support as needed. Often low back support
is enough for a child who straightens stiffly

Figure
For creeping and crawling
Note: Some children advance to standing
without ever crawling.
Shift weight from one arm to the other. Provide support as
needed, and gradually take it away

Figure

Figure
Shift weight from one leg to the other.

Figure
Play trying to balance on a tipping surface.

Figure
Crawl forward, sideways, and backward.

Figure

crawling scooter
For standing and walking
Stand and balance on knees.

Figure
CAUTION: Not for a child with bent-knee
spasticity.
Pull to stand.
(Often the child will stand better when he pulls himself up than
when someone helps him.)
Stand while holding on, and reaching.

Figure
Help with standing and then walking.

Figure
Give less and less support while he walks with only a
‘safety-belt’-and then alone.

Figure
Have the child practice stepping forward, backward, and
sideways.

Figure
Whenever possible, turn these activities into games. Talk to
the child a lot while you do them to help develop language skills at the
same time.
Skills for daily living and self care
A child with cerebral palsy will get abilities later than other
children - but she will get them! Of course, the child may not achieve
everything, and may not always walk. But make sure the child achieves what
she can in each important area of development:
The child will often need a lot of help with language and
communication skills. Develop these skills in whatever way seems possible:
using words, gestures, pointing (with hand, foot, head, or eyes), or with
communication boards. (See Chapter 31)

Figure
Help the child become as independent as possible in eating,
dressing, washing, toileting, and in meeting other daily needs. Do
this by guided practice, imitation, and step-by-step learning. These self-care
skills are discussed in Chapters 36 to 39.
Develop some form of moving about and, if necessary, use
wheel-boards, wheelchairs, pedal tricycles, walkers, crutches, or other aids.
(See Chapters 63, 64, 65, and 66.)
Keep experimenting until you find what works best.
For example, this girl, with poor body and hip control, tends to
‘fall through’ the space between her arms when the handgrips on the
walker are upright.

Figure
She does much better on a higher walker with a handgrip that
runs from one side to the other.

Figure
Often leg braces do not help a child with cerebral
palsy walk better. But sometimes they do. When in doubt, try low-cost braces
first, to look for possible problems. For example:
Carla walks in a very crouched position.

Figure
She may be helped by below-knee braces that hold her feet at
nearly a right angle (90°)

Figure
or by above-knee braces that keep her knees almost straight...

Figure
But it is possible that the below-knee braces will throw her
badly off balance,

Figure
and that the above-knee braces will make balancing even harder.
You will need to experiment!
Figure
Even if braces for walking do not work, Carla may be helped to
walk straighter by using ‘night splints’ to hold her knees straight
and prevent contractures.
|
IMPORTANT: Practice in learning skills
should take place with family and friends so that the child develops skills in
relating to others. However, the child will also need time to practice her
skills alone and with the person who is mainly responsible for treating or
teaching her. |
|
CAUTION: Many suggestions for developing
basic skills are discussed in Chapter 34, “Child Development and
Developmental Delay,” and Chapters 36 through 39 on developing skills for
self-care. However, for the child with cerebral palsy, some of these
activities will need to be done differently to help reduce and not increase
muscle spasms. If any activity increases spasticity, try it differently until
you find a way that reduces muscle tension and improves position. |
PREVENTION
With these precautions, children will be less likely to have
cerebral palsy:
· Good nutrition of the
mother, both before and during pregnancy, reduces the chance of premature
birth - and of cerebral palsy.
· If possible, girls should
avoid pregnancy until full grown (16 or 17 years old).
· Avoid unnecessary medicines
during pregnancy.
· Try to avoid getting
near persons with German measles during pregnancy. Or get vaccinated
against German measles before becoming pregnant.
· Go for regular health
check-ups during pregnancy (prenatal care). If there are any signs that
giving birth may be difficult, try to arrange for a skilled midwife or doctor to
attend the birth - if possible, in a hospital. (See the list of “Signs of
Special Risk,” Where There Is No Doctor, p. 256.)
· During labor, do not let the
midwife try to speed things up by,

pushing forcefully against the
womb,

or by using injections or
hormones (oxytocin, pituitrin, etc.) before the child is born.
· Be familiar with, and be sure
your midwife is familiar with, all the precautions and emergency measures
of childbirth. Learn what to do if the baby is born blue and limp and does not
breathe right away, or has the cord wrapped around the neck. (See Where
There Is No Doctor, p. 262.)
· Breast feed the baby
(breast milk helps prevent and fight infection), and make sure the baby gets
enough to eat. (See Where There Is No Doctor, p. 121 and
271.)
· Vaccinate the baby
(especially for measles).
· When the baby has a
fever,

uncover him completely.
If the fever is high, wet the child and fan him until he is
cooler.
Never wrap the baby up in clothing or blankets.

Figure
This can make the fever worse and cause fits or permanent brain
damage.
Be sure the child with fever drinks a lot of liquids, and follow
the other instructions on pages 75 to 76 of Where There Is No
Doctor.
· Know the signs of
meningitis and get (or begin) treatment quickly.

Figure
· When your baby has
diarrhea, prepare Rehydration Drink and give it to him every few minutes to
prevent or correct dehydration. See Where There Is No Doctor,
p. 151 to 161.
|
Preventing dehydration helps prevent fits and brain damage
(cerebral palsy). |

Figure
OTHER PARTS OF THIS BOOK WITH INFORMATION CONCERNING CEREBRAL
PALSY
Cerebral palsy is a complex disability that involves many
problems and needs. Therefore much of the basic information you will need is in
other chapters. It is essential that you read Chapters 4, 8, 33 to 43, and 62 to
66.
Throughout the book, important information about cerebral
palsy has been marked with a in the margin.
Many references to cerebral palsy are also included in the
INDEX.
Chapter 10: Muscular Dystrophy: Gradual, Progressive Muscle Loss
Muscular dystrophy is a condition in which
muscles, month by month and year by year, get weaker and weaker.
Because the disability gradually gets worse, we say it is
‘progressive’.
HOW TO RECOGNIZE IF MUSCLE WEAKNESS IS CAUSED BY MUSCULAR
DYSTROPHY
· Mostly affects boys (rarely
girls).
· Often brothers or male
relatives have same problem.
· First signs appear around ages
3 to 5: the child may seem awkward or clumsy, or he begins to walk
‘tiptoe’ because he cannot put his feet flat. Runs strangely. Falls
often.
· Problem gets steadily worse
over the next several years.
· Muscle weakness first affects
feet, fronts of thighs, hips, belly, shoulders, and elbows. Later, it affects
hands, face, and neck muscles.
· Most children become unable to
walk by age 10.
· May develop a severe curve of
the spine.
· Heart and breathing muscles
also get weak. Child usually dies before age 20 from heart failure or pneumonia.
Figure
Early common sign of muscular dystrophy

Figure
· To get up from the ground, the
child ‘walks up’ his thighs with his hands.
This is mainly because of weak thigh muscles.
QUESTIONS ABOUT MUSCULAR DYSTROPHY
How common is it? It is not very common.
Rehabilitation centers may see one child with muscular dystrophy
for every 30 or 40 with cerebral palsy or polio.
What causes it? Nobody knows. But in 2 out of 3 families
with muscular dystrophy, there is a history of it among male relatives of the
mother. Though the parents are usually normal, the mother carries the
‘gene’ that produces dystrophy in her sons. Her daughters will develop
normally, but they may have sons with muscular dystrophy.
What treatment is there? None. No medicines help. Special
therapy or exercises will not stop the weakness from increasing. Surgery to
release tiptoe contractures is at best of temporary benefit.
The family can, however, do much to help the child make the best
of his life and adapt to his limitations as they progress.
Also, activities, exercises and braces to prevent contractures
may help the child to keep walking longer. If the child sits in a bad position,
pillows or supports to help him sit straighter can help prevent deformities.

Figure
Is the child’s mind affected? About half of these
children are somewhat mentally retarded (slow learners); some are very
intelligent.
What can be done? The family can do many things to help
the child live more fully and happily. The child should remain active and
continue normal activities for as long as possible. Play with other children is
important. So are learning and exploring. The child should go to school.
Encourage other children to help him with learning and play. The teacher should
realize that some - but not all - children with dystrophy learn a little more
slowly than normal. Try to include the child in as many family and community
activities as possible.
The steadily increasing weakness and the lack of effective
treatment will be hard for both the family and child to accept. Friendly
assistance, advice, and encouragement from health workers and friends can be a
big help. Help the family to look at the situation honestly, and to do their
best.
A boy with muscular dystrophy paints the top of his wheelchair
table. Although he cannot lift his arm without help, a simple ‘arm
rocker’ made of foam plastic lets him move it in all directions. It also
allows him to feed himself.
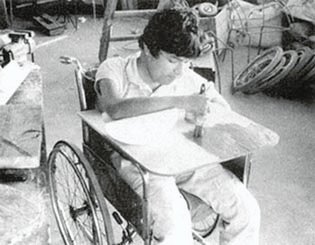
Figure
|
The goal of the family is to help the child be as active and
happy as possible, and to adjust to his increasing limitations. |
Helping the child to keep walking for as long as possible
Exercise. To keep as strong as possible and prevent
contractures, probably the best therapy, at least at first, is to stay active,
to walk, run, and play. While range-of-motion and stretching exercises may help
(see Chapter 42), it is even better to involve the child in games, work, and
other activities that keep his joints flexible. Even though he is slow and
awkward, encourage him to take part. Feeling sorry for him and just letting him
sit is the worst thing you can do.
Walking uphill and hillside farm work help prevent tiptoe
contractures of the ankles.

Figure
Braces. Long-leg braces should not be used until
absolutely necessary, as they will let the child’s legs grow weaker faster.
Sometimes lightweight plastic ankle splints, worn day and night, will help delay
ankle contractures and keep him walking better. (See Chapter 58.)

Figure
If contractures of the knees and hips begin to develop,
try resting or sleeping with ‘sand bags’ to press down the legs and
help straighten them.
Figure
Figure
|
CAUTION: Balance your efforts to provide therapy
or surgery against the need of the child (and his family) to lead as full,
happy, and normal a life as possible. His weakness will increase and his life
will be short regardless of all efforts. The goal of all care for the child with
muscular dystrophy should be to help him get the most out of living
NOW. The temporary benefits of surgery should be weighed
against the pain and hardships it would involve. |
Other aids. The child will reach a point where he needs
to use crutches. Later, (often by age 10) he will not be able to walk. Do
not force him when it becomes too hard. Instead, try to obtain or make a
wheelchair. (See Chapters 64 to 66.) At first, the child may be able to roll
it himself. But as his weakness progresses, he may need to be pushed.
Figure
A wide cloth or canvas strap across his belly and chest may
allow the child to play, to lean forward, and to use his arms more freely.
Breathing deeply is important, especially when the
muscles that move the lungs begin to weaken. Encourage the child to sing loudly,
to shout, to blow whistles, and to blow up balloons.
Shouting and climbing are both good exercises for the lungs.

Figure
Other problems
· Getting fat is a common
problem in children with dystrophy. The child needs to eat a healthy balanced
diet. But take care not to let him eat too much - especially sweet things. Extra
body weight will make walking, breathing, and other activities more difficult
for his weakening body, and will make it harder for family members to lift him.
· Constipation (hard,
difficult stools) may become a problem. Drinking lots of liquid helps. So
does eating fruits and vegetables, and foods with lots of fiber.
· Spinal curve can become
severe (see picture of Tito drawing, below). A corset or body brace may help
hold the child in a straighter position so he can use his arms better and
breathe better.
· Arm weakness in time
may become a problem for self-care and eating.
You can make a simple aid to help get the hand to the mouth.
Figure
|
CAUTION: If elbow contractures develop, it is
probably better to leave them, as a bent elbow is more useful than a stiff,
straight one. |
It is important to help the child gain interests and skills that
he can continue to develop even as he becomes very weak. He should stay in
school, if possible, even when he has to go in a wheelchair.
Learning to draw and paint can be fulfilling. In Los Pargos, an
organization of families of disabled children in Mexico, 4 brothers with
muscular dystrophy have all become very good artists. Their paintings have won
prizes in contests and are sold to raise money for the group. The best artist of
all was the oldest brother, Tito. He took pride in his paintings and enjoyed
teaching the other children. He did one of his best paintings, a sea turtle with
wings, a week before he died, at age 17.
Even when he was so weak he could barely move, Tito continued to
create beautiful pictures.

Figure
PREVENTION: The only way to prevent muscular dystrophy is
for women who may have the dystrophy gene not to have children. This mostly
means sisters of affected boys and close relatives on the mother’s side. If
you have one son with dystrophy, other sons will be likely to have it too. You
might consider not having more children.
OTHER MUSCULAR DYSTROPHIES AND MUSCULAR ATROPHIES
The type of dystrophy just described - also called progressive,
pseudohypertrophic, or Duchenne’s muscular dystrophy - is the most common.
But there are many different types of muscular dystrophy and muscular atrophy.
All start little by little: some in early childhood, some between ages 13 to 19,
and some in adults. All steadily get worse and worse. Some types, however,
almost stop after a certain age, and the person may live to active old age,
although
handicapped.
Chapter 11: Club Feet, Flat Feet, Bow Legs, and Knock-Knees
WHAT IS A DEFORMITY AND WHAT IS NORMAL?
Sometimes parents worry because they think a part of their
child’s body is abnormal or deformed. But in small children, often what
seems unusual is within what is normal, and will get better as the child
grows. For this reason, it is important to know what variations are normal and
which may be problems.
|
Note: For children born with parts of their bodies
missing or shortened, see Chapter 12 on birth defects. |
1. Many children are born with their feet somewhat bent or
crooked. To learn the difference between a normal bend caused by the
baby’s position in the womb, and true club feet.
CURVED FEET: NORMAL in the first weeks or months of life
Figure
‘FLAT’ FEET: NORMAL until age 2

Figure
2. ‘Fat’ or ‘flat’? - When most babies begin
to walk, they walk on the insides of their feet, with their legs wide apart.
Also their feet still have baby fat on the bottom. As a result, the feet look
very flat. In nearly all cases, they will get better by themselves.
3. A baby’s legs often bend outward (‘bow legs’),
like this. (1) This bending starts to disappear at the age of 18 months. Then
the legs slowly straighten until they actually bend inward a little, like this.
(2)
BOW LEGS: NORMAL until about 18 months
Figure
KNOCK-KNEES: NORMAL between 2 and 12 years

Figure
4. This ‘knock-kneed’ position generally develops
around age 2. By age 5 or 6 the knees begin to straighten.
|
Note: Children with brain damage sometimes develop
a ‘knock-knee’ way of standing or walking. If the child with
knock-knees also moves or walks in a stiff or jerky way, or shows other
problems, check for signs of brain damage. (See Chapter 9 on cerebral palsy.)
|
|
IMPORTANT: In any child who develops bow legs or
knock-knees, check for signs of rickets and other problems. See Chapter 13.
|
SEVERE KNOCK-KNEES
To check for severe knock-knees, have the child stand with her
knees touching. If the distance between the ankle bones is more than 3
inches in a 3 year old, or 4 inches in a 4 year old, the problem is
probably severe enough to need attention.

Sign of a problem
If the knock-knees are severe, braces may help straighten the
knees and keep the condition from getting worse. In a child over 6 or 7 years
old, braces usually do not help. In extreme cases, surgery may be needed.
Knock-knees may also lead to flat feet.
CLUB FEET

club foot before correction
About 3 out of 1,000 children are born with a club foot (or
feet). Sometimes it runs in the family, but usually the cause is unknown.
Sometimes a newborn baby’s feet turn inward, just because
they were in that position in the mother’s womb.
If the front part of a baby’s foot is turned inward, it
will often straighten out by itself before she is 2 years old.

Figure

Figure
To find out whether the condition is likely to correct itself,
or if it is a true deformity (club foot) that needs special attention, try to
put the foot in a normal position.

Bent foot straightens: NORMAL
If you can easily straighten the foot, and bend it into a
position opposite to the way it was turned, the foot probably does not have a
bone deformity and will get better by itself. Also, if you scratch the foot
lightly, the child often will move it into a normal position.

Bent foot does not straighten:
CLUB FOOT
If you cannot put the foot in a normal position, it will need to
be straightened with strapping or casts (see Chapter 60).
Are club feet a sign of some other problem? Although club
foot often occurs without any other problem, occasionally it is a complication
of spina bifida (problem in the spinal cord, see Chapter
22). Always check the child’s spine and test if he has feeling in his feet.
The feet may also gradually become deformed into a ‘club
foot’ position, because of cerebral palsy, polio, arthritis, or spinal cord
damage.
Rarely, club feet occur together with a ‘clubbed hand’
or other weakness and deformities of the body. See Arthrogryposis.
Correcting club feet (For details, see Chapter 60.)

Figure
A club foot (1) should be held in a cast (2), or strapped in a
straighter position, soon after birth - until it is corrected past normal.
After correcting the foot, daily stretching exercises are often
needed to help keep the foot straight.
Figure
A brace is used (day and night if necessary) to keep the foot
from bending in again,
Figure
until finally, normal use and exercise keeps the foot straight,
Figure

club foot after correction with
casts, by village workers (PROJIMO)
About 60% of club feet can be effectively straightened without
surgery in 6 to 8 weeks, using either strapping or casts. These
methods are described in Chapter 60.
Correction of club feet should begin soon after the child is
born - if possible, in the first 2 days. At birth, a baby’s bones and
joints are still soft. As the child gets older, his bones get harder and become
less flexible.
Usually, good correction without surgery is only possible in the
first year of life. If the deformity is not severe, however, a club foot can
sometimes be corrected with casts, even if the child is already 2, 3, or even 5
years old or more. But in an older child, it takes longer, and surgery is more
often needed for good, lasting results.
Some children with very deformed feet will need surgery, even if
strapping or casting is done early. However, we have found that some children
for whom surgeons have recommended surgery can have their feet straightened
with casts at a village center.
Keeping the feet straight once they are corrected
Once a club foot has been straightened, great care must be
taken to keep it straight. The whole family must make sure that the
following precautions are taken:
· An ankle brace should be worn
night and day at least until the child is walking, and often until
the child is 15 or 18 years old.
· Foot-stretching exercises will
be needed, especially if there is any sign that the foot is clubbing again.
Gently and steadily stretch the foot past its normal position in the
opposite direction of the deformity. Do this exercise 2 or more times a day.

Figure
· Check the foot regularly.
Return quickly to the rehabilitation center for an
evaluation if there is any sign that the clubbing is coming back.
How long will it take?
How difficult it is to straighten a club foot, how long it
takes, and how long braces and special exercises will be needed depends on a
number of factors:
· The severity of
clubbing. A severely deformed foot with abnormal bones is much harder to
correct.
· Abnormal muscle
balance, if present, will keep pulling the foot to the inside, even after it
is corrected. (See muscle testing)
· Generally, correction is more
difficult if both feet are clubbed.
· Club feet in girls
(although less common) are likely to be more difficult to correct than in boys.
· If there are any other
abnormalities (such as a clubbed hand or stiffness in the knees or elbows),
club feet may be especially difficult to correct. Usually surgery is needed.
· The older the child,
the harder it is to correct a club foot. Past the age of 2 years, it is often
not possible without surgery.
· Children without feeling in
their feet (spina bifida) require special precautions and slower correction
to avoid pressure sores. Casts, if used, must not apply much pressure, and must
be changed often.
If a child’s foot shows little or no improvement after 4
weeks of casting, or if improvement stops in spite of continued casting, surgery
is probably needed for more complete correction.
BRACES FOR USE AFTER CORRECTING CLUB FEET
For some feet, a plastic ankle brace (1) may work well.

Figure
For more difficult feet, a metal brace may be needed, with an
ankle strap that pulls the ankle inward (2).
A slight build-up on the outer edge of the sandal or shoe may
also help (3).

Figure
For instructions on making braces, see Chapter 58.
For babies under one year, or small children at night, feet can
be held in a good position using a bar that joins the feet (4).

Figure
For the child whose feet bend mostly at the middle or front

Figure
wearing shoes in reverse may help keep the feet
corrected.
Figure
FLAT FEET
Most children whose only problem is flat feet really have no
problem at all - except that poorly informed doctors or greedy special-shoe
salesmen make their parents think so!
Most babies have naturally fat feet, which
can look flat.

Normal foot of a child under 2
years old
Do not confuse a FAT foot with a FLAT foot!
In older children and adults there is a lot of natural variation
in people’s arches.

Figure
Even a foot as flat as this (1), if it causes the child no pain,
need not be considered a problem. Often flat feet run in families. If parents or
relatives have similar feet but no pain, or if the child can move his feet
strongly in all directions, do not worry about it.
|
Do not worry about flat feet if there is no pain, obvious
weakness, or loss of movement. |
Children who are late beginning to walk often have weak arches
with flat feet, until their feet get stronger.
Even children with very flat feet seldom develop a problem or
have more than average pain or discomfort when they do a lot of standing or
walking. Usually flat feet are a problem only when paralysis or brain damage
is the cause - as in some children with polio, cerebral palsy, or spina
bifida. Also, children with Down syndrome sometimes have flat feet that
may lead to pain or discomfort.
Correcting flat feet

Figure
The best treatment to help the child with flat feet and no other
problem may be to go barefoot. Walking barefoot on sand or rough ground
helps the feet get stronger and form a natural arch. Walking on tiptoe, skipping
rope, and picking things up with the toes may also help.
|
BEWARE of going barefoot where hookworm is common.

Figure
|
CAUTION: Special exercises, training in
‘foot posture’, shoe adaptations, heel wedges and shoe inserts (heel
cups and insoles) are often prescribed to correct flat feet. However, studies
show that usually none of these help. Use of insoles to support the
arches may even cause weaker arches. Usually insoles should be tried only when
pain is a problem, or in some severe flat feet caused by polio, cerebral palsy,
or Down syndrome.
|
WARNING: THIS METHOD USUALLY DOES NOT WORK
Some specialists try to straighten a foot that is tilted like
this

Figure
by putting a wedge under the heel of the shoe like this (1).

Figure
But instead of straightening the foot, this often causes further
deformity, because the heel slides to the side (2), and the shoe stretches here
(3) and wears out here (4).
Figure
|
INSOLES AND OTHER FOOT SUPPORTS
Some children with flat feet resulting from polio, cerebral
palsy, or Down syndrome may be helped by insoles or other foot supports. But
other children will not be helped. Each child’s needs should be carefully
considered. If after trying an insole for 2 weeks, the child walks with more
difficulty, change the insole or stop using it.
An insole is a firm pad that is put inside a shoe or sandal to
support the arch.

Figure
Insoles can be made of leather, porous rubber, or a piece of a
car tire, shaping it with care so that it will support the foot comfortably.
Before making the final insole, put a piece of cardboard,
wood or some other material shaped like the insole, under the child’s foot.
Try different heights to find what seems to work best. Make sure the heel is
in a straight line with the leg.
After making the insole, check the position of the foot.
Do this with the child standing on just the insole, and then with the insole
inside the shoe. Watch him walk, and ask him how it feels. If everything seems
right, check it again in 2 weeks.

CORRECT-The heel is in a straight
line with the leg.
TOO LOW-The heel tilts outward.
The insole should be thicker.

TOO HIGH-The heel tilts inward.
The insole is probably too thick.
|
CAUTION: A person who has a weak ankle and
low arch sometimes cannot use an insole, because it lets his ankle turn outward
as he walks. He may have learned to walk in a way that keeps his ankle from
turning out. For such a person, an insole may make walking more difficult, or
may force him to use a brace to keep his foot straight. |
|
IMPORTANT: The thickest part of an insole
should be directly under the ankle bone, just in front of the heel, like this
(1).

CORRECT
It should not be in the middle of the arch, like
this. This can deform the foot more without correcting the problem (2).
WARNING: Many commercial insoles, and even
orthopedic shoes, have the arches in this incorrect position (3). Check them
carefully. If they are like this, do not use them. Also be sure shoes are not so
wide that the heel slips to the side.

WRONG
|
If the child’s foot is flat or very floppy due to
paralysis, often an insole is not enough. He may need a short plastic brace that
supports the foot like this (4),

Figure
or a brace that supports the foot and ankle, like this (5).

Figure
For instructions on making plastic braces, see Chapter
58.
There is probably only one shoe or sandal alteration that does
any good. A small metal plate on the inner edge of the heel (6) stops uneven
wear - and may help prevent foot pain.

Figure
Chapter 12: Common Birth Defects
TYPES OF BIRTH DEFECTS
One out of every 100 or so babies is born with some kind of
obvious defect or deformity. There are many different types. In this chapter we
describe a few of the most common: cleft lip and cleft palate, extra
or joined fingers or toes, and short, missing, or deformed limbs. We
also discuss children born with multiple contractures
(arthrogryposis). Please also refer to the chapters on club
feet (Chapter 11), and spina bifida (Chapter 22).
CAUSES
In many cases, the cause of a birth defect is not known. But
sometimes a defect may be caused by one of the following:
· Poor nutrition during early
pregnancy. This is thought to be one cause of cleft lip and palate.

The mother of this girl with
cleft lip and palate did not get enough to eat while she was pregnant.
· Genetic (hereditary).
Sometimes certain defects run in families. For example, if one parent was born
with an extra thumb, there is a greater chance that a child will be born with a
similar defect. One or both parents may be ‘carriers’ of the factor
that causes a defect, without having it themselves. However, it may be present
in relatives. Often both parents must have a ‘defect factor’ for a
child to be born with the defect. For this reason, birth defects are more
common in children whose parents are closely related, and who therefore
carry the same defect factors.
· Medicines, pesticides,
chemicals, and poisons. Especially during the first 3 months of development,
a baby in the womb can easily be harmed by chemicals and poisons. Many
medicines, drugs, and pesticides (plant, insect, and rat poisons) can cause
birth defects if a pregnant mother is exposed to them.
A doctor gave this boy’s
mother a medicine for ‘morning sickness’.
· German measles. If the
mother gets German measles during the first 3 months of pregnancy, it can cause
defects in the baby. These usually affect the senses (hearing and seeing), the
brain (cerebral palsy and retardation), or organs inside
the body (heart, liver). Sometimes the baby is born with ‘rubber
band-like’ grooves on the limbs and deformed or missing fingers or limbs.

Figure
· Children born to mothers 40
years of age or older are more likely to have Down syndrome and defects of
the hands, feet, or organs inside the body (heart, liver). In this age group,
about 1 mother in 50 will have a child born with Down syndrome or defects.

This boy’s mother was 45
years old when he was born.
CLEFT LIP AND CLEFT PALATE
A cleft lip (or ‘hare lip’) is an opening or gap in
the upper lip, often connecting to the nostril.
A ‘cleft palate’ is an opening in the roof of the
mouth connecting with the canal of the nose.

simple cleft lip

double cleft lip

cleft palate
Usually 1 in about 800 children is born with a cleft lip, cleft
palate, or both.
Babies with these conditions often have trouble sucking, and may
choke or gag on food that gets into their nose. Usually breast feeding is the
best way to feed these children.
Put the breast deep into the mouth so that the milk comes out on
the back of the baby’s tongue.

Figure
Occasionally the mother may need to get milk from her breasts by
squeezing them, and then feed the milk to her baby with a spoon.

Figure
To prevent choking, feed the baby while he is sitting up with
his head tilted forward a little.

Figure
Make every effort to have the defects corrected by surgery since
this can greatly improve the child’s looks, eating ability, and speech.
The best age for surgery is usually at 4 to 6 months for the lip and
about 18 months for the palate.
To prepare for surgery, parents should frequently
stretch the deformed lip, so that the 2 sides meet in the middle.
Figure
Even after the cleft lip and palate have been successfully
repaired, speech problems often occur’. The family should gently encourage
the child to speak as clearly as she can. Lip and tongue exercises may help. The
child who cannot get surgery may need to learn sign language, using her hands to
help people understand her.
JOINED FINGERS AND EXTRA OR DEFORMED FINGERS OR TOES
Some children are born with 2 or more fingers joined together.
This does not cause much difficulty in use of the hand. However, special surgery
can often separate the joined fingers.

Figure
When a child is born with a small extra finger or toe that has
no bone in it, you can tie a string tightly around it, like this. In a few days
the finger will dry out and fall off.

Figure
Larger extra fingers or toes, if they get in the way, can be
removed by a surgeon.

Figure
A child who is born with a toe that sticks out may need surgery
in order to wear shoes. The toe can sometimes be put straight. At other times it
may be simpler to remove it.

Figure
To get the best results, the surgery should be done by a
specially trained orthopedic or plastic surgeon.
INCOMPLETE OR MISSING ARMS OR LEGS
Sometimes medicines a mother takes early in pregnancy cause a
child to be born with missing or incomplete arms or legs, or both.
A child born without arms but with normal legs and feet can
often learn to use his feet almost as if they were hands: for eating, writing,
drawing, playing games, and doing many kinds of work.

Figure
It is important to encourage the child to use her feet, or
whatever part of her body possible, to do everything she can for herself.

Figure
The child who is born with incomplete arms and legs can be
helped a lot by artificial arms with hooks for grasping.
We do not give instructions for making these arms in this book,
as they are fairly complicated. However, try every possibility to get artificial
arms for the child. They can make a very big difference in her life. If
possible, the child should get her first limbs by age 3.
For ideas about aids and artificial limbs for children born with
missing or defective hands and feet, see Chapter 27, “Amputations,”
and Chapter 67, “Artificial Legs.”
This little girl was born with ‘rubber band-like’
constrictions in her hand and leg, and with parts of her fingers and foot
missing. The deformities happened because her mother had German measles when
pregnant.

Figure
Her foot looked like this.

Figure
Village rehabilitation workers made her a
plastic brace with a partial foot built into it, so she could wear a regular
shoe or sandal.
A firm foam-plastic foot was shaped and attached to a plaster
mold of the foot (see Chapter 58). The plastic brace was heat molded over this.
Figure
ARTHROGRYPOSIS (Multiple contractures from birth)
Arthrogryposis means ‘curved joints’. Children with
this disability are born with stiff joints and weak
muscles. The strange position of arms and/or legs may give a child
the look of a wooden puppet.

Figure
In some children, both arms and legs may be severely affected.
In others, only the legs or feet, or hands or arms may be affected.
A child born with clubbed feet and with one or both arms stiff
with hands turned out, may have arthrogryposis.
TYPICAL BABY WITH ARTHROGRYPOSIS

Figure
|
The cause of arthrogryposis is not known. It may be a
virus infection of the mother, during pregnancy. Arthrogryposis is
a rare condition in most of the world, but for unknown reasons, in parts
of Central and South America it occurs more frequently. (In PROJIMO, in Mexico,
1 of every 100 disabled children seen has arthrogryposis.) |
Rehabilitation of the child with arthrogryposis
aims at helping the child do as much for herself as possible.
Some children with arthrogryposis are able to walk, especially
if contractures are corrected. Correction of club feet and hip and knee
contractures should begin gradually, and without forcing, soon after birth, with
casting, positioning, and/or range-of-motion exercises.
TYPICAL STANDING POSITION OF A CHILD WITH ARTHROGRYPOSIS
If both hips are dislocated, surgery to put the bones back into
their sockets is not usually helpful. The child walks as well without surgery.
If only one hip is dislocated, surgery may help.

Figure
Often, however, contractures of arthrogryposis can only be
corrected by surgery. The possible benefits - and losses - which surgery may
bring should be carefully evaluated. For example, a stiff elbow in a bent
(contracted) position may be much better for eating than an elbow that has been
straightened, and will not bend.
|
WARNING: A STIFF ELBOW IS OFTEN MORE USEFUL LEFT
BENT |

Figure
Most children with arthrogryposis are very intelligent. If given
a chance, many can learn to do a lot of things for themselves, even with
severe disability. Often they try hard and are eager to
learn. It is very important that these children be encouraged and helped to
do as much as they can for themselves, and that they go to school. The
following story may help give you an idea of the possibilities of a child with
arthrogryposis.
|
SIMPLE STEPS TOWARD INDEPENDENCE-A true story
Gabriel is 7 years old. He lives with his family in Mazatl�n,
Mexico. He was born with arthrogryposis. Some of his joints are stiff and
straight, others are stiff and bent. He lacks most of the muscles in his arms,
legs, and hands. He cannot sit alone or lift a hand to his mouth.
Figure
Gabriel’s parents love him dearly and care for him
tenderly. However, when he was born, doctors told them that nothing could be
done for him. So his parents grew used to doing everything for him. As he grew
older, they carried him in their arms, changed his diapers when he
dirtied them, and gave him food in his mouth. They treated him like a baby -
though he no longer was one.
When his mother learned of PROJIMO, she took Gabriel there,
hoping that with surgery or special medicine, he might improve. The village
rehabilitation workers at PROJIMO investigated all possibilities.
They even took him to a famous hospital for disabled children. But the
specialists said they could do nothing for Gabriel.
Fortunately, therapists who were visiting PROJIMO as instructors
explained to the team that in fact there was a lot that could be done, not to
help Gabriel walk, but to help him do more for himself - within his
possibilities. The team began to work with the family, to help Gabriel become
more independent.
Now, with the help of the village rehabilitation workers and his
family, Gabriel is able to meet some of his basic needs for himself. He feels
less like a baby and more like a young man. He has stopped using diapers; he
asks when he needs to go to the toilet. He has learned to use his mouth like a
hand, to hold and do things.
He has learned to feed himself. He swings his arm onto the table
using his neck muscles, and hooks his hand over a spoon. Using the edge of the
table and the rim of the dish to push against, he see-saws the spoon to his
mouth. To drink he uses a straw with a bend in it.
Figure
Gabriel’s family has joined Los Pargos, an organized group
of families of disabled children. He attends school in a specially-adapted
wheelchair that he can move himself. He is learning to read, write, paint
pictures, and to play with other children.
There is much more that Gabriel and his family will be able to
achieve, now that they all see how much he can do for himself. Gabriel is happy
and eager to learn more.

Gabriel wrestling with another
disabled child.
|
Various aids and adaptations can help children
with arthrogryposis or similar disabilities become more independent:
Eating aids are described in Chapter 36.

Figure
Writing aids are shown in Chapter 1, Chapter 27 and Chapter 53.

Figure
Wheelchair aids are shown in Chapter 64.

Figure
PREVENTION OF BIRTH DEFECTS
It is not possible to prevent all birth defects. There are,
however, ways to make it less likely that children will be born with birth
defects.
· Eat well during
pregnancy. (See Where There Is No Doctor, Chapter 11.)
· Avoid marrying close
relatives. If you already have one or more children with a birth defect,
consider not having more.
· Avoid all medicines during
pregnancy unless you are sure they will not damage the baby. (Aspirin,
vitamins, some antacids, and iron in the correct dose are all right.) Avoid any
contact with pesticides and other poisons. Tobacco and alcohol during pregnancy
can also damage the developing child.
· While pregnant, stay far away
from children with German measles if you have never had it. If you are not
pregnant, try to catch it before you get pregnant. Vaccine exists
for German measles, but is not often available.
· Consider not having more
children after age 35 or 40, or if you have had one child with Down syndrome,
since the chance of having another is increased.

A child with brittle bone disease.
(Photo by Philip
Kgosana)
Chapter 13: Children Who Stay Small or Have Weak Bones
In this chapter we look at children whose bones are weak and
deformed, and at children who do not grow as tall as other children’. We
include rickets, brittle bone disease, and children who stay very
short (dwarfism). In all of these conditions, the legs may become
bowed, and the shape or proportions of the bones are often not normal.
RICKETS

SIGNS OF RICKETS
Rickets is weakness and deformity of the bones that occurs from
lack of vitamin D. Vitamin D occurs in whole milk, butter, egg yolks, animal
fats, and liver, especially fish liver oil. The body also makes its own vitamin
D when sunlight shines on the skin. Children who do not eat enough foods with
vitamin D, and who do not get enough sunlight, gradually develop signs of
rickets.
Rickets is fairly common in some countries, especially in cool
mountain areas of Asia and Latin America where babies are kept inside and
wrapped up. Rickets is also increasing in crowded cities where children are
seldom taken into the sunlight.
Treatment for rickets is to give fish liver oil, and to
spend time in the sunlight. The best and cheapest form of prevention is
to be sure sunlight reaches the child’s skin. Foods that contain vitamin D
also help.
BRITTLE BONE DISEASE

SIGNS OF BRITTLE BONE DISEASE
The child is born with bent or twisted limbs, or with broken
bones. (Or he may seem normal at birth, and the bones begin to break later.) He
may start to walk at near the normal age, but increasing deformities due to
breaks may soon make walking impossible. Because of the many broken and bent
bones, these children stay very short. Parents sometimes do not realize when
their child breaks a bone.
Brittle bone disease is not common. Sometimes it is
inherited, and someone else in the family will have the same problem.
There is no medical treatment. However, sometimes surgery can be
done to straighten and strengthen the leg bones by putting a metal rod down the
middle of them. This may help the child walk for longer, but he may eventually
need a wheelchair to move about. Back problems increase with age; a body brace
may help.
Children with brittle bone disease are often intelligent and do
well in school. Increasing deafness may become a problem. Help them to develop
their minds and learn skills that do not require physical strength. The child
must learn how to protect his body from breaks. It helps to sleep on a firm bed.
CHILDREN WHO STAY SHORT (Dwarfism)
Parents often worry when a child does not grow as quickly as
other children. Shortness has many causes. Here we discuss only a few.
· Normal slow
growth. Some children normally grow more slowly and mature sexually later
than others. If the child is normal and healthy in other ways, do not worry. He
will probably grow quickly when he begins to grow up sexually, even if this
happens as late as 15, 16, or 17 years old.
· Normal short size. When
one or both parents are shorter than average, they may have children who are
also short. Shortness ‘runs in the family’ and this is normal. Make
sure the child is healthy and eats well.
· Poor nutrition. Some
children do not grow normally because they do not get enough to eat, or do not
eat the food their bodies need. They may seem normal except that they are thin,
small, have big bellies, and get sick often. Or they may lack energy, seem very
unhappy, or develop swollen feet, hands, and faces. These children need more and
better food. They may also need more stimulation, play, love, and attention in
order to grow and develop more quickly (see Chapter 35).
· Long-term illness or
medication. Severe long illness often slows down a child’s growth.
Also, certain medicines such as cortisone or steroids for arthritis, if given
for a long time, can slow down growth and weaken bones.
· Dwarfism. Some children
are born with a condition in which the body does not grow normally. There are
many different patterns and causes. In 1 of 5 children it is inherited, and
certain relatives will also be very short.
NORMAL

THREE TYPES OF DWARFISM
In the most common type of dwarfism (1), the arms and
legs are short for the body. The head is big, the forehead bulges, and the
bridge of the nose is flat. The child often has a swayback, pot belly, and
bowlegs. Hip problems, club feet, or eye problems and hearing loss may occur.
TREATMENT
There is no medical treatment for most children who are short,
including those with dwarfism. In many countries, doctors prescribe
‘growth’ hormones to short children to make them grow faster. These
may cause some growth at first, but they soon make the bones mature and stop
growing, so that the child stays smaller than he would have without
treatment. Do not give hormones to speed growth.
Children who are very short for their age sometimes are made fun
of by other children, or get treated as though they are younger than they really
are. Life can be difficult for them and they may feel unhappy or unsure of
themselves. It is important that everyone treat them just like other children
their age. CHILD-to-child activities can help other children become more
understanding (see Chapter
47).
Chapter 14: Erb’s Palsy: Arm Paralysis from Birth Injury
WHAT IS IT?
Erb’s palsy is a paralysis of the
muscles in a baby’s arm, caused by injury of the
nerves in the shoulder at birth (during delivery).

Figure
The baby lies with one arm and hand twisted backward and does
not move the arm as much as the other.
If the full range of motion of the arm is not kept through
regular exercise, contractures will develop that may prevent
lifting the arm above the shoulder or turning the hand palm up.
HOW COMMON IS IT?
Nerve damage causing Erb’s palsy occurs in approximately 1
out of every 400 births. It is much more common in babies who are born butt
first (breech) because the shoulder is easily stretched and the nerves injured.
Severe Erb’s palsy in 14
year old boy. This is as high as he can lift his arm.
WHAT CAN BE DONE ABOUT IT?
With the baby, start range-of-motion exercises 2 times a day.
Extend the child’s arm and turn the hand upwards.
Figure
Then raise the arm straight over the child’s head.

Figure
When the child is old enough, have him do exercises himself, for
range of motion and to increase strength.
Ask him to lift his arm as high as he can, turning the palm up
as far as he can,
Figure
and then lift it with the other hand as high as he can, with the
palm up.
Figure
Note: If contractures have already formed, do
exercises more often, for a longer time. Each time try to turn the hand up and
lift the arm as high as possible. Hold it in the stretched position while you
count to 25, or sing a song.
Other helpful exercises

Figure

Figure
Figure

Figure
Figure
Look for ways to include these exercises in work and play.

Figure
PREVENTION
Erb’s palsy can sometimes be prevented if the midwife or
doctor takes care not to strain or force the baby’s shoulder when being
born. Examination of the mother’s belly before birth should let the midwife
know if the baby is likely to be born breech. In this case a hospital delivery
by a skilled doctor or midwife may reduce the chance of injury.
Contractures and significant disability from
Erb’s palsy can largely be prevented by exercises. Some weakness may last
throughout
life.
Chapter 15: Painful Joints

Figure
Joint pain in children has many causes. Depending on the cause,
different treatments may be needed. The chart that follows will help you decide
what the cause of chronic (long-lasting) joint pain in a child might be.
However, other less common causes may also be possible. Sometimes laboratory
tests may be needed to be more certain.
Specific treatment is needed for certain kinds of joint pain -
especially those caused by infection. However, some basic
principles of care and therapy apply to most joint pain,
regardless of the cause. Following the chart of causes, you will find some
general guidelines for the care of joint pain. These guidelines are described in
more detail in Chapter 16 on juvenile arthritis.
Three chapters on disabilities with joint pain are
“Juvenile Arthritis” (Chapter 16), “Rheumatic Fever”
(Chapter 17), and “Hip Problems” (Chapter 18). However, arthritis
(joint pain and damage) can occur with any disability where
paralysis or muscle imbalance cause abnormal positions or twisting
of joints. Many children with polio develop painful dislocations
or, when they are older, arthritis.
NOTE: The chart does not include the many
infectious diseases that may cause temporary joint
pain. These do not usually lead to long-term disabilities. For details of
diagnosis and treatment of illnesses that cause temporary joint pain, consult a
health worker or see a medical text such as Where There Is No
Doctor.
|
CAUTION: Try not to confuse similar illnesses. Two
of the most common causes of joint pain in children are rheumatic fever
and juvenile arthritis. Even some doctors and health workers get them
mixed up and diagnose juvenile arthritis as rheumatic fever. The two illnesses
do have similarities. However, rheumatic fever almost always follows a period of
sore throat with fever. If the child did not have a sore throat, probably the
joint pain is not due to rheumatic fever. When in doubt, however, 10 days of
penicillin pills may be a wise precaution. |
Carefully study the differences between the common causes of
joint pain. If you are not sure, seek help from someone with more experience.
COMMON CAUSES OF CHRONIC JOINT PAIN IN CHILDREN (pain that
lasts more than 2 weeks or keeps coming back)
|
Problem |
Age it often begins |
Pain in one or in several joints |
Fever |
Other signs |
Treatment and therapy |
|
rheumatic fever (See Chapter 17.) |
5 to 15 years old |
Usually pain is in several joints. (Rarely it begins with
severe pain and swelling in only one joint, but often there is also some pain in
other joints.) Often pain starts in ankles and wrists, then knees and elbows.
Pain may change from some joints to others.

Figure
|
High fever is typical (usually starts suddenly).

Figure
|
· Joint pain and fever usually
begin 1-3 weeks after severe sore throat with fever (strep throat).
· Small lumps may appear under
the skin over joints.
· sometimes wiggly reddish
circles on skin
· in severe or advanced cases,
heart problems (‘heart murmur’, difficulty breathing, or chest pain)
· usually gets better in 6 weeks
to 3 months - but likely to come back |
· penicillin for 10 days each
time throat gets sore (or continuously if heart is affected)
· aspirin in high doses with
precautions
· rest
· range-of-motion (ROM)
exercises
· Apply heat or cold to painful
joints. |
|
juvenile arthritis (also called juvenile rheumatoid
arthritis or Still’s disease) (See Chapter 16.) |
Any age, but often begins between 2-7 or 9-12 years old
Lasts for years (Often the arthritis gets better when child
becomes sexually developed) |
May affect few joints, many joints, or almost
all joints.

Figure
(In 1/3 of children it begins in only one joint - later
it may affect others.) |
Often some fever when pain is worst. (Rarely, it begins with
high fever.)

Figure
|
· usually no history of sore
throat
· severely painful, hot, swollen
joints often leading to muscle weakness, contractures and deformities
· sometimes a rash that comes
and goes
· may begin little by little, or
suddenly and severely
· one or both eyes may become
red and sore (iritis) and become damaged

Figure
· usually lasts for years with
periods when it gets better and then worse |
· aspirin in high doses with
precautions to avoid stomach upset
· Apply heat or cold to painful
joints.
· ROM exercises
· exercises without motion to
strengthen muscles
· lots of rest, but also
moderate activity
· lots of understanding and
support |
|
destruction or slipping of cap of thigh bone at the hip
(See Chapter 18.) |
Destruction: mostly boys 4-8 years old
Slip: mostly boys 11-16 years old |
pain in one hip (rarely both)
Destruction:
(1) Cap of head of thigh bone breaks into pieces and gradually
re-forms in 2 to 3 years

Figure
X-ray needed to make definite diagnosis |
no fever |
· child begins to limp - often
without complaining of pain
· may complain of pain in knee
or thigh (or sometimes hip); gradually develops weakness for raising leg like
this

Figure
|
· For destruction: it may be
best to do nothing, although many specialists still recommend casting, braces or
surgery.
· For slip: surgery to pin the
cap into the right place may be needed.

Figure
|
|
below-knee pain
(Osgood-Slater’s problem) |
Boys 11-18 years old |
usually one knee only

Figure
|
no fever |
· especially in very active,
strong boys
· may begin with pain after
jumping, running, or forceful exercise |
· Avoid forceful exercises or
activities until pain goes away (usually in 2 to 3 years).
· aspirin and hot (or cold)
soaks for pain
· The problem may last for years
but in time will go away, although the bony bump remains. |
|
‘hot’ infection of a joint (bacterial
infection: staphylococcus, streptococcus, typhoid, etc.) |
any age, but rarely in very young children |
one hip, knee or ankle joint
rarely more than one joint |
often low fever, sometimes high fever, at least at first |
· sometimes follows injury to
joint or illness such as typhoid
· usually begins suddenly
· joint often red, hot, swollen

Figure
· joint destruction may be
severe-leading in time to a fused or ‘frozen’ joint, or dislocation
|
· Identify cause of infection
(tab tests needed).
· Treat with appropriate
antibiotic.
· Apply splint to avoid motion
and activity during early stage. |
|
‘cold’ or ‘slow’ infection of a joint
tuberculosis (TB), (or less commonly, syphilis, gonorrhea, or fungus - which are
not discussed here) |
any age, but mostly in older children and young adults |
one hip or knee, or in backbone (See TB of spine)
Figure

Figure
often much pain (sometimes no pain until the bone or joint
damage is severe) |
no fever |
· often history of TB in family
· Only half of these children
have signs of lung TB.
· strongly positive TB skin test
(test has meaning only in children not vaccinated against TB)
· child often quite thin or
sickly (but not always)
· Pain usually begins little by
little and may become so bad that the child cannot move his leg. |
· anti-tuberculosis medicines (2
or 3) for at least 1 year (See Where There Is No Doctor, p. 180.)
· daily ROM exercises
· aspirin and hot soaks for pain
·
‘exercises-without-motion’ to keep muscle strength |
|
sprains and torn ligaments |
older child or adult |
one joint only

Figure
hot and swollen at first |
no fever |
· Ankles and knees are common
sites.
· often results from forceful
twisting
· Joint may be loose or floppy,
and remain weak for months or years. It may easily be twisted or injured again.
|
· Apply cold during first day
after sprain; following days, apply heat.
· Avoid motion but keep joint in
good position.
· aspirin for pain
· Provide temporary support with
elastic or-adhesive bandage or (in severe cases) a cast or ankle brace. |
|
injury to joint surface (for example: torn meniscus,
bursitis) |
older child or adult |
usually one joint only, often the knee |
no fever |
· usually after twist or strain
or injury
· may hurt suddenly or go weak
at certain times but not at others
· Swelling or ‘liquid’
under skin may form behind knee or on the edge of joint.
Figure
|
· Provide support with elastic
bandage.
· rest, moderate activity
· gentle ROM exercises
· aspirin for pain
· If problem continues, seek
help of a specialist. |
|
dislocated joint due to injury
(dislocation is when a bone comes out of its socket) |
at birth or in older child |
one joint
Hips, shoulder, and elbows are most common. |
no fever |
· at first, very painful and
weak
· In weeks or months (if
uncorrected) pain becomes less but weakness often remains.

Figure
|
· Have an experienced person try
to put the bone back in its socket (the same day or soon after the dislocation
occurs). Older dislocations and some new ones may need surgery.
· Provide support for a few
weeks with elastic bandage (especially shoulders and knees).
· Gently do ROM exercises every
day. |
|
dislocated joint due to muscle weakness or muscle
imbalance |
occurs in older child with polio, other paralysis, or arthritis
|
usually one joint
Figure
pain mild to severe, often occurs with weight bearing and
increases with time |
no fever |
· deformed (strangely shaped)
joints
· Knees, shoulders, hips, feet,
elbows may gradually dislocate because muscles pulling them in one direction are
stronger, or because muscles surrounding the joint are so weak.
Figure
· Careless stretching exercises
may cause or increase dislocation. |
· Try to put dislocated joint
back into place.
· Avoid positions that force
joint out again.
· For partial dislocations of
knee, careful stretching exercises may help - but take care to avoid further
dislocation. |
How to care for painful joints
1. REST THE JOINTS
The more painful the joint, the more it needs rest. Some
movement is important, but no forceful exercise or heavy use of the joint.
If joints are swollen, it helps to keep them lifted up.
Figure
2. HEAT AND COLD
Applying heat (see side box) or cold to the joint often reduces
pain and makes motion easier. For cold, use packs of ice wrapped in a cloth or
towel for 10 or 15 minutes. Experiment to see which works better. Usually
cold works better on hot, inflamed joints and heat on sore, stiff
joints.
Hot wax can be used instead of hot water. Some specialists say
that it does not do more good than hot water, but persons with arthritis find it
very soothing.
Heat beeswax or paraffin until it just melts (but not too hot -
test it first on a finger).

Figure
Dip the hand or painful joints into the hot wax.

Figure
Take it out. The wax will quickly harden.
When it cools, dip it in again.

Figure
|
HOT SOAKS
1. Boil water. Let it cool until you can hold your hand in it
comfortably.
Figure
2. Wet a thick cloth or towel in hot water and squeeze out the
extra.

Figure
3. Wrap the cloth around the joint.

Figure
4. Cover the cloth with a piece of thin plastic.
Figure
5. Wrap with a dry towel to hold in the heat.

Figure
6. Keep the joint raised.
7. When the cloth starts to cool, put it back in the hot water
and repeat. |
3. PAINKILLERS
Usually aspirin works best, because it reduces both
pain and inflammation.

Figure
Note: For severe pain, splints to prevent
motion help reduce pain and prevent contractures.
4. RANGE-OF-MOTION (ROM) EXERCISES

Figure
It is important to move the joints through their full range of
motion at least twice a day (especially if splints are used). If it hurts, apply
heat or cold first, and move them very slowly. Do not force! (See Chapters 16
and 42.)
5. EXERCISES WITHOUT MOTION
Figure
These are exercises to strengthen muscles without bending the
painful joints. For example, a child with a painful knee can keep her thighs
strong by tightening her thigh muscles while her leg is - - straight. She should
hold the muscles tight until they get tired and begin to tremble. This will
strengthen them and keep them strong.
6. CONTINUE DAILY ACTIVITIES

Figure
With most joint pain, it is important that the child remain
fairly active. She should try to continue with all daily activities that do not
strain or overwork the painful joints. Moderate activity is usually recommended
(except for acute infections or injuries, when complete rest may be needed for
several days).
Designs for therapy baths
Floating and playing in water provide exercise and therapy for
many kinds of physical disabilities - especially those in which movement is
limited because of pain or muscle spasms.
For children who have the opportunity, bathing, swimming, and
playing in rivers and ponds with other children is good - but only when the
rivers or pools are not dangerous and do not transmit diseases.

Figure
This ‘therapy pool’ at PROJIMO has one large deep tank
for standing, swimming, and play. And it has 2 narrow ‘water lanes’ at
different depths for children to learn to walk while supported by water.
Disabled and non-disabled children play here together.
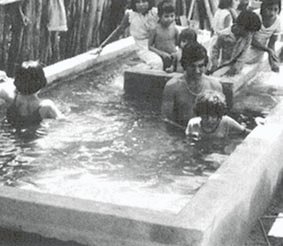
Figure
TUBS OR TANKS OF SUN-HEATED WATER (solar heating)
Bathing in warm water is especially helpful. The penetrating
heat of the water helps to improve blood flow, calm pain, and relax the muscles.

Figure
You can dig a hole in the ground and cover its sides with
plastic sheets or cement to prevent the water from leaking out. So that the
sunlight heats the water faster, use black plastic, or paint the cement a dark
color. (Green is friendlier than black.)

Figure
TUB WITH A SELF-CIRCULATING SUN HEATER

Figure
(1) Because warm water weighs less than cool water, the hot
sun-heated water will rise and run into the tank here.
(2) In order for the water to keep flowing, the hose heating
unit must be below the level of the tub.
(3) sheet of clear plastic over the hose
(4) black hose
(5) The cooler water will run out here.
|
INFORMATION ON ASPIRIN FOR SWOLLEN JOINTS IN PERSONS WITH
ARTHRITIS OR RHEUMATIC FEVER
Aspirin (acetylsalicylic acid) is usually the best medicine for
joint pain:
· Aspirin not only
helps to control pain, it reduces inflammation (swelling and
damage to joint surfaces). Thus it helps stop destruction of the joints. Many
other painkillers do not do this.
· Aspirin is not
expensive.
· When taken correctly, aspirin
has fewer risks, dangers, and complications than most other medicines for
joint pain.
In order for aspirin to work well without causing problems:
· Take the correct
dose at the right times every day.
· Keep taking the same amount of
aspirin even after the pain has lessened. This will still help control swelling
and let the joints begin to heal.
· Take strict precautions to
avoid stomach upset.
PRECAUTIONS
A. Aspirin is an acid. It can cause stomach-ache, chest pain
(so-called ‘heartburn’), or even make holes (ulcers) in the stomach.
To avoid these problems:
· Always take
aspirin with food or a large glass of water.
· If this does not prevent
stomach pain, take the aspirin not only with food and lots of water, but also
with a spoonful of an antacid such as Milk of Magnesia (magnesium sulfate),
Maalox, or Gelusil.
Stop taking aspirin if:
· stomach pain still
occurs after following the above precautions,
· you start to vomit blood,
· you start to shit blood, or if your shit looks like
black tar (digested blood).
B. Too much aspirin will poison the body. (The dose that
will reduce inflammation is almost as much as the dose that can poison.) An
early sign of poisoning is ringing in the ears. If the ears begin to ring,
stop taking aspirin until it stops. Then take it again, but in a slightly
lower dose.
C. Keep aspirin out of the reach of small children.
CAUTION: To prevent choking do not give medicine to a
child while she is lying on her back, or if her head is pressed back. Always
make sure her head is lifted forward.
DOSES OF ASPIRIN FOR ARTHRITIS AND RHEUMATIC FEVER
500 mg. tablets:
Adults: 2 to 3 tablets, 4-6 times a day
Children,
8-12 years: 1 tablet, 4-6 times a day
Children, 3-7 years: half a tablet, 4-6
times a day
Children, 1-2 years: one-quarter tablet, 4-6 times a
day

Figure
If there are no swollen joints, use another medicine just for
pain. This is very important if aspirin causes too many side effects. For other
medicines for pain, see the Green Pages in Where There Is No
Doctor.
The dosage given here is the anti-inflammatory dosage, which is
double the normal dosage for reducing pain and lowering fever.
The dosage is based on 100 mg. of aspirin for each kg. of a
person’s weight each day. For example, a child weighing 25 kilos would take
2500 mg. each day, or 1 tablet of 500 mg. 5 times a day (always together with
meals or lots of water).
CAUTION: Aspirin tablets for adults usually come in
325 mg. (5 grain) or 500 mg. (8 grain) tablets. Children’s aspirin usually
comes in 81 mg. (1¼ grain) tablets. Be sure to figure out the dose
correctly. Avoid aspirin combined with caffeine or with other painkillers.
The dose of aspirin for your child is:
________________________________________________ |
Chapter 16: Juvenile Arthritis
Chronic Arthritis in Children
HOW TO RECOGNIZE IT
· The arthritis (joint pain)
often begins between the ages of 5 and 10, but may begin in very young children
or teenagers.
· Usually it keeps getting worse
for several years.
· There are times when the pain
and other signs get better, and times when they get worse.
· It affects different children
in different ways. It can be mild or very disabling.
Signs

JOINTS THAT MAY BE AFFECTED
· Joint pain. Often
begins in the knees, ankles, and wrists. Later it affects the neck, fingers,
toes, elbows, and shoulders. Still later, the hips and back may be affected.
· Joints are especially painful
and stiff in the morning (morning stiffness).
· Fevers and rash that
come and go. (In some children these are the first signs.)
· The knees become large and may
turn inward.
· Pain may make it difficult to
straighten the knees, hips, and other joints. The cords may
tighten, forming contractures, and the bones may gradually
become dislocated.
· A child with severe
arthritis often sits with his arms and legs bent in the least painful position.
Without exercise and good positioning, contractures may form so that he cannot
walk or even stand up.

Figure
· Children with severe arthritis
in the neck and jaw may have a small, short chin.
Figure
· The fingers may become very
thin and deformed, or thick, with slender tips.

Figure
· Wrists and ankles may become
stiff and bent.
Figure
· Contractures may develop in
the fingers or toes, and with time the bones may fuse (stick together).
More information about JUVENILE ARTHRITIS
|
There are 3 types of juvenile arthritis:
1. Fever type: There are times during the day when the child has
a high fever, a rash, and feels ill and tired. He looks very sick. The joint
pain seems less important, and it begins days or months after the other signs.
There may be severe anemia (child looks pale).
2. Many-joints type: More than 5 joints with pain. The child
hurts a lot, and moves very little. Often severe contractures develop. The child
does not grow much, and his sexual development is delayed.
3. Few-joints type: Fewer than 5 joints affected. It can affect
more joints after months or years. If the back is affected, it is more likely
that severe arthritis will continue when he is adult. It may affect the eyes,
causing iritis and blindness.

iritis
|
What causes it?
The exact cause of juvenile arthritis is not known, but it has
something to do with the body’s ‘immune system’ (defenses against
disease). This begins to attack not only germs, but parts of the body itself.
The problem is usually not hereditary, and is not related to
climate, diet, or the child’s way of life. It is not caused by anything the
parents may have done. It cannot spread from one child to another. It does not
affect the child’s intelligence.
Will the child get worse, or better? What about her
future?
The progress of the disease varies a lot. Typically, there are
times when the joints become very painful, and times when they hurt less. Often
the joint pain and disability will get worse and worse for several
years, then gradually start to improve. Two out of 3 children will stop having
active arthritis after 10 years, although the damage already done to the joints
may cause some permanent disability. Some children will continue to have
arthritis when they are adults, but it is usually milder.
|
Most children with arthritis will become adults who walk,
work, and have full and happy lives. |
How does it affect the child and her family?
A child with severe arthritis suffers a lot. After a night of
being kept awake by the pain, the child may be irritable, sad, and dull. But
when the pain is less, she may be friendly and lively.
Since the arthritis often continues to get worse for years, even
with all efforts to cure it, both the child and her family may lose hope and
stop trying.
Also, the family may not understand how much the child is
suffering, because the cause of the pain does not show. (In children’s
arthritis the joints do not usually get red, as they do in adults.) So the
family sometimes calls the child a ‘cry-baby’ or a trouble-maker. The
child may feel abandoned or guilty. The situation is very hard on the whole
family.
The family needs the help and support of understanding
neighbors, health workers, and, if possible, a rehabilitation worker. They need
to understand that by continuing exercises, therapy, and
medicines - often for years - the child does have hopes of getting
better. If therapy takes the form of games with other children and family
members, it may help both her body and spirit.
SECONDARY PROBLEMS
When parts of the body do not get enough movement or exercises,
joint contractures are common. With time, the bones may become fused (joined
together) or dislocated. Also, the muscles that straighten the
arms and legs become very weak. However, with exercises and with enough movement
and good positioning, all these problems can be prevented or made less severe.
Managing juvenile arthritis
The child will need:
1. medicine to relieve the pain and help
prevent damage to the joints
2. plenty of rest, keeping the body in good
positions
3. exercises and movement to prevent contractures
and deformities, and to keep the muscles strong
4. mental, physical, and social activities, so that the
child’s life is full and satisfying
5. if necessary, aids, and braces or casts
to correct contractures and to help the child to move about
MEDICINES
Aspirin (acetylsalicylic acid) is usually the safest and
best medicine. It not only helps the pain, but also reduces inflammation and
damage in the joints. For precautions and doses, see the INFORMATION SHEET.

Figure
Medicines that generally should NOT be used:
Corticosteroids have a strong anti-inflammatory effect,
but they are dangerous. Although they quickly reduce the pain, joint destruction
continues. Steroids make the child’s body less able to fight infection,
stop his growth, and weaken his bones so that they break easily. If the
child takes a lot of steroids, his face becomes round and a hump of fat forms on
the back of his neck and shoulders. As a rule, steroids should be used only
when the child’s life or eyesight is in danger. Steroid eye-drops at
the first signs of iritis can prevent blindness.

‘moon face’ and hump of
fat on the back of the neck, caused by steroids
Gold salts. Gold combined with sodium and sulfur, in
injectable form, sometimes helps when aspirin is not effective. But it is very
toxic (poisonous) and its use should be limited.
Indomethacin (Indocin), phenylbutazone, and related
medicines are so toxic that they should not be given to children.
|

|
WARNING: We mention corticosteroids, indomethacin,
and phenylbutazone because many doctors prescribe them unnecessarily, putting
the health or life of the child in danger. If a doctor prescribes one of these
medicines for a child, get advice from other doctors before using it. |
REST AND POSITION
Children with arthritis need a lot of rest. They tire easily,
and should have a chance to rest often. Help the child to be in positions
that keep the arms, wrists, hips, and legs as straight as possible.
In these positions, contractures develop more easily.
Figure
Although it may hurt more, it is better for the child to lie on
her back or stomach, not on her side with her legs bent.
When pain is worst, alternate rest with legs straight and
slightly bent.
In these positions, contractures are less likely to develop.

Figure
Rest and sleep with the arms and legs as straight as possible.
Use pillows only in a way that gently helps the joints straighten more. Let the
legs slowly straighten under their own weight.
EXERCISES AND MOVEMENT
Our goal is to prevent contractures and dislocations, and to
maintain the fullest possible range of motion for the body. So exercises are
needed to strengthen the muscles that straighten the joints.
HOW PAIN CAUSES CONTRACTURES
|
When these muscles are tightened, they straighten the knee,
|
Because it hurts to straighten the knee, the child with
arthritis does not use these muscles much. So they become very weak. |
Since the muscles on top are weaker than those below, the uneven
muscle strength keeps bending the leg more and more, even during sleep. |
|

Figure
|

Figure
|

Figure
|
|
and these muscles bend it. |
But these muscles stay tightened to keep the knee bent and guard
against pain. So they stay stronger. |
NOTE: This kind of uneven muscle strength
is called muscle imbalance. |
Because contractures from arthritis result mainly from unequal
muscle strength, it is important that the child do all exercises and
activities in ways that will strengthen the weak muscles that straighten the
joints, not the muscles that bend them. For example:
|
Do exercises that work this muscle. |
But do not do exercises that work this muscle. |
|
This is the muscle that straightens the knee and prevents
contracture (1).

Figure
|
This is the muscle that bends the knee and causes a contracture
(2).
Figure
|
|
STRENGTHEN MUSCLES THAT STRAIGHTEN THE JOINT. |
DO NOT STRENGTHEN MUSCLES THAT BEND THE JOINT. |
Follow this same logic with all exercises and activities. And
look for ways to make the exercises useful and fun.
For example, Alicia has arthritis and can no longer walk by
herself or straighten her arms and legs completely. As a way of moving herself
about and getting some exercise, she can sit on a chair with
casters, as shown here. But she should be careful to move in a way
that helps prevent contractures.
|
Pulling herself forward with her arms and legs exercises mostly
the muscles that bend the joints. |
Pushing herself backward, with her arms and legs, does more to
strengthen the muscles that straighten the joints. |
|

Figure
|

Figure
|
|
This can make contractures worse. |
This helps prevent contractures. |
Helping the child to strengthen the right muscles
One problem with exercises is that, when either you or the child
try to straighten a joint, pain - or the fear of pain - can cause her to tighten
the muscles that bend it. For example:
|
If you pull like this, the muscles that bend the elbow will pull
against you-and get stronger. |
Even if the child herself tries to straighten her elbow, the
pain will cause the stronger, bending muscles to tighten. |
|
Figure
|

Figure
|
|
The muscles that straighten the elbow will not be used - and
will get weaker. |
As a result, these exercises may strengthen the bending muscles
instead of the weaker straightening muscles. This means that these exercises can
actually make contractures get worse! |
EXERCISES WITHOUT MOTION
So it is important that the child learn to do exercises that
strengthen the muscles that pull against contractures, not those that make them
worse. This will be easiest and least painful if she does exercises without
motion.
First help her to learn which muscles move parts of her body in
different directions.

Figure
Have her exercise these muscles by relaxing and tightening
them, without moving her arm.
Then help her find interesting ways to strengthen the muscles
that need it without moving them. For example, she can lean on a fence like
this.
Everyday she can step a little farther back from the fence (1),
to take more weight on her arms.

Figure
Notice that this exercise also strengthens her
knee-straightening muscles and helps stretch her heel cords, wrists, hips, back,
and neck, in order to look the llama in the eye.
|
Note: We have shown these exercises in a girl who
already has contractures. But it is best to start them before contractures
begin. |
You can figure out similar exercises without motion for all the
weak muscles that need strengthening to help prevent or correct contractures.
For example, to strengthen the knee-straightening muscles, the
child can lie on her back with her leg as straight as possible. Have her tighten
the muscles on top of her thigh (without tightening those
underneath) and count to 25. Then relax and repeat 10 times. She should do this
3 or 4 times a day Again, look for ways to make it more fun.
Tightening this muscle (1) pulls the kneecap and rings the bell.

Figure
You can strap a small bell or flag to the leg, so that it will
ring or move when the knee bone moves.

Figure
Progression of exercises for the child with an ARTHRITIC
KNEE
(Arthritis often starts in the knee and later affects other
joints.)
CONCEPTS:
1. Strengthen the muscles that straighten the knee
(without strengthening those that bend it).
2. Do not move the knee when doing exercises.
3. Keep changing the position in which you do the exercise, and
add weights to make the exercises harder as the child’s strength
increases.
First exercise: leg on ground
First do the exercise without motion lying down.
Tighten here (1) without moving and count to 25. Relax and
repeat 10 times. Do it 3 or 4 times a day.

Figure
After a few days, do it sitting up.
Tighten here (2) without moving.

Figure
Second exercise: straight leg raise
1. With the leg straight, tighten the muscles on top of the
thigh (as in the first exercise).

Figure
When you lift the leg, be sure that the knee points up or
slightly (1) out to the side.

Figure
2. Then lift the leg without bending the knee, and slowly count
to 5 or 10.
3. Lower the leg slowly.
Figure
4. Rest.
Do not let knee bend at all (2). (If the knee bends even a
little when you lift the leg, it means that the muscles here are still too weak.
Go back to first exercise.)

Figure
When the child can do this exercise lying down without
bending his knee, begin putting weights on his leg:
Figure

Figure

Figure
For the weight, you can use a small bag full of sand.
Figure
After a few days, have him do the same exercise sitting up:*
|
* CAUTION: Do not do this sitting exercise if the
child has arthritis in the hip, or hip contractures. It uses the hip-bending
muscles that will make the contractures worse. |
Figure

Figure
Again, gradually increase the weight. Begin with half a kilo,
and build up to 5 kilos. But do not increase the weight until the child can do
the exercise at the first weight without bending his knee.
When the child can do the exercise at 2 kilos without bending
her knee, she can begin doing the following variation. Keep the leg raised the
whole time.
|

Figure
|

Figure
|

Figure
|

Figure
|

Figure
|
|
1. Tighten the muscle on top of the thigh. |
2. Lift the leg, keeping it straight. |
3. Move the leg to the side and turn it outward. |
4. Move the leg back in and turn it inward. |
5. Lower the leg and relax. |
|
IMPORTANT: If there is also arthritis in the hip, or
hip contractures, do these exercises lying down, not sitting up. |
Third exercise: knee slightly bent
1. Lie down with a rolled towel or blanket under the knee.

Figure
2. Turn the leg out to the side.

Figure
3. Lift the foot and slowly count to 5 or 10.

Figure
4. Lower it slowly.
5. Rest.
6. Repeat the exercise 10 to 30 times.
Make sure that only the foot is raised, not the thigh, and that
the knee is lifted as straight as possible.
As the child gains strength, continue with the same series of
steps as for the second exercise.
|

Figure
|

Figure
|

Figure
|

Figure
|
|
1. Lying down, lift the foot with a weight on it. Build weight
up slowly to 5 kilos. |
2. Sitting up, lift the foot without a weight. |
3. Sitting up, lift the foot with a weight. (Build up to 5
kilos.) |
If arthritis or contractures have begun in her hip, it is best
to do the exercise lying down with the hip as straight as possible (nothing
under the knee). |
|
|
Do these 2 exercises only if there is no danger of hip
contractures. |
|
To strengthen the muscles, continue the exercise until the child
can no longer hold the leg straight or it begins to shake slightly. The more
often the child does these exercises the faster the muscles will get stronger.
These exercises can be done even when the joint is swollen and painful. However,
if the joint hurts more during or after the exercise, use less weight and repeat
fewer times.
Exercising an ARTHRITIC KNEE through daily activities
WALKING. Walking is one of the best exercises for
strengthening the thigh - if the child puts some weight on the leg.
|
For arthritis, try to use canes, not crutches. A crutch can
cause contractures. |
NO |
YES |
A cane helps strengthen weak muscles and prevent
contractures. |
|

Figure
|

Figure
|
If he uses a cane, he must put some weight on the leg. This
strengthens the muscles that straighten the leg. |
|
WARNING: If a child uses a crutch and does
not step down with his leg, this strengthens only the muscles that bend the leg.
|
During the times when the child’s arthritis is less
painful, she should be active. It is fine for her to run, ride a bicycle, or
take long walks - as long as this does not cause much joint pain.
These activities strengthen weak thighs.
Walking uphill exercises the thighs more than walking on flat
ground.

Figure

Figure
After the child can walk fairly well without aids, a good
exercise is walking on the heels. (If the arthritis also affects the ankles,
this may not be possible. But try.)

Figure
SWIMMING. Swimming is one of the best exercises for a
person with arthritis.

Figure
Floating and play in water also is good exercise. The water
holds up the body and allows movement of the arms and legs without weight, yet
against the gentle resistance of the water.
Figure
Range-of-motion exercises for children with arthritis
For a child with arthritis, it is important that every day he
move his body, arms, and legs through as full a range of motion as possible.
But this is not always easy. Pain and stiffness make
straightening of joints difficult. So before starting to exercise, take steps to
calm the pain and relax the tense muscles. Aspirin helps do this. Take it
half an hour before beginning exercise (or before getting up to help morning
stiffness).
|
Note: Range-of-motion exercises for different joints
are described in Chapter 42. Here we discuss ways to make them easier for
children with arthritis. |
Heat helps relax muscles and calm pain. If many joints
are painful, it helps to lie in warm water (a little warmer than body
temperature).
If possible, get or make a tub large enough for the child to lie
straight and to stretch his arms and legs in all directions.
Warm water not only helps calm pain, but gently lifts and takes
the weight off body parts. This makes motion easier. Support the child only as
much as needed so that his arms and legs are loose and held up by the water. Ask
him to relax completely. Let him begin to move his arms and legs. The more he
relaxes, the more they will straighten as he moves.

Figure
Find ways for the child to play in the water. This will help him
forget his pain and make straightening the joints easier.

Figure
In moments when she has her leg or arm most straight, ask her to
hold that position a moment without bending.
This way, little by little, she will find she can straighten her
joints more and more.
Figure
‘Floating-in-air’ devices for relaxing and moving
painful joints
The best way for relaxing and reducing weight to exercise
arthritic joints is to float in warm water. When this is not possible, after
applying hot soaks, the leg or arm can be hung in a simple device - loosely, as
if floating in water.
‘FLOATING’ AN ARTHRITIC LEG

Figure
After hanging the limb, wait until the child relaxes, then have
him swing it gently this way and that.
Let the leg move with its own weight as in a swing. Increase the
swinging until the knee and hip bend and straighten completely (or as much as
possible).

Figure
Look for ways to turn the exercise into a game.
For example, the child might knock gourds or blocks down while
another child tries quickly to set them up again, and see who wins.

Figure
The gourds can be put farther and farther away so that he has to
stretch more each time to knock them down. When his leg is most stretched, ask
him to hold it that way a moment before letting it bend.
Also have the child do exercises lying on his back and swinging
his leg outward (to one side). This helps prevent knock-knee contractures.

Figure
A device like this helps strengthen the muscles that straighten
the knee. This way works better than a weight tied to the ankle because the pull
continues even when the knee is bent.

Figure
Put stones or pieces of metal in an old can. Use only as much
weight as will let the child straighten her knee completely. As the leg becomes
stronger, add more weight.
The child can also swing her leg while sitting or lying on a
table edge. Encourage her to swing the leg as far up and back as possible. Turn
it into a game.

Figure
Movement of the arms. This is done much like the legs:
|
LYING FACE UP |
LYING ON THE SIDE |
AND SITTING |
|
Swing the arm away from the body. |
Swing the arm forward and back. |
Swing the shoulder and elbow through their full range of motion.
|
|

Figure
|

Figure
|
Figure
|
|
These movements can be done keeping the hot soaks on the arm.
|
Encourage the child to move her limb in a rhythmic
manner-perhaps to music. Try to help her forget the pain. If she becomes
interested in something else - a game or the music-this will help reduce the
tightness of her muscles.

Figure
Look for ways to do these movements as part of daily activities.
CORRECTING CONTRACTURES CAUSED BY ARTHRITIS
For general information on the cause, prevention, and
correction of contractures, see Chapter 8. Range-of-motion and
strengthening exercises will help prevent or correct early contractures (see
Chapter 42). For severe contractures, stretching aids or casts may be
needed (see Chapter 59). However, when using casts or other aids to straighten
contractures, it is very important to continue exercises without motion
to strengthen the muscles that straighten the limb.
PRECAUTIONS FOR CASTING AN ARTHRITIC LIMB
1. First examine the joint for signs of dislocation. Try moving
the bones forward and backward and from side to side.

Figure
CAUTION: If the joint is partly
dislocated or very loose, it is best not to use casts or stretching devices, as
these can increase the dislocation. It is better to continue with the
exercises, taking care not to force the joint.
2. If there are no signs of dislocation, little by little
straighten the joint as far as is possible without causing much pain.

LIKE THIS
CAUTION: Do not pull like this, or you may dislocate
the joint.

NOT LIKE THIS
3. With the joint as straight as you can get it without too much
pain, carefully cast the leg.

Figure
Until the cast dries, apply steady pressure here (1) so that the
bones keep their right locations and the joint stays straightened.
4. As long as the cast is in place, do without-motion exercises
several times a day. This helps keep the straightening muscles strong.

Figure
You can cut a hole above the kneecap (2) to be sure it moves
when she tightens her muscles.
5. Every 2 days remove the cast, apply heat and do
range-of-motion exercises, bending and straightening the leg little by little.
Then gently stretch the leg a little more, and put on another cast.

Figure
(IMPORTANT: It is best to replace the cast
completely rather than to use wedges with the same cast, because of the risk of
dislocation.)
6. Continue straightening the leg with new casts every 2 days
until it is completely straight or does not straighten more.
Keep a record of the progress like this (see Chapter 5). This
way you can tell when the leg is no longer getting straighter and it is time to
stop using casts.
Figure
Homemade aids for stretching joints
Because daily movement of joints is so important with arthritis,
casts should be avoided whenever possible. So try to figure out other ways to
correct contractures. Use whatever materials you can find, such as plastic,
bamboo, and inner tubes.
These are a few of the examples of aids invented in a Mexican
village for a girl with arthritis.
|
CAUTION: Make sure that the aids pull in a way that
does not cause dislocations. |
KNEE

METHOD 1
METHOD 2
Note: The behind-the-knee aid usually works the
best. It is steadier and so causes less muscle tightening. Because it holds the
leg more firmly, it is less likely to cause dislocations. It is also more
comfortable and less awkward.
WRIST
Over-the-hand support

Under-the-hand support
|
PRECAUTIONS in the use of aids for stretching
contractures:
· They should be
made in a way that will prevent dislocations. When using, check often for
early signs of dislocation.
· The aids should not pull so
much that they cause pain and defensive muscle tightening.
· Use them during most of the
day and at night (about 20 of every 24 hours).
· Remove them 2 or 3 times a day
in order to do exercises.
· Also do exercises without
motion with the aids in place.
· Take care that the aid does not stop blood flow or
press on nerves. If the hand or foot becomes cool, changes color, begins to hurt
or becomes numb-remove the aid, and make the needed adjustments. |
For other aids and devices for straightening contractures,
see Chapter 59.
Correcting contractures of arthritic hips
Look for ways that the child can relax with her head as straight
as possible. If she also has contractures in her knees, she can lie like this.
The child will relax and straighten her body more easily if she
can play or read.
(1) Place supports or cushions behind her back and head, but
just enough so that she has to straighten herself some. As her hips and neck
gradually straighten, keep lowering her back and head little by little.
(2) Give just enough support under her knees and feet to keep
her hips and knees stretched. As they gradually relax, lower her knees and raise
her feet little by little, so that her hips and knees straighten.

Figure
In the morning, she may be stiff and bent, and will need help to
straighten like this every day - or several times a day.
If possible, also have her lie on her belly.
Think of games or exercises in which the child will stretch his
hips and knees. In this example, the boy rolls the log to lift the flag and hit
the gourd. This helps strengthen the straightening muscles of his legs.
As the child’s back, hips, and knees straighten more and he
gains strength, the hammock can be stretched more tightly and a heavier weight
put on the top of the stick, where the flag is.

Figure
A homemade walker similar to this can help a child with hip
contractures begin to walk. It also provides exercise for the straightening
muscles of both the arms and legs.
As the child’s hips and knees straighten more and more, the
crutches and seat can be raised.
It is best if she walks backward (“Pretend you’re a
crab!”). This way she will strengthen the straightening muscles in her
legs. Walking forward would strengthen more the muscles that bend the legs, and
this could increase contractures.

Figure

ADJUSTABLE SEAT
|
LEARNING TO MOVE AND TO SMILE-the story of Teresa
Teresa has had juvenile arthritis since age 7. When her mother
first brought her to PROJIMO from a distant village at age 14, her body had
stiffened into the shape of a chair. Her eyes were the only parts of her body
she could move. Her joints hurt her so much that she spent every night crying.
Years before, a doctor had prescribed aspirin for her pain. But the aspirin
began to give her severe stomach pain, so she stopped taking it.
Once Teresa was a cheerful, active little girl. She had
completed 3 years of school. Now she was sad and felt hopeless. She would cry
out with pain each morning when her father carefully lifted her out of bed and
sat her in a chair. She rarely spoke and never smiled.
When Teresa arrived at PROJIMO she had severe contractures of
her wrists, fingers, elbows, hips, knees, ankles, and feet. The rehabilitation
team had her start using aspirin again, but with care that she take it with
meals, lots of water, and an antacid. They then began a long, slow process of
therapy, part of which we show in the following photos.

To help correct her wrist
contractures, visiting therapists made these splints for her out of costly
plastic.

However, to the therapists’
surprise, they found out that these low-cost splints made by villagers from a
plastic bucket worked better.

Every day the team spent several
hours with Teresa, gently doing range-of-motion, stretching, and strengthening
exercises. Here a visiting physical therapist teaches a village worker how to
help Teresa increase movement in her stiff neck and back.
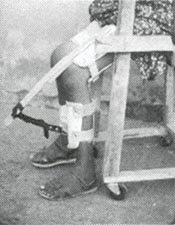
They also made leg splints out of
plastic buckets and strips of rubber tire tube.

When Teresa could move her joints
some, the team made her an adjustable walker. It had shoulder supports and a
saddle seat that could be raised as her legs straightened. She learned to walk
by pushing herself backward. This strengthened the muscles that straighten her
legs.
Teresa was improving steadily. She began to talk, smile, and to
take interest in things. An older brother came to visit for a few weeks. He
learned about her exercises and therapy so he could help her when they returned
to their village.
Unfortunately, soon after Teresa went home she became ill with
dengue (break bone fever) and nearly died. Her family stopped both exercises and
medicines. When she returned to PROJIMO 6 weeks later, she was as stiff and bent
as when she first came. She was so depressed she spoke to no one. The team began
her rehabilitation all over again.

This time they straightened her
legs and arms with plaster casts (see Chapter 59). They changed the casts every
2 days. With each cast change her joints were exercised.

Finally, with the casts,
Teresa’s knees and wrists became fairly straight. She now had some hand
movement and could play in the playground.

Exercise in the therapy pool at
PROJIMO was fun and greatly improved her movement.

Kicking balls with other disabled
children helped Teresa strengthen muscles that straighten legs.

Village children help her with
activities to use her hands. Here she weaves a basket.

When her legs were stronger, the
team made an adjustable standing frame for her.

Later Teresa began to walk using
a homemade walker with wood wheels. She wore leg braces for support.
As Teresa’s legs and arms straightened, her neck bent
forward more and more. She could not lift her chin from her chest. The village
workers made her a head support, attached to a firm cloth around her chest. Over
a period of months, the support gently brought up her head.
Teresa is now able to walk with crutches. Through daily work
she gets much of the same therapy she gets doing her exercises.

Figure

Figure

Figure

She also continues with her daily
exercises to straighten and strengthen her arms and legs.

Sewing together with her friends
helps Teresa improve the use of her hands. She is also gaining skills with her
therapy.
(5 photos by Richard Parker)

At home, Teresa now helps care
for her younger brothers and sisters. She and her family share the household
tasks. Before, others had to take care of her.
(photo by Andy Brown) |
|
Chapter 17: Rheumatic Fever
Rheumatic fever is a serious illness with joint pain
and fever. It usually lasts about 6 weeks but may last up to 6 months (or
rarely more). Then the joint pain usually goes away completely. But heart
damage, if it has occurred, may be permanent or become
disabling (shortness of breath; sickly child).
CAUSES
Rheumatic fever usually results after a sore throat
caused by bacteria called ‘streptococcus’. (The rheumatic fever is
somewhat like an allergic reaction.) A ‘strep throat’ often starts
suddenly with throat pain and fever and without signs of a cold.
Rheumatic fever is most common where epidemics of strep throat are common -
in crowded communities with poor hygiene.
PREVENTION
Rheumatic fever can often be prevented by giving penicillin to
children who have signs of a strep throat. Keep giving penicillin for at least 3
days after all signs disappear. Long-term prevention involves improving hygiene
and living conditions (a fairer society).
|
CAUTION: Most sore throats in children are
not ‘strep’, but are caused by the common cold; these should
not be treated with penicillin, or any other antibiotic and never
injections. Typically, a strep throat is quite painful and starts suddenly,
with high fever, and without a stuffy nose or other signs of a cold.
|
|
SIGNS OF THE TYPICAL CASE
· Child between the
ages 5 to 15
· Began 1-3 weeks after the
child had a severe sore throat
· High fever - child
quite sick
· Joint pain. Pain often
starts in one or more of the larger joints (especially wrists and ankles). Then
it changes to other joints, often knees and elbows. The painful joints may swell
and become red and hot.

Figure
· Child gets well in
about 6 weeks to 3 months, but may get the same illness again after another
sore throat.
OTHER SIGNS (not always present)
· Reddish curved
lines on skin
· Lumps (the size of
peas) under the skin over or near the joints
· Heart problems. You may
hear a ‘murmur’ if you put your ear over the child’s chest.
Instead of the typical ‘lub-dub... lub-dub’ of the heartbeat, you will
hear a soft, long ‘whoosh’ for one of the sounds: ‘whoosh-dub...
whoosh-dub... whoosh-dub’. The ‘whoosh’ sound means a valve to
the heart has been damaged so that it does not close completely. In extreme
cases this can lead to heart failure (see Where There Is No
Doctor, p. 325).
·
Nosebleed, belly pain, chest pain, or signs of pneumonia occur in only a few
cases. |
Treatment
· If you think a child might
have rheumatic fever, get medical advice quickly. Early treatment may help
prevent heart damage. (After fever and joint pain have begun, treatment does not
seem to shorten the length of the illness.)
· Give penicillin by mouth for
10 days; or give a single injection of benzathine penicillin G into the butt
muscles (one-half in each butt); or inject procaine penicillin
daily for 10 days. For children who are allergic to penicillin, use
erythromycin. See box for doses. (For cautions in the use of
penicillin, see Where There Is No Doctor, p. 351.)
· Give aspirin in high dosage.
An information sheet with the dosage and precautions for taking aspirin is in
the previouses pages. Continue giving aspirin until a few days after all signs
are gone.
· Apply heat or cold packs to
painful joints to help reduce pain and swelling.
· Do full range-of-motion
exercises of painful joints gently every day (see Chapter 42).
· Do ‘exercises without
motion’ to maintain strength.
· The child should stay in bed
or rest quietly most of the time until all signs are gone (about 6 weeks). Then
he can begin activities little by little.
|
TREATMENT OF RHEUMATIC FEVER |
|
Name of medicine |
Age |
Dose |
When to take |
|
Penicillin V or G
(by mouth) |
up to 3 years |
125 mg. |
4 times a day for 10 days. |
|
over 3 (includes adults) |
250 mg. |
|
|
OR |
|
|
|
|
Benzathine penicillin
(by injection) |
up to 3 years |
600,000 units |
single injection (Give one-half in each butt.) |
|
over 3 (includes adults) |
1,200,000 units |
|
|
OR |
|
|
|
|
Procaine penicillin
(by injection) |
up to 3 years |
600,000 units |
Inject one-half into each butt muscle once a day for 10 days.
|
|
over 3 (includes adults) |
1,200,000 units |
|
|
For persons allergic to penicillin give: |
|
Erythromycin
(by mouth) |
up to 3 years |
125 mg. |
4 times a day for 10 days. |
|
over 3 (includes adults) |
250 mg. |
|
|
NOTE: Whenever possible, it is safer to
give children medicine by mouth than by injection. |
PREVENTION of repeat attacks
Persons who have once had rheumatic fever have a risk of getting
it again. For these persons, take care to treat any sore throat quickly with
penicillin. If the person shows signs of heart damage (murmur) with the first
attack, there is a high risk of further damage with repeat attacks. These
persons would be wise to take a preventive dose of penicillin regularly for at
least one attack-free year or until they are 17 years old (after which the risk
of strep throat is lower). Long-term prevention is especially important in
persons who already have serious rheumatic heart damage.
|
PREVENTIVE DOSAGES:
· or 1 injection of
1.2 million units of benzathine penicillin G, once a month,
· or 1 tablet of 500 mg. of sulfadiazine 2 times a
day,
· or 1 tablet of 250 mg. of potassium
penicillin V, 2 times a day with an empty stomach.
· For children allergic to penicillin, give 1 tablet of
250 mg. of erythromycin, 2 times a day.
Before using these medicines, read the precautions. See the
GREEN PAGES of Where There Is No Doctor. |
Chapter 18: Hip Problems
DISLOCATED HIPS
A hip is dislocated when the thigh bone is out of
its socket at the hip. Some babies are born with one or both hips already
dislocated. Sometimes these babies have no other problem. With early treatment,
the problem can often be corrected easily, and the child will not be
disabled or have a limp.

Figure
(1) NORMAL HIP: The round head of the thigh bone is
inside the hip socket.
(2) DISLOCATED HIP: The round head of the thigh bone often lies
above the socket.
For this reason it is important to examine all babies when
they are 10 days old to see whether they have dislocated hips.
1. Compare the 2 legs. If one hip is dislocated, that side may
show these signs:
· the upper leg
partly covers this part of the body (1)
·
there are fewer skin folds (2)
· the leg may
seem shorter, or turn out at a strange angle (3)

Figure
2. Hold both legs with the knees bent, like this,

Figure
If one leg stops early or makes a jump or click when you open it
wide, the hip is dislocated.

Figure
3. To test a slightly older child, bend the knees and compare
their height.
If one knee is lower, the hip on that side is probably
dislocated.

Figure
Treatment
Keep the baby with his knees high and wide apart. To do this,
· use many thicknesses of
diapers (nappies) like this,

Figure
· or pin his legs like this
(when the baby sleeps),

Figure
· or carry the baby like this.

Figure
In places where babies are traditionally carried with their legs
spread on the woman’s hips or back, usually no other treatment is
necessary.
Dislocated hips with other orthopedic problems
Children with the disabilities listed here often
are born with dislocated hips. Therefore, it is essential
to examine these children carefully a few days after birth, to make sure there
are no dislocations.
· Down
syndrome
· spina
bifida
·
arthrogryposis
· cerebral
palsy
· club feet
Many (but not all) dislocated hips can be corrected in the ways
we described. Keeping the legs wide apart during the first months of the
child’s life helps to improve the shape of the socket.
If it is difficult to keep the legs apart, you may need to use
casts or make special braces.
CAST
The casts should be used for 2 to 4 months or longer, depending
on the child’s age (longer for older children) and the amount of the
deformity. (Use a cloth or bottle to catch the baby’s pee, so it does not
run inside the cast.)

BRACE
Not all dislocations can be corrected in these ways. Some need
surgery, and in some cases the hip is so deformed that the dislocation cannot be
corrected, even with surgery.
With spina bifida, if one hip is dislocated, surgery may help.
But if both hips are dislocated, hip surgery usually will not help the child to
walk any better.
Dislocated hips can also occur after the child is born,
either from an accident or as a complication of some other disability -
especially polio (due to weakness in the muscles and cords that hold the
hip joint together) or cerebral palsy (due to spasticity
and contractures).

Figure
THE TELESCOPE TEST
To find out if the hip is dislocated or can easily be pulled out
of joint, place the child on his back.
Pull up on his knee, and than push it down, like this (1).
At the same time, feel his hip with your other hand, like this
(2).

Figure
If the thigh bone moves in and out like a telescope, the hip is
probably dislocated.

Figure
Dislocations that are complications of polio or cerebral palsy
can seldom be corrected without surgery. But often it is better not to
operate, because the operations do not always turn out well, and the
children who have the possibility of walking will walk in spite of the
dislocated hips.
HIP PROBLEMS DUE TO DESTRUCTION OR SLIPPING OF THE CAP OF THE
THIGH BONE
There are 2 different hip problems that occur most often in very
active children, usually boys.
1. Destruction of the cap or ‘growth
center’ on the ‘head’ of the thigh bone is called Legg-Perthes
disease. It usually begins between 4 and 8 years of age. It occurs in
one of every 300 to 600 boys.
2. Slipping of the cap on the head of the thigh bone is
less common. It happens, suddenly or little by little, usually between 11 and
16 years of age (when the child is growing fast).
|
SIGNS:
· Child begins to limp:
body dips toward affected side.
Figure
· Often he does not complain of
pain.
· Or he may feel some
pain in the knee or thigh (or less often, hip) - although the problem is
at the hip.

Figure
· Motion for bending, or opening
of hip may become somewhat limited, or painful if he tries to bend it more.
· In time the thigh becomes
thinner and weakness develops in the muscles that lift the leg sideways.
Figure
|
The cause in both cases is often unknown but may be
related to an injury caused from jumping or falling.
Destruction of the growth center results from a temporary loss
of its blood supply, which results in death of the bone.
DIAGNOSIS: If a child has signs of one of these problems,
try to get an X-ray to find out the cause.
Figure

Figure

Figure
Destruction of the growth center is usually not related to other
diseases. In some cases, however, destruction of the growth center from loss of
blood supply is caused by tuberculosis of the hip, sickle cell anemia,
cretinism, or use of corticosteroid medicines. A careful medical study is
advisable.
Treatment and progress of Legg-Perthes disease
When the growth center has lost its blood supply, the bone dies
and begins to break into pieces. At the same time, the body begins to make new
bone. In 2 to 3 years a new growth center is completely formed, and the child
walks more or less normally again, usually without pain. However, the new growth
center is usually flatter than before and does not fit into the hip socket as
well. As a result, after several more years, the hip joint begins to wear out
and a progressive, destructive, painful arthritis may begin.
Many ways to treat Legg-Perthes have been tried. Most methods
try to keep the leg in a position that makes the growth center form a round and
normal shape again.
An old method was to prevent weight bearing and
keep the hip bent in a sling. THIS DOES NO GOOD. We mention it
only because in some countries children are still made to use slings and
crutches for years.

Figure
A newer method was to cast or brace the
legs wide apart.

Figure
full-leg braces

upper-leg braces only
Casts or braces were kept on the child until the new growth
center formed completely - usually for 2 to 3 years! This was very hard
on both the child and family.
An even newer method was surgery. The surgeon cut loose a
piece of bone (1) containing the hip socket,

Figure
and turned it (2) so the head of the thigh bone fit deeper into
the socket. (The result was similar to widely separating the legs.)

Figure
Surgery was expensive and had more risks. But it was much
quicker: only 6 weeks’ bed rest with a cast. Then the child could lead a
more or less normal life, without slings or braces. But it still took 2 years
for the new growth center to form, and during this time the pain and/or limp
continued.
Recent studies show that none of these methods - sling,
casts, braces, or surgery-makes any real difference. Treated or not, the
pain and limp gradually go away - and are likely to come back as arthritis years
later. Although many doctors still recommend one or another of these treatments,
usually the best advice to parents is to DO NOTHING. (This is a hard
decision for parents to accept, but will make life happier for both the child
and family.) Let the child remain active, but do not make him run, jump, or walk
far if it bothers him. Moderate exercise is important. Swimming is
excellent.
Treatment and progress of slipped growth center
When the growth center slips, if possible it should be put back
into place surgically, and pinned. When surgery is impossible, the child should
avoid all strenuous exercise, running, and jumping in the hope that the growth
center will not slip farther until it becomes fused to the thigh bone (normally
when the child is 16 to 18 years old). Without surgery, and especially if the
slippage is severe, a progressive destructive arthritis is likely to
result.
Chapter 19: Bone Infections
Osteomyelitis
Bone infections are mostly a medical problem.
Therefore we do not describe all of the many types of bone infections or details
of medical and surgical treatment.
Chronic (long-lasting) bone infections are fairly common
in villages where persons go barefoot and where injuries and illnesses that can
lead to bone infections are frequent. They can be caused by fungus, or by many
different kinds of bacteria (including typhoid, tuberculosis, and
staphylococcus). Often these infections last for years, causing bone destruction
and severe disability.
Bone infections are a very common complication of injuries,
burns, and pressure sores in persons who have no feeling in their hands and
feet. This includes persons with spina bifida, spinal cord
injury, and leprosy. Because the person does not feel pain, often she
does not rest, clean, or protect the injured area. As a result, it becomes
infected. Gradually the infection gets deeper until it reaches the bone.
|
THROUGH PROPER EARLY CARE OF SORES AND INJURIES, BONE INFECTIONS
CAN USUALLY BE PREVENTED. |
The loss of parts of the body sometimes seen in a person who has
leprosy (Hansen’s disease) is not caused by the leprosy germs. It is caused
by other germs, which infect the bone because of injuries the person gets that
are not cared for because they do not hurt.

Figure
|
WARNING: Deep pressure sores that do not
heal, even after they are kept clean and no weight or pressure has been put on
them for months, may have a bone infection. Bone infection is especially likely
if the sore reaches the bone, or if a small hole at the bottom of the sore
refuses to close and drains liquid or pus. If you think there might be a bone
infection, get medical help if possible and go through all the steps to treat it
adequately.

Figure
|
Signs of chronic bone infection
· The skin near a
bone has small, deep sores that heal and then open again to drain pus. Gradually
the affected area gets bigger and new holes open.
· There may or may not be pain.
· The pus may or may not smell
bad.
· Usually there is no fever -
except sometimes at first or at times when the infection gets into the blood.
· Often the infection will get
better with antibiotics, but keeps coming back.
· The affected bone may
gradually become thicker as it is destroyed inside and forms a new bony
covering.

Figure
Treatment
· Whenever possible
get experienced medical help.
· If treated early with the
right antibiotics in the right (high) dosage, sometimes the infection will go
away and not come back. If possible, a sample of the pus should be studied
(cultured) by a medical laboratory to find out what kind of infection it is and
what medicine is likely to work best. Usually the medicine should be taken for a
long time (months).
· If you cannot get the pus
cultured, you might try treating the infection with tetracycline (by mouth), or
dicloxicillin (a special penicillin). Use relatively high doses. For dosage and
precautions, see Where There Is No Doctor or a medical text.
· Surgery may be needed to
remove the dead, infected bone.
· Sometimes amputation is
necessary.
· Even with excellent treatment,
after months or years without problems, new sores may open and again begin to
drain from the infected bone.
Rehabilitation and aids
What kind of rehabilitation or
orthopedic aids may be needed will depend on the amount of
destruction that has occurred. Sometimes surgery cannot be obtained or the
person may prefer to live with the problem rather than with an amputated limb.
For prevention, rehabilitation, and aids, see Chapters 24, 26,
and 58 on pressure sores, leprosy, and braces.
When there has been a lot of bone destruction, sometimes a brace
can help make walking easier.

Figure
Large hole down to the bone in the foot of a woman with a bone
infection (osteomyelitis). She has had this problem since childhood 30 years
before.
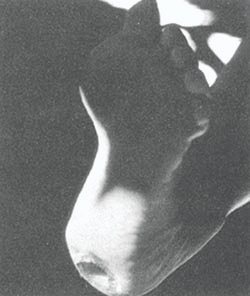
Figure
|
WARNING: The pus coming from the infected
bone may cause serious infections in other persons. Change bandages regularly;
boil them before using them again, or burn them. Wash hands often. Take great
care with hygiene. |
Chapter 20: Spinal Curve and Other Back Deformities
The backbone, or ‘spine’, is a chain of
bones called ‘vertebrae’ that connect the head to the hipbone.
Separating each of the vertebrae is a small cushion called a ‘disk’.
The backbone holds the body and head upright. It also encloses, in its hollow
center, the ‘spinal cord’ or trunk line of nerves
connecting the brain to all parts of the body.
Figure
|
NORMAL SHAPE OF THE BACKBONE
Figure
Normally, the backbone (and back) is straight when seen from the
back, and has 4 curves when seen from the side. |
|
Sideways curve
(scoliosis - S-shaped curve) |
|

Figure
|
May result from unequal paralysis of back muscles
or from a hip tilt due to one shorter leg. Sometimes the cause is not known.
|
|
Rounded back
(kyphosis) |
|
Figure
|
May result from weak back muscles or from poor posture (bent
over position when standing or sitting). |
|
Swayback
(lordosis) |
|

Figure
|
May result from weak stomach muscles, from hip
contractures, or from the way a child walks to make up for
a weak leg or hip. |
|
Sharp bend or bump in spine
(tuberculosis of the
backbone) |
|

Figure
|
Results from destruction of one or more vertebrae by
tuberculosis infection |
Of these different problems, scoliosis or a sideways curve is
the most common serious problem. Often, however, rounded and/or swayback are
seen together with scoliosis.
NON-FIXED AND FIXED SPINAL CURVES
With a non-fixed or ‘functional’ curve
there is no deformity of the vertebrae. This usually happens when the body tries
to stand straight even though the hips tilt or there is other unevenness not in
the spine.
For example, a child with a shorter leg from polio will stand
with his hips tilted (1). For him to stand straight, the spine has to curve.

Figure
A non-fixed curve can usually be straightened by putting blocks
under the foot (2), or by holding the child up under the arms.

Figure

Figure
Fixed or ‘structural’ curves are deformities in the
bones of the back themselves.
A fixed curve cannot be straightened, by positioning or holding
up the child.

Figure
|
Note: In some cases, with time a non-fixed curve may
gradually become fixed. |
CAUSES OF SPINAL CURVE (SCOLIOSIS)
Most scoliosis (about 80%) occurs in otherwise healthy
children for no known reason. Sometimes it occurs in several members of the same
family, so there may be a hereditary (familial) factor. Although
about 1 of every 10 persons has some scoliosis (if looked for), only about 1 in
400 has enough of a curve to be a problem. Curves of unknown cause are often
first seen - and progress quickly - in children from 10-16 years old, during the
period of rapid growth.
Known causes of fixed scoliosis range from
infection to tumor to rare disease. When possible, consult a
doctor with experience in these problems.
Some children are born with fixed scoliosis, or develop it in
early childhood, because of defects in the spine itself.
These problems can only be identified by X-rays.

Figure

Figure
Non-fixed scoliosis always results secondary to other
problems, such as uneven paralysis of the back muscles, or a hip tilt (often due
to a shorter leg). Spinal curve often develops in children with polio,
cerebral palsy, muscular dystrophy, spina bifida, spinal cord injury,
arthritis, and dislocated hip. Be sure to examine all children with
these disabilities for spinal curve. With time, non-fixed curves
may gradually become fixed.
Examining for spinal curve
This is discussed in the chapter on physical examination
(Chapter 4).

Figure
Look along the line of the back with the child bent over.

Figure
Figure
The rib hump is formed because where the spine is curved, the
vertebrae also are twisted to one side.

Figure
|
POSSIBLE SIGNS OF EARLY SCOLIOSIS
1. one shoulder higher than other
2. One shoulder blade
sticks out more.
3. One hip is higher or sticks out more than the
other.
4. One arm hangs closer to body than the other.
5. swayback
6.
rounded shoulders or ‘hump back’
7. a larger crease at one side of
waist than other
8. Child stands sagging or leaning to one side.
9. rib
hump (when child leans forward)
10. a hump near the waist (when leaning
forward)
11. a brother, sister, parent, or close relative with scoliosis
|
CHECK FOR:
Figure
overhead view of vertebrae
When you examine for scoliosis, also check to see if the curve

can be straightened
(non-fixed),

or cannot be straightened
(fixed).
What to do
This will depend on:
· how severe the
curve is.
· if it is getting worse - and if
so, how quickly.
· whether the curve is
fixed.
· the age of the child.
|
In a child who does not stand, check spinal curve while he is
sitting. If one side of his butt is weaker and smaller, it may cause a hip
tilt.

Figure
Put a book or board under the weaker butt, and see if this
straightens his spine. If so, a cushion raised on one side may help him sit
straighter. |
How severe the curve is and whether it is getting worse can be
best measured by X-rays.
1. For each curve, pick the 2 vertebrae that tilt most in
relation to each other.
2. Draw lines level with the top of each vertebra.
3. Measure and record the angle of the spinal curve.

Figure
4. Regularly record the curve and notice any changes.

Figure
Because X-rays are expensive and often hard to get, you can get
some idea of whether the curve is getting worse by measuring the angle of the
rib hump.
Have the child stand or sit as straight as possible, while he
bends forward.
Be sure the top piece is completely level (1). You can use a
carpenter’s level or a homemade one (see box).
Measure this angle (2).

Figure
|
A home made level for measuring rib hump angle
Fill the tube (1) with colored water so that the water reaches
the top edge of the board at both ends when level.
(2) piece of thin plastic tube (old I.V. tube)
When measuring the rib hump, level the top (3) by making sure
the water is at the top edge of the board at both ends.
Figure
|
If the rib hump angle stays about the same month after month,
the curve is probably not getting worse. Keep checking it every few months. If
the rib hump angle increases steadily, the curve is getting worse. X-rays should
be taken and a decision made about what to do.
Non-fixed curves that are not getting worse should
usually be treated only by doing something about the underlying problem.
For example, if the child’s spinal curve is not fixed and
comes from a hip tilt due to unequal leg length:
Measure the difference in leg length

Figure
Level the hips by standing on books or boards.

Figure
Put a lift on shoe or sandal
Figure
This child was developing a spinal curve due to hip tilt and
short leg.

Figure
Village rehabilitation workers put a lift on his sandal.

Figure
This corrected his spinal curve and lop-sided posture.
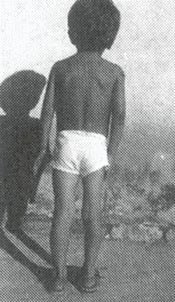
Figure
Body jackets or bracing for a non-fixed curve usually do
not help to correct the curve or even to prevent its getting worse. However, for
a child with a curve so severe that it makes sitting or walking difficult, a
body jacket or corset may help.

Figure
Spinal curves under 20° (fixed or non-fixed) usually
need no special care - other than to be watched, and measured every few months
to see if they are getting worse.
Some experts say that exercises to strengthen the back muscles,
like this (1), help correct and slow down the curving of the spine. Other
experts say it does no good. (We do not know.)

Figure
Spinal curves over 20°, if they are fixed and
getting worse, may get worse less quickly with a brace.

Figure
A brace like this (the Milwaukee brace) is often used. It works
because it is so uncomfortable that the child must stretch his body as straight
as possible to reduce the discomfort.

Figure
A plastic ‘Boston brace’ like this is more
comfortable, can be completely hidden under the clothes, and probably does as
much good.

Figure
SURGERY
For spinal curves over 50° which are quickly getting worse,
surgery may be needed. Surgery ‘fuses’ (joins together) the most
affected vertebrae. Usually it only partly straightens the spine. Except for
very severe curves, surgery should be avoided in children under 12 years old
because the fused part of the spine will not grow any more.
If the curve of the spine is less than 40° by the time the
child stops growing, usually it will not progress further. If the curve is over
50°, it is likely to keep getting worse even after the child stops growing,
and surgery is often recommended.
However, ‘spinal fusion’ surgery is very costly and
requires an orthopedic surgeon specially trained in this
operation. It can also be very hard on the child and family. When surgery cannot
be obtained, a body jacket or brace should perhaps be used to help slow down the
curve’s progress. When a curve becomes too severe, there is no longer
enough room in the chest for the lungs and heart to work well, and the child may
get pneumonia and die.
EXERCISES FOR ROUNDED BACK AND SWAYBACK
Children with rounded back may benefit from exercises to help
straighten it, like this (1).

Figure
These exercises are explained in the Exercise Sheet #5.
The child should also be encouraged to sit and stand as straight
as possible, with the shoulders back.
Children with swayback may benefit from exercises to strengthen
the stomach muscles, like this (2),

Figure
or by exercises to correct hip contractures (if the child has
them). See Exercise Sheet
#3.
Chapter 21: Tuberculosis of the Backbone: Pott’s Disease
Tuberculosis (TB) of the backbone is not common, but is still
seen in poor communities, especially in children. It is the most common form of
tuberculosis of the bone.
It is important to recognize and treat it early, before
damage to the backbone causes nerve damage and
paralysis.
If a child begins to develop a sharp bend in the middle
section of the backbone, with shortening and thickening of the chest, it is
probably tuberculosis of the spine. You can almost be sure it is, if someone
in the family has TB of the lungs.
As the spine collapses forward, the child may have
to hold himself up using his arms.

Figure
Seek medical help quickly. Skin test, X-rays (of the
chest and spine), and microscope examination of pus from abscesses (pockets of
pus) may help in the diagnosis. If the X-ray shows typical bone destruction, the
child should be treated for tuberculosis even if no TB germs are found.
|
SIGNS
· It begins little by little -
often without pain at first.
· A bump develops in the
backbone. This is because the front part of one or more vertebrae is destroyed
and collapses.

Figure

Figure
· The child has trouble bending
over to pick things up.
· An abscess full of pus may
form near the lump in the spine. It may open lower on the body and drain pus.
· As the condition gets worse,
back pain may begin.
· Signs of spinal cord
injury may develop: pain, numbness, weakness or paralysis in feet and legs, and
loss of urine and bowel control. (See “Spinal Cord Injury”)
· TB skin test is usually
positive. (However, the skin test is of use only if the child has not been
vaccinated against TB.)
· Often someone in the home has
TB.
· Only half of children with TB
of the spine also have TB of the lungs. |
Treatment
· Use 2 to 3 TB medicines
for at least a year, as for TB of the lungs. (See Where There Is No
Doctor, p. 180.)
· A back brace may help
keep the damaged spine straighter. It can be made of plaster, or of plastic
using techniques similar to those used for making plastic leg braces.
Or make a very simple back brace from a metal tin or drum:
1. Cut an oval piece from a heavy tin.

Figure
2. Hammer the tin to fit the child’s back.
Without forcing, try to put the back in the straightest position
possible.

Figure
3. Pad the tin and wrap it with a soft
cloth.

Figure
4. With an elastic bandage, bind the plate firmly to
the child’s back.

Figure
|
CAUTION: Make sure the bandage does not hurt the
child, damage his skin, or make it difficult for him to breathe. |
The child in the photo on the previous page was effectively
braced by a traditional bonesetter in this way.
· In severe or advanced
cases, surgery may be needed to help straighten and stabilize the bones
of the spine.
|
CAUTION: Because of the risk of paralysis, an
orthopedic surgeon should be consulted if possible. |
Hopes for the future
With early, complete treatment the damaged bones will usually
heal and the child may live normally, although often somewhat hunched over.
If nerve damage and paralysis have begun, sometimes surgery (or
even bracing during treatment) can bring some improvement.
When nerve damage is severe, rehabilitation will
be the same as for spinal cord injury (see Chapters 23, 24, and 25).
PREVENTION consists of early diagnosis and treatment of
tuberculosis, and in the fight against poverty. Vaccination against TB may also
help.
Chapter 22: Spina Bifida
WHAT IS IT?
Spina bifida (also called meningocele or myelomeningocele) is a
defect that comes from a problem in the very early development of the unborn
child. It happens when some of the back bones (vertebrae) do not close over the
center tube of nerves (spinal cord). As a result, a soft
unprotected area is left, which may bulge through the skin as a dark bag. This
‘bag of nerves’ is covered by a very thin layer (membrane) which may
leak liquid from the spinal cord and brain. Nobody knows what causes it.
But 1 of every 250 to 500 babies is born with spina bifida.

Figure
Problems that occur with spina bifida
(1) High risk. Without early surgery to cover the bag of
nerves, it almost always gets infected and the child dies of
meningitis .
(2) Muscle weakness and loss of feeling. The legs
or feet may be paralyzed and have little or no feeling.
(3) Hips. One or both hips may be
dislocated.
(4) The feet may turn down and in (club feet), or up and
out.

Figure
(5) If the defect is relatively high up the back (L1 or above,
see next page), there may be muscle spasms (spasticity) in the
legs and feet.
(6) Poor urine and bowel control. The child may not feel
when he pees or has a stool. When he gets older he may not develop control, and
will pee or shit without knowing it.
Figure
(7) Big head. ‘Hydrocephalus’, which means
‘water on the brain’, develops in 4 out of 5 children with spina
bifida. The liquid that forms inside the head cannot drain normally into the
spinal cord, so it collects and puts pressure on the brain and skull bones.
Although the child’s head may look normal at birth, little by little it
becomes swollen with liquid, like this.
(8) very big head
(9) big veins
(10) The eyes may turn downward because of pressure in
the head. This ‘setting sun sign’ means danger of blindness and
severe brain damage.

Figure
(11) Brain damage. Without early surgery to lower the
pressure of the liquid in the head (and sometimes even if the surgery is done),
some children become blind, mentally retarded, have fits (epileptic seizures),
or develop cerebral palsy (see Chapter 9).
PROBLEMS THAT MAY OCCUR WHEN THE CHILD IS OLDER:
(1) Curve of the spine (See Chapter 20.)
(2) Urinary infections and kidney damage
Figure
(3) Pressure sores may form over the bones, because the
child cannot feel. (See Chapter 24.)

Figure
(4) Foot injuries. Children who can walk but have no
feeling in their feet may easily develop sores or injuries. If neglected, these
can lead to severe infections of the flesh, bone infection, and deformities or
loss of the feet.

Figure
What is the future for a child with spina bifida?
This will depend first on how serious the defect is, next on
medical treatment and general care, and finally on special training and on
family and community support.

Figure
The higher up the back the defect is or the more severely the
spinal cord is affected, the worse the paralysis and other problems are likely
to be. If the head is already very swollen, the child’s chances are poor.
The costs will usually be great, even for a rich family. Surgery to drain the
liquid from the head is sometimes followed by infection. The operation may need
to be repeated several times. In spite of the best medical attention, at least 1
of every 4 or 5 children born with severe spina bifida dies in the first months
or years of life.
However, the child with a defect that is low down on the back
usually has less paralysis, and has a good chance of living a full and happy
life. With good family and community support, many children with spina
bifida go to school, learn to do many kinds of work, get married, and have
children.
Often these children are late in learning basic skills for
self-care (getting dressed, eating, going to the bathroom). This is partly
because of the disability. But it is also because their
parents often overprotect them and do everything for them. It is important
for parents to help these children to do more for themselves.
What are the chances that my child with spina bifida will
walk?
This depends on many factors. However, the higher up the defect
is on the spine, the more paralysis the child will probably have. The drawings
below show how likely it is for the child to walk, based on the level of the
defect. The shaded areas show the parts of the body affected by paralysis and
loss of feeling.
Figure
CARING FOR THE CHILD WITH SPINA BIFIDA

BEFORE SURGERY

AFTER SURGERY
Care of the defect. When there is a ‘bag of
nerves’ on the spine of a newborn baby, his chances of living are much
better if he has an operation within a few weeks. The surgery covers the defect
with muscle and skin. Without this operation there is a high risk of injury and
brain infection (meningitis); the child will probably not live very long.
For children who cannot get an operation, try to protect the bag
of nerves so that its thin covering is not injured or broken. (If it breaks,
meningitis can occur.)
One way to protect the bag is to make a ring or
‘donut’ of soft cloth or foam rubber (1), and to tie it so that it
surrounds the bag. Do not let the ring or clothing touch the bag.

Figure
Hydrocephalus. It is important to measure the distance
around the head of the child at birth, and every week or so afterward. If head
size increases faster than normal (see chart), or if you notice that the head
is swelling a lot, the child probably has hydrocephalus.
A surgical operation called a ‘shunt’ may need to be
done before the pressure of the liquid in the brain causes much damage. A tube
is run from a liquid-filled hollow in the brain into the entrance to the heart
or into the belly (abdominal cavity). This way the extra liquid is drained from
the brain.

SHUNT-BRAIN TO HEART
SHUNT-BRAIN TO BELLY
Not all children who have early signs of hydrocephalus need this
operation. If the head is not very swollen and stops increasing rapidly in size,
it may get better by itself.
CAUTION: ‘Shunts’ do not always give
good results. Even with surgery, 1 out of 5 children with hydrocephalus dies
before age 7, and more than half become mentally retarded. Others are
intelligent, however, and develop normally. Before deciding on the operation,
get advice from 2 or 3 specialists.
|
Note: We realize that, for many families,
the operations described here will not be possible. Except where free hospital
services are available, they are very costly.
Before deciding on surgery, there are several things to
consider:
· What will the
child’s future be like, if he lives? Is he likely to suffer greatly,
or might he have a chance to live a full and happy life, despite his
limitations?
· If the family spends much
money on operations, and then on daily care of the child, how will this affect
the health and well-being of the other children in the family?
In short, before deciding whether to operate, it is important to
consider carefully how this may affect the quality of life for both the child
and the family. |
Bladder and bowel management
A child with spina bifida usually does not develop the same
control of peeing (bladder control) and shitting (bowel control) as other
children do. The child may always dribble urine. Or, as she gets older, she may
continue to empty her bladder or bowels without warning, perhaps without even
knowing or feeling it. Standard methods of toilet training will not work. Do
not blame or scold her for her accidents.
|
WARNING: In some children with spina
bifida, the bladder does not empty completely. This is dangerous because if
urine stays in the bladder for a long time, bacteria will grow in it and this
can lead to infection of the bladder and kidneys. In children with spina bifida,
urinary infections are a frequent cause of death.

Figure
|
A mother can learn to feel how full the bladder is, and to tap
on it gently to see if this makes the baby pee. If not, she can regularly press
gently on the bladder to push out the urine.

Figure
Later, some children can learn to empty their bladders by
crying, rolling over, laughing, or sneezing. Others learn to do it by pressing
on the stomach, like this, although this can also be risky.

Figure
Some children may need to use a ‘catheter’ or rubber
tube to get the urine out. By age 5 they can often learn to
‘catheterize’ themselves.

Figure
Girls often need to empty the bladder regularly with a catheter,
and perhaps use diapers (nappies) to catch any urine that drips out in between.

Figure
For girls, a mirror helps in finding the urine hole.
As they grow older, boys are often able to use a
‘condom’ connected to a bag (1) that collects the urine.

Figure

Figure
Most children with spina bifida can be helped to take care of
both their bladder and bowel so that they stay relatively dry, clean, and
healthy. Then they can go to school and do things outside the home with greater
confidence. Therefore, it is extremely important that rehabilitation workers
and family members help the child work out a good bladder and bowel program.
|
IMPORTANT INFORMATION on urinary and bowel
problems and prevention and treatment of urinary infections is in
Chapter 25. Be sure to study this chapter! |
PREVENTION and correction of contractures
Some children with spina bifida tend to develop
contractures either because of muscle imbalance or, less often,
because of spasticity (abnormal muscle tightness). Contractures
most often develop in the feet, hips, and knees. Range-of-motion and
stretching exercises, as discussed in Chapter 42, can help prevent and correct
early contractures.
|
CAUTION: Only do stretching exercises where
there is stiffness or limited range of motion. When joints are floppy, do not
stretch them more where they already bend too much. For example: |
|
If the foot is stiff in this position,

Figure
|
do exercises to gradually bring the foot up.
Figure
|
But if the foot is floppy or already bends up more than normal,

Figure
|
avoid exercises that would stretch it even more.

Figure
|
Because children with spina bifida have stronger muscles for
bending than for straightening the hips, they tend to develop hip
contractures, like this child (1). Stretching exercises and lying on the
belly may help.
Figure
Also, make sure walking aids help correct rather than increase
the contractures.
This expensive metal ‘walker’ lets this child with
spina bifida ‘walk’ with hips bent. It can cause hip contractures and
make walking without aids less possible.
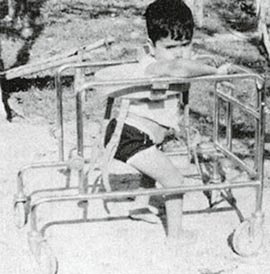
Figure
When the child is changed to parallel bars adjusted to the right
height, he walks more upright. This helps prevent contractures and increases the
possibility of walking without aids.

Figure
Sometimes a child stands with hips and knees bent, partly
because his feet bend up too much.
This can lead to hip and knee contractures.

Figure
Lightweight below-knee braces that hold the feet in a
more firm position may be all the child needs to stand straighter, walk better -
and prevent contractures.

Figure
|
Do not let the child get fat.
Because the legs and feet of a child with spina bifida are weak,
it is important that she does not get too heavy. Even for a child who does not
walk, moving will be easier if she is not fat. Encourage her to eat nutritious
foods, but to avoid a lot of sweets, fatty foods, and sweetened drinks. |
HELPING THE CHILD DEVELOP
Many children with spina bifida are paralyzed from the waist
down. In spite of their disability, it is important for them to develop their
bodies, their minds, and their social abilities as much as possible. Certain
‘adaptive aids’ can be used to help paralyzed children go through the
same stages of development as able-bodied children, at close to the same age.
(See the developmental chart)
For the child to progress through the early stages of
development, it is important that he can
|
SEE STRAIGHT AHEAD |
SIT WITH HIS HANDS FREE |
EXPLORE HIS SURROUNDINGS |
STAND WITH HIS HANDS FREE |
SIT, STAND, AND WALK |
|
NORMAL |
|
|
|
|
|
Figure
|
Figure
|

Figure
|

Figure
|
Figure
|
|
SPINA BIFIDA |
|
|
|
|
|

Figure
|

Figure
|

Figure
|
Figure
|

Figure
|
|
If she cannot get herself into a position where she can see what
is happening in front of her, lie her on a ‘wedge’ or fix a carton or
box so she can sit leaning back in it. |
You can make a seat from an old bucket or some other object, so
that she can sit and play. |
You can make a little cart that helps her to move. The cart can
have a handle so that another person can push it. |
Make a standing frame that holds her in a standing position.
Holding up the weight of her body on her legs will strengthen her bones, so they
will not break as easily. |
She can use a brace that holds her up, so that she can walk with
crutches. It helps if the brace has hip and knee hinges so that she can sit
down. |
When adapting aids for children with spina bifida, remember that
each child is different. Some children manage to walk without braces, perhaps
with the aid of parallel bars like these, and later crutches. Others will need
above-knee or below-knee braces (see Chapter 58). Other children will need
wheelchairs.

Figure
This child with spina bifida learned to walk using elbow
crutches adapted to form a walker. As his balance and control improved, the
supports on the crutches were gradually removed until he could walk with the
crutches alone.

Figure
Surgery and orthopedic corrections
To prevent or correct foot contractures in many children,
it may be necessary to straighten the feet in the same way as for club feet. So
that the contractures do not come back, the children will need to do exercises
and perhaps use simple plastic braces, at least at night.
For curving of the spine, if severe, some children need surgery
or a body brace.
For children with spina bifida who have one hip
dislocated, corrective surgery is sometimes helpful. But surgery generally
is not recommended for those children with both hips dislocated. Usually
they will walk just as well if the hips are left dislocated - and with fewer
complications and less suffering. (See “Hip Problems”)
|
CAUTION: Before any orthopedic surgery is
performed on a child with spina bifida, carefully evaluate the possibility she
has of walking and whether the surgery will really help her. |
PREVENTION of pressure sores and injuries
As a child who has no feeling in parts of his body grows older
and heavier, there is increasing danger that pressure sores (bed sores) will
form over bony areas that support his weight (mostly his butt or his feet). To
prevent this:
· Have the child
sleep and sit on a mattress or cushion that is soft (such as foam rubber),
and move or turn over often.
· Examine the child’s lower
body daily for early signs of irritation or sores. Check especially the hips,
knees, and feet.
· When he is a little older, the
child can learn to check his own body each day for sores.
DANGER: Whether the cause is spina bifida
or leprosy, children who walk but have no feeling in their feet run a high risk
of cuts, burns, sores, and serious infections on their feet. Teach them to
check their feet every day.

Figure
Also, be sure that sandals, shoes, and orthopedic braces fit
well and do not cause blisters or irritation.
This child with spina bifida cut her feet on broken glass.
Because the cuts did not hurt, they were neglected and became severely infected.
In time, the infection spread to the bones in both her feet and began to destroy
them. As a result, her feet are very deformed and she may lose them completely.

Figure
|
IMPORTANT INFORMATION on prevention and treatment
of pressure sores is in Chapter 24. Be sure to read it. Also see Chapter
26 on Leprosy for special footwear and ways to protect the feet. |
You will find other important information that relates to a
child with spina bifida in other chapters of this book, especially:
Chapter 23, “Spinal Cord
Injury”
Chapter 24, “Pressure Sores”
Chapter 25,
“Urine and Bowel Management”
Also refer to the chapters on contractures, club feet,
exercises, developmental delay, braces, wheelchairs, and special seating.

This child with spina bifida was
born to a village family too poor to afford surgery.

The PROJIMO team made her a
special seat with a bowl attached to a hole in the back to protect her
‘sack on the back’.

A child with spina bifida learns
to walk with the help of a homemade walker. (PROJIMO)
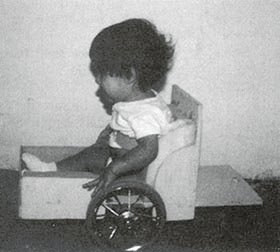
A one-year-old with spina bifida
in a mini wheel-chair made by disabled workers
(PROJIMO)
Chapter 23: Spinal Cord Injury
Spinal cord injury usually results from an
accident that breaks or severely damages the central nerve cord in
the neck or back: falls from trees or mules, automobile accidents, diving
accidents, bullet wounds, and other injuries. Spinal cord injury is more common
in adults and older children - and in many cultures it is twice as common in men
as in women.
The spinal cord is the line of
nerves that comes out of the brain and runs down the backbone. From
the cord, nerves go out to the whole body. Feeling and movement are controlled
by messages that travel back and forth to the brain through the spinal cord.
When the cord is damaged, feeling and movement in the body below the level of
the injury are lost or reduced.
Level of the injury
How much of the body is affected depends on the level of the
injury along the backbone. The higher the injury is, the greater the area of the
body that is affected.

Figure
Complete and incomplete injuries
When the spinal cord is damaged so completely that no nerve
messages get through, the injury is said to be ‘complete’. Feeling and
controlled movement below the level of the injury are completely and permanently
lost. If the injury is ‘incomplete’, some feeling and movement may
remain. Or feeling and controlled movement may return (partly or entirely)
little by little during several months. In incomplete injuries, one side may
have less feeling and movement than the other.
X-rays often do not show how complete a spinal cord injury is.
Sometimes the backbone may be badly broken, yet the spinal cord damage may be
minor. And sometimes (especially in children) the X-ray may show no damage to
the backbone, yet the spinal cord injury may be severe or complete. Often, only
time will tell how complete the injury is.
EARLY QUESTIONS THAT A SPINAL CORD INJURED CHILD AND FAMILY
MAY ASK
“Will my child always remain paralyzed?”
This will depend on how much the spinal cord has been damaged.
If paralysis below the level of the injury is not complete (for example, if the
child has some feeling and control of movement in her feet) there is a better
chance of some improvement.
Usually the biggest improvement occurs in the first months. The
more time goes by without improvement, the less likely it is that any major
improvement in feeling or movement will occur.
Occasionally surgery to release pressure on the spinal cord or
nerves, if done in the first hours or days following the injury, will bring back
some movement or feeling. But surgery done more than a month after the injury
almost never brings back any movement or feeling. Never agree to such surgery
unless at least 3 independent and highly respected neurosurgeons recommend it.
It is very unusual that a child who is paralyzed
by a broken neck is walking with a neck collar in 6 weeks.
Figure
After one year, the paralysis that remains is almost
certainly there to stay. As gently as you can, help both the child and parents
accept this fact. It is important that they learn to live with the paralysis
as best they can, and not wait for it to get better or go from clinic to clinic
in search of a cure.
|
It is best to be honest with the child and the family.
Explain the facts of the situation as clearly, truthfully, and kindly as
possible. |
“My child’s feet are beginning to move!” -
spasticity
Immediately after a spinal cord injury the paralyzed parts are
in ‘spinal shock’, and are loose or ‘floppy’. Later (within
a few days or weeks) the legs may begin to stiffen - especially when the hips or
back are straightened. Also, when moved or touched, a leg may begin to
‘jump’ (a rapid series of jerks, called ‘clonus’).
This stiffening and jerking is an automatic reflex called
‘spasticity’. It is not controlled by the child’s mind, and often
happens where spinal cord damage is complete. It is not a sign that the
child has begun to feel where he is touched or is recovering control of
movement.
|
CAUTION: Sudden jumping or stiffening of
the legs when moved or touched does not mean feeling or controlled movement is
returning. This is a spastic reflex.

Figure
|
Some children with spinal cord injury develop spasticity; others
do not.
|
|
If the spinal cord injury is above the level of the top edge of
the hipbone (above the 2nd lumbar vertebra) spasticity is very likely.
SPASTIC |
|
level between 1st and 2nd lumbar vertebrae |

Figure
|
|
|
|
FLOPPY
If the injury is below this level, paralysis is usually floppy
(no muscle spasms). |
Severe spasticity often makes moving and control more difficult.
However, the child may learn to use both the reflex jerks and spastic stiffness
to help her do things. For example,
When the child wants to lift her foot, she hits her thigh,
triggering the jerks that lift the leg.

Figure
In lower back injuries, the spasticity or stiffness of the legs
may actually help the child stand for transfers.

Figure
“Will my child be able to walk?”
This will depend mostly on how high or low in the back the
injury is. The lower the injury, the better the chance of walking. A person with
complete spinal cord injury in the neck has no chance of walking. She will need
a wheelchair.
If the child’s injury is in the lower back and if his arms
are strong and he is not too fat, there is a chance he may learn to walk with
crutches and braces. But he will probably still need a wheelchair to go long
distances.
Many spinal cord injured persons prefer a wheelchair to walking
with braces and crutches.

Figure
However, it is best not to place too much importance on learning
to walk. Many children who do learn to walk find it so slow and tiring that they
prefer using a wheelchair.
It probably makes sense to give most paraplegic children a
chance to try walking. However, do not make the child feel guilty if he prefers
a wheelchair. Let the child decide what is the easiest way for him to move
about.
For independent living, other skills are more important than
walking, and the family and child should place greater importance on these:
skills like dressing, bathing, getting into and out of bed, and toileting.
Self-care in toileting is especially important - and is more difficult because
of the child’s lack of bladder and bowel control.

A child who is paraplegic learns
to walk with a plywood parapodium made by village rehabilitations workers.
(PROJIMO)
“What are the hopes for my child’s
future?”
The chances of a paraplegic’s leading a fairly normal life
are good - provided that you:
1. avoid 3 big medical risks:
· skin
problems (pressure sores)
· urinary
infections
· contractures (shortening of
muscles, causing deformities)
(Contractures are not a danger to life but can
make moving about and doing things much more
difficult.)
2. help the child to become more
self-reliant:
· home
training and encouragement to master basic self-help skills such as moving
about, dressing, and toileting
· education: learning of skills
that make keeping a household, helping other people, and earning a living more
possible
It is more difficult for quadriplegic persons to lead a normal
life because they are more dependent on physical assistance. However, in some
countries many paraplegics and quadriplegics manage to lead full, rich lives,
earn their own living, get married, and play an important role in the community.
With effort and organization, the same possibilities can exist in all countries.
“Can anything be done about loss of bladder and bowel
control?”
Yes. Although normal control rarely returns completely, the
spinal cord injured child often can learn to be independent in his toilet, and
to stay clean and dry (except for occasional accidents). Often he will need a
special urine collecting device, will learn to use a catheter, and will learn to
bring down a bowel movement with a finger or suppository. Management of bladder
and bowels are discussed in Chapter 25.
|
VERY IMPORTANT INFORMATION ON URINE AND BOWEL CONTROL IS IN
CHAPTER 25. BE SURE TO READ THIS CHAPTER! |
“What about marriage, sex, and having
children?”
Figure
Many spinal cord injured persons marry and have loving, sexual
relationships. Women with spinal cord injuries can become pregnant and have
normal babies. Men may or may not be able to get a hard penis or ejaculate
(release sperm). Paraplegic and quadriplegic men whose injuries are incomplete
are more likely to have children. Some couples where the husband cannot release
sperm decide to adopt children. Whether or not they can have children, male and
female spinal cord injured persons often enjoy loving sexual relationships.
Especially for young men, fear of the loss of sexual ability is
often one of the most fearful and depressing aspects of spinal cord injury.
Honest, open discussion about this, and the possibilities that do exist, with a
more experienced spinal cord injured person may help greatly. There is a good
discussion of this in Spinal Cord Injury Home Care Manual.
See reference.
HELPING THE CHILD AND FAMILY ADJUST
Spinal cord injury, especially in the child, brings many of the
same problems as does spina bifida. Also many aspects of rehabilitation are
similar. (We suggest you read Chapter 22 on spina bifida to get additional ideas
for the rehabilitation of young children with spinal cord
injuries.)
Perhaps the biggest difference from spina bifida is that spinal
cord injury begins later. One day the child is physically active and able, the
next he is suddenly paralyzed and (at first) unable to do much for himself. He
has lost all feeling and control in part of his body; it is like a dead weight.
This is very hard for the child - and family - to accept. Both
have an enormous fear and uncertainty about the future. The child may become
deeply depressed, or angry and uncooperative. He may refuse even to sit in a
wheelchair because this means accepting not being able to walk.
There are no easy answers to the child’s fear and
depression, but here are some suggestions families have found helpful.
· Recognize that the
child’s fear, depression, and anger are natural responses and that with
love, understanding and encouragement, he will little by little overcome them.
· Be honest to the child
about her disability. Do not tell her, “We will find a
cure for you,” or, “Soon you will get well and be able to walk
again.” Very probably this is not true, and telling the child such things
only makes it more difficult for the child to accept her disability and to begin
shaping a new life. Also, as the promised ‘cure’ fails to happen, the
child becomes more uncertain, distrustful, and afraid. In the end, it will be
much easier for her if you gently tell the truth. Here is one example.’

Figure
· Provide opportunities to
keep the child’s mind active: playing, working, exploring, learning
through stories, games, and studies. But at the same time respect and be
supportive of the child when he feels sad and frightened. Let him cry,
comfort him when he does, but do not tell him not to cry. Crying helps relieve
fear and tension.
· Start the child with
exercises, activities, and relearning to use her hands and body as soon as
possible. Start with what the child can do, and build on that.
· Try to have the child
watch, talk with, and get to know other persons with spinal cord injury (or
children with spina bifida), especially those who are living full and happy
lives.
· Invite the child’s
friends to come visit her, play with her, and let her know that they are eager
for the day she will be back in school.
· Encourage the child to do
as much for herself as possible. Let her do anything she can do for herself
- even if it takes longer.
|
Help in ways that let the child do more for herself.
|
· As much as possible, avoid
‘tranquilizers’ or other strong medicines. The child needs an alert
mind and an ability to move actively all day.
Look for ways to help spinal cord injured persons learn skills
and play a useful, helpful role. Here 2 young, spinal cord injured persons in
PROJIMO examine a disabled child, and give recommendations to the family, using
an early draft of this book.

Figure
HOW TO PREVENT MORE SEVERE SPINAL CORD INJURY IN CASE OF
ACCIDENT
When a person has just had an accident that may have injured the
spinal cord, great care must be taken to prevent further damage.
After an accident, there may be spinal cord injury if:
· the person is
unconscious, or
· the person cannot move,
cannot feel, or has numbness in his legs or hands.
If you think the spinal cord might be injured:
· Do not move the
person until a health worker with a large board or stretcher arrives.
Especially avoid bending the person’s neck and back.
· Lift the person without
bending him, onto a board or stiff stretcher. (A stiff rack is better than a
soft stretcher. Make one out of poles from trees or whatever is available.) Make
ties of strips of clothing, or whatever you can.
Figure
· Tie him down
firmly and stabilize his head.
· Carry the person to a medical
center or hospital. Try not to bounce or jiggle him.
HOW TO LIFT A SEVERELY INJURED PERSON ONTO A
STRETCHER
from Where There Is No Doctor
|
1.

Figure
|
2.

Figure
Make sure that the head and neck do not bend. |
|
With great care, lift the injured person without bending him
anywhere. |
Have another person put the stretcher in place. |
|
3.
Figure
|
4.

Figure
|
|
With the help of everyone, place the injured person carefully on
the stretcher. |
If the neck is injured or broken, put bags of sand or tightly
folded clothing on each side of the head to keep it from moving. |
Common secondary problems in children with spinal cord
injury
(1) Leg bones do not grow as fast, become thin and weak, and can
break easily, especially if the child does not bear weight on them.
(2) sudden high blood pressure with pounding headache
(dysreflexia) due to irritation in non-feeling parts (quadriplegics only)
(3) periods of depression, anger, and difficulty accepting
disability
(4) curving or ‘hunching’ of spine
(5) Child suffers greatly in hot weather because body loses
ability to control its temperature.
(6) urinary infections (may involve kidneys and cause death)
(7) pressure sores (bed sores) in-body areas where feeling has
been lost (See Chapter 24.)
(8) rash or sores between legs due to loss of urine and bowel
control
(9) increased risk of pneumonia in quadriplegics, due to weak
breathing muscles
(10) pressure sores caused by long-leg brace
(11) spasticity causes legs to straighten and pull together and
feet to ‘tiptoe’ stiffly
(12) contractures - especially of
- elbows and hands (in quadriplegics)
- hips
(bend up and pull together)
- tiptoe and club foot deformities - especially
in small children
(13) burns or other injury where body cannot feel
Figure
To prevent or reduce the harmful effects of these problems,
special precautions need to be taken early and continued throughout life.
EARLY CARE FOR THE SPINAL CORD INJURED PERSON
Early care following spinal cord injury is best done in a
hospital, especially if the child is likely to get good nursing care.
Family members should stay with the child in the hospital to make sure the child
is kept clean and turned regularly, so that bed sores and pneumonia are avoided.
(Busy hospital staff with little experience treating spinal cord injuries
sometimes let severe bed sores develop - which may threaten the child’s
life.)
|
CAUTION: During the first 6 weeks, or until
any breaks in the bone have healed, take great care when turning the child so
that the angle of his back, neck, and head does not change. Use the same
methods and precautions used in lifting a newly injured person onto a stretcher.
When the neck or back has healed, the child can start lying on his stomach, at
first for 10 minutes and then longer if there are no problems. |
Surgery of the spine may or may not be necessary. After
surgery, the person must lie very still for at least 6 weeks. The main purpose
of surgery is to prevent more damage - not to cure the paralysis. The damage
already done to the spinal cord cannot be corrected with surgery or
medicine.
Preventing pressure sores (bed sores)
When feeling has been lost, pressure sores can easily form on
the skin over bony areas - especially on the hips and butt. The biggest risk of
sores is in the first weeks after the injury. This is because the child must
stay very still, and has not yet learned to move or turn over his body.
Prevention of pressure sores is extremely important, and needs understanding and
continuous care, both by the child and those caring for him.
|
BE SURE TO READ CHAPTER 24 ON PREVENTION AND TREATMENT OF
PRESSURE SORES. |
Summary: early prevention of pressure sores (For details,
see Chapter 24.)
· Lie on a soft
mattress or thick, firm, foam rubber pad.
· Place pillows and pads to keep
pressure off bony areas.
· Change position (turn over
from front to back and side to side) every 2 to 3 hours. To avoid pressure
sores, lying on the belly is the best position.
· Keep skin and bedclothes clean
and dry.
· Eat good food rich in
vitamins, iron, and protein.
· Move and exercise a lot to
promote good flow of the blood.
· Check skin daily for earliest
signs of pressure sores - and keep all pressure off beginning sores until the
skin is healthy again.

Figure
Avoiding contractures
In the first weeks following a spinal cord injury, when the
child is in a lying position, joint contractures (muscles shortening) can easily
develop, especially in the feet and elbows. Pillows and pads should be placed to
keep the feet supported, the elbows straight, and the hands in a good position.
Gentle range-of-motion exercises of the feet, hands, and arms should begin as
early as possible, taking care not to move the back until the injury is healed.
PHYSICAL THERAPY FOLLOWING SPINAL CORD INJURY
ASSISTED BREATHING AND COUGHING
Persons with spinal cord injury in the neck or upper back often
have part of their breathing muscles paralyzed. Slowly the remaining muscles
become stronger and breathing improves. But breathing often stays weak. The
person may not be able to cough well and can more easily get pneumonia.
To help the person cough, place hands as shown below. Ask him to
cough, and as he does, push firmly inward on the chest. Be careful not to move
the backbone.
TWO-PERSON ASSISTED COUGH
Do this several times a day when the person has a cold, and more
often if the person develops more trouble breathing or seems to have a lot of
mucus in his lungs or throat.

Figure
ONE-PERSON ASSISTED COUGH
To help the child breathe deep and to stimulate the breathing
muscles, press lightly here while the child tries to breathe deeply in and out.
Do this for a few minutes, several times a day.

Figure
If the person has a lot of mucus in her lungs, it also helps to
lie her down, like this (1), and pat her back briskly. This helps loosen the
mucus so that it can be coughed out. Be sure she drinks lots of water to help
loosen the mucus.

Figure
MOVEMENT AND EXERCISE
Do range-of-motion exercises for about 10 minutes for each arm
and leg. In the first weeks, do the exercises twice a day. Later, once a day may
be enough. If any signs of contracture develop, spend more time and effort on
those parts of the body. From the start, exercises should be both
passive (someone else moves the child’s body parts) and whenever
possible, active (the child does it himself).
Range-of-motion exercises should begin with great care
the day after the spine is injured (see Chapter 42). The exercises will help to
improve the flow of blood (which reduces the chance of bed sores), to prevent
contractures, and to build the strength of the muscles that still work.
Range-of-motion exercises should be continued throughout life, when
possible as a part of day-to-day activity.
|
CAUTIONS:
· Until any breaks or
tears in the spine have healed (6 weeks or more) exercise must be very gentle
and limited, with smooth motions and no jerking.
¨ Especially at
first, take great care that exercises do not move the position of the back and
neck. Start with feet, ankles, hands, wrists, and elbows.
¨ If exercises trigger severe
muscle spasms or jerking, do not do them until the break is healed.
· Do not use force in trying to
get the full range of motion, as joints can easily be damaged.
· For quadriplegics often it is
better to stretch the fingers only when the wrist is bent down like this,

Figure
but not when it is bent back like this.

Figure
This way enough contracture is left to be useful for taking hold
of things. Although the fingers lack movement by muscles, they close around an
object when the wrist is bent back.
If possible, get instructions from an experienced
physical therapist.
· Try to keep the full range of
motion of all parts of the body. But work most with those joints that are
likely to develop contractures, especially:
¨ paralyzed parts
that tend to hang in one position, such as the feet,

Figure
Prevent this through exercises and by supporting
feet.
¨ or, joints that are kept
straight or bent by spasticity or by muscle imbalance. For
example:
In quadriplegia the muscles that
straighten the elbow (1) are usually paralyzed, while the muscles that bend the
elbow (2) stay fairly strong. These muscles keep the elbow bent, and in time
they shorten so that the arm can no longer straighten
fully.

Figure
It is important that the arms can
straighten until they bend backward a little (3) - which is the only way he can
lift himself with his arms.
Figure
For this reason, straight arm
positioning and early range-of-motion exercises for the elbow are essential.
While he is still kept lying down, teach him to straighten his elbows by turning
his hands up and then lifting his arms (4).

Figure
|
MAINTAINING HEALTHY POSITIONS
The position that the body is in during the day and night is
also important to prevent contractures.
Contractures that cause ‘tiptoeing’ of the feet
can develop easily, especially when there is spasticity. Keep the feet in a
supported position as much of the time as possible:
Teach the child to make sure his feet are in a good
position.
Figure
Even for the child who may never walk, maintaining the feet in a
flat position makes moving from chair to bed, toilet or bath easier.
|
CAUTION: A support like this works well with
floppy feet, but may trigger spasticity or jerking of the feet. Position them
slowly. |
Another common problem for children with spasticity is that the
knees pull together and in time contractures prevent the legs from separating.
To prevent this, when the child lies on her side she should learn to

Figure
A common problem with wheelchair users is that they slump
forward. In time this can deform the spine.
In a wheelchair with a straight-up back a person with spinal
cord injury slumps like this in order to balance.

LESS APPROPRIATE
A chair can be designed (or adapted) so that it tilts back. This
provides balance for a better position.

MORE APPROPRIATE
A special cushion also helps keep the butt from sliding forward
(and helps prevent pressure sores).
Figure
If possible, make cushion out of ‘micropore’ foam
rubber (foam with very tiny bubbles). Rubber-coated coconut fiber also works
well.
For more suggestions for wheelchair adaptations, see Chapters 64
and 65.
EARLY PHYSICAL RE-EDUCATION
The goal for a spinal cord injured person is to become as
independent as possible in doing what he or she wants and needs to do. But even
before the skills of daily living are relearned, the person needs to learn to
protect the body where functions that used to be automatic have been lost.
The protective functions that may be lost or changed include:
1. Adjustment of blood pressure to changes in body
position.
2. Feeling (including pain) that protects from injuries (such as
bed sores).
3. Sense of body position and ability to keep balance.
4.
Muscle strength and coordination.
5. Control of body temperature - especially
keeping cool in hot weather.
1. A sudden drop of blood pressure in the brain when the
person rises from lying to sitting, or sitting to standing, can cause
dizziness or fainting. This is a common problem in spinal cord injury because
the blood pressure adjustment mechanism is partly lost. Little by little the
body can be helped to re-adapt, but precautions are needed. (These same
precautions are for anyone who has been kept lying down a long time.)
Before beginning to sit, raise the head of the bed-a little more
and a little longer each day.

Figure
Start like this for 15 minutes.
In a week or 2 build up to this for 3 hours.

Figure
If the person begins to get dizzy or faint when sitting, tilt
him back and lift his feet.

Figure
Lifting exercises help the body relearn to adjust blood pressure
- and also prevent bed sores and strengthen arms.

Figure
Before beginning to stand, make a standing board, and strap the
child to it. Start at a low angle, and stand the board up more-and longer - each
day

Figure
2. The loss of feeling in parts of the body can lead
to pressure sores and other injuries, such as burns and cuts. This is
because the body no longer feels pain and does not warn the child to change
position or move away from danger.
It is important that the child learn to protect himself by
changing positions often and avoiding injuries. This includes:
· learning to roll
over

Figure
· turning at least
every 4 hours when lying or sleeping
·
lifting from sitting every 15 minutes
·
examining the whole body every day for signs of injuries or sores
Figure
· washing
daily

Figure
· learning to
protect himself from burns and other injuries. For example,
DO NOT sit on or touch hot
objects (or roads).

DO NOT sit, lie or sleep near an
open fire.
Keeping clean is very important for persons with reduced
feeling, especially if they lack bladder and bowel control. Take care to bathe
daily. Wash and dry the genitals, the butt, and between the legs as soon as
possible each time they get wet or dirty.
If redness, diaper rash, or sores develop, wash more
often and keep the sore area dry. Keep the legs spread open and
exposed to the air. When they must be covered, use soft absorbent cotton cloth.
Putting a little vinegar in the rinse water after bathing the child, and after
washing diapers and underclothes, helps prevent skin rash and
infection.
For treatment of specific skin infections (fungus, yeast,
bacteria) consult a health worker or a medical book (like Where There Is
No Doctor, see Chapter 15).
3. Loss of ability to sense what position the body is in
affects a person’s sense of balance. So does loss of muscle control. The
child needs to develop new ways to sense the position of his body and keep his
balance. Start with the child sitting on a bench, if possible, in front of a
mirror.
Help the child progress through these stages:
· both hands on
bench
· both hands on knees
· lift one arm sideways, forward, and back
· After doing this in front of a mirror, have him do it
without the mirror.
· As the child gains
better balance, start doing different movements with first one and then both
arms, such as lifting weights or playing ball.

Figure

Figure
|
Note: Some children may have so much difficulty
with balance that they may have to start in a wheelchair or a chair with high
back and arm supports. |
4. Muscle re-education All muscles that still work need
to be as strong as possible to make up for those that are paralyzed. Most
important are muscles around the shoulders, arms, and stomach.
Weight-lifting is a good exercise to strengthen shoulders.

Figure
Look for ways to make the exercises useful and fun.

Figure
5. Temperature control Normally, when a person feels hot,
he sweats and the blood vessels beneath the skin swell. This automatic cooling
system is partly lost in persons with high spinal cord injury. In hot weather,
they may get high fever or can even die of heat stroke.
For this reason they must learn (and be allowed) to rest quietly
in the shade, in the coolest place possible, during the hottest part of the day

Figure
Children with spinal cord injury can learn to paddle around very
well in old tire tubes. They love it, and it is excellent arm and shoulder
exercise. However, it is very important that someone watches them.
If he can spend part of the hottest hours of the day in a
shaded, shallow pool or pond, this is ideal.

Figure
For hot weather, a plastic spray bottle works very well for
cooling the body.

Figure
|
TAKE CARE also to protect against cold.
Body temperature can also drop too low. |
DYSREFLEXIA (Sudden high blood pressure with pounding
headaches)
Persons with quadriplegia or very high paraplegia run the risk
of ‘dysreflexia’ - or sudden, dangerous increase in blood pressure
with severe pounding headaches.
Dysreflexia is the body’s reaction to something that would
normally cause pain or irritation, but which the person does not feel because of
the spinal cord injury.
|
COMMON CAUSES OF DYSREFLEXIA |
SIGNS (OF DYSREFLEXIA) |
|
· bladder problems -
especially when the bladder is too full, infected, or has bladder stones (This
is by far the most common cause.)
· stretching of the
bowel-from constipation, with a big ball of hard shit, or from finger
pressure to remove the shit
· pressure areas or
sores-or even irritation from lying on a small object without knowing it
· burns
· spasm of the
womb - especially just before or in the first days of a woman’s
monthly period, or during childbirth |
· severe pounding
headache
· sweating of the head
· stuffy nose
·
reddish skin patches on face and neck
· goose
pimples above the level of injury
· slow
pulse
· high blood pressure (up to 240/150)

Figure
|
|
Dysreflexia is a medical emergency. The high blood
pressure could cause fits or deadly bleeding inside the brain. |
What to do
Act quickly to remove the cause and lower the blood
pressure.
· Quickly lower the
blood pressure in the head.
¨ If
lying, sit up; stay sitting until the signs go away.
¨ Change position, drop feet down, loosen belt or
straps, remove tight stockings.
· Look for the cause
of dysreflexia, and remove it if possible.
¨
Bladder. Feel the lower belly to see if the bladder is full. If a
catheter is in place, check for bends or kinks and straighten them to let
urine flow. If the catheter is stopped up, open it by injecting 30 cc. of boiled
and cooled water (or sterile saline solution) into the catheter. Or take the
catheter out. If a catheter is not in place and the person cannot pee,
put in a catheter and empty the bladder.
¨ If a urinary infection
appears to be the cause, inject an anesthetic solution into the bladder through
a catheter. Use 10 cc. 1% lidocaine in 20 cc. of boiled water. Clamp the
catheter for 20 minutes and then release. Treat the infection.
¨ Bowel. If the bladder
does not seem to be the cause, check for a full bowel. How long has it been
since the last bowel movement (shit)? Put some lidocaine
(Xylocaine) jelly on your finger and check if the bowel is packed
with hard shit. If it is, put in more lidocaine jelly. Wait 15 minutes, or until
the headache becomes less. Then gently remove the shit with your finger.
¨ Pressure. Change the
child’s position in order to relieve pressure over bony areas. (Sometimes
just staying in the same position too long can bring on
dysreflexia.)
· If the signs do
not go away, get medical help as fast as possible.
· If the child has frequent or
severe periods of dysreflexia, or you cannot find the cause, try to have him
seen by a specialist on spinal cord injury, and possibly a ‘urologist’
(specialist of the urine system).
|
Suggestion: For quadriplegics in villages, it is
wise to have injectable 1% lidocaine (Xylocaine) and lidocaine gel available for
dysreflexia emergencies. |
Self-care
With help and encouragement of family, friends and
rehabilitation workers, the child with spinal cord injury can
learn to become as independent as possible in meeting his basic needs: moving
about, eating, bathing, dressing, toileting, and in time other skills for
daily living.
Progress toward self-care, especially at first, may be slow and
frustrating. The child will need a lot of understanding and encouragement.
Persons with low spinal cord injury will find it easier to relearn self-care
skills than those with higher injuries who have less use of their hands and
arms. Quadriplegics usually will remain at least partly dependent on others for
some of their daily activities. To make activities easier both for themselves
and their helper, it is important that they avoid getting fat.
Useful methods and techniques have been worked out for helping
relearn basic skills. We cannot describe many of these in detail. However, much
depends on determination, imagination, and common sense. Start with first things
first - like rolling over and sitting up in bed.
A few simple aids can often help a person become more
independent. For example,
(1) loose-fitting clothing with elastic or easy-to-do fastener
(for example, a brassiere that fastens in front)
(2) convertible wheelchair toilet
(3) a rope with a loop for pulling to sit
(4) homemade bed, the same height as wheelchair and toilet
(5) padding to prevent sores
Figure
When hands are affected, devices like these (or others that you
can invent) make relearning to eat and write easier.

Figure
‘Velcro’ sticks-to-itself tape makes it possible for
the person to put on aids by herself.
metal tube soldered to a piece
that fits into hand band
Suggestions for getting in and out of wheelchairs and learning
to walk with crutches are included in Chapter 43.
KEEPING ACTIVE

Figure
Many of the ‘complications’ of spinal cord injury
happen because the person spends a lot of time just lying and sitting. To keep
healthy, the body needs to keep active. Lack of movement and activity causes
poor flow of the blood. This can lead to pressure sores, swollen feet, painful
or dangerous blood clots (thrombosis) especially in the legs, increasing
weakness of bones (osteoporosis) with risk of breaking them, stones in the
bladder or kidneys, increased risk of urinary infections, and general physical
weakness and poor health.
It is important - both for the body and mind - that spinal cord
injured persons keep physically active. Let your child do as much for herself as
she can: pushing her own wheelchair, bathing, transferring, washing clothes,
cleaning house, and helping with work.

Figure
Active games and sports can also be encouraged. Swimming,
basketball, and archery can be done well with upper body use only.
Quadriplegics can become skillful with bow and arrow by using a straight-arm
splint and a special hook, fastened to the hand, to pull the string.

Figure

Figure
(Note: Archery may also help correct spinal
curve. The arm that pulls the string should be on the side with bulge in the
back.)
To keep leg bones growing well and to prevent them from becoming
weak and breaking easily, even children who may always be wheelchair riders
should stand for a while every day. Standing also helps the child’s bowels
move more often.
This standing frame was invented by a paraplegic youth and his
father. The boy uses the spasticity in his legs to stand. When the muscles tire
he hangs and sits on the padded poles.
This can be done by strapping the child to a ‘standing
board’ (1) or by making some kind of a standing frame.
Figure
Figure
This design for a standing wheel-bed allows a spinal cord
injured child with pressure sores on her butt to actively move about. The child
can adjust it while on it, from a flat-lying position to a near-standing
position. It can be made out of wood or metal.

Figure

Figure
Spinal cord injured persons as leaders
Spinal cord injured persons in various countries are now taking
the lead in making new lives for themselves and in getting their communities to
recognize their abilities. Examples of 2 programs run primarily by spinal cord
injured persons are included in Chapter 55. These are the Organization of
Disabled Revolutionaries in Nicaragua and the Centre for the Rehabilitation of
the Paralysed in Bangladesh. Members of these and many similar organizations
would be happy to share ideas and suggestions with any group of disabled persons
interested in organizing their own program or shop.
OTHER PARTS OF THIS BOOK WITH INFORMATION USEFUL FOR SPINAL
CORD INJURY
|
IMPORTANT: In addition to this chapter,
some essential information for spinal cord injury is in other parts of this
book, especially Chapter 24, “Pressure Sores,” and Chapter
25, “Urine and Bowel Management.” These chapters are a
continuation of information on spinal cord injury. We have put them in separate
chapters because the information they cover is also essential for other
disabilities. |
Chapters marked with a star (*) are essential for basic care
of spinal cord injury.
* Chapter 24 Pressure Sores
* Chapter 25 Urine and Bowel Management (includes
urinary infections)
Chapter 26 Leprosy (especially advice for care of hands
and feet without feeling)
Chapter 36 Feeding, especially aids for feeding
Chapter 37 Dressing
Chapter 38 Toilet Training, especially aids
Chapter 39 Bathing
* Chapter 42 Range-of-motion and Other Exercises
* Chapter 43 Crutch Use, Cane Use, and Wheelchair
Transfers
Chapter 51 Adapting Home and Community to Needs of the
Disabled
Chapter 52 Growing Up, Social Adjustment, Love, Sex, Role
in Family and Community
Chapter 55 Example 3, Centre for the Rehabilitation of
the Paralysed, and Example 4, Organization of Disabled Revolutionaries
Chapter 58 Braces
Chapter 63 Walking Aids
Chapters 64, 65, 66 Wheelchairs
For other references to spinal cord injury, see the INDEX, and
the books and reference material.
|
THE STORY OF J�SICA
J�sica is a little girl who was paralyzed because of an
unnecessary injection she received when she was 3 days old. Her mother does not
know why or with what she was injected. This is the story of her rehabilitation
at PROJIMO.
The injection resulted in an infection that reached her spine,
and permanently paralyzed her legs.

Figure
Misuse of medicines and especially injections is a common and
preventable cause of disability. See Chapter 3.
J�sica’s feet became clubbed. When she tried to stand, she
developed large, infected pressure sores on her knees and feet.

Figure
When J�sica first came to PROJIMO at age 4, the village team
first treated the infected sores. Then they began to cast her feet to gradually
straighten them (see Chapter 60).

Figure
They left ‘windows’ in the casts to keep treating the
sores.

Figure
Little by little the sores healed and J�sica’s feet
straightened. Here one of the workers changes her cast.

Figure
J�sica also lacks normal bowel and bladder control. From the
uncontrolled loss of urine, she developed pressure sores in her genital area.
Vania, an 8-year-old paraplegic girl, helped treat J�sica’s sores. She also
assisted J�sica with a ‘bowel program’, which helps her
‘time’ her bowel movements. This makes daily activities and going to
school much easier.

Vania treats the pressure sore on
J�sica’s foot.

Here Vania cleans and dresses
sores on J�sica’s genital area.

When her feet were straighter,
the village workers made above-knee braces for her and a simple wood walker. In
a few weeks J�sica was walking.

With practice J�sica was able to
walk with crutches - and finally with only her braces.
J�sica now goes to school in the village. Seeing disabled
persons at PROJIMO who were happy, active, and accepted in the community has
given J�sica a more hopeful, confident, and adventurous outlook on life. |

Mari, who is paraplegic, is one
of the leaders of the PROJIMO team. Here she works on a cast for making a
plastic brace. See her story.

Victor, a young doctor, became
quadriplegic in a traffic accident. He could do nothing for himself when he came
to PROJIMO. The village workers helped him gain strength and develop many
skills. Soon he became a member of the PROJIMO team and became the village
doctor.

This pressure sore, at the base
of the spine in a young man with quadriplegia, was present for 2 years. It was
15 cm across under the skin, and had completely destroyed the lower part of his
spine.

Village workers at PROJIMO clean
and dress the pressure sore.

Here one of the workers packs the
sore with a paste of sugar and honey. With this treatment 2 times each day, the
sore stayed clean and free of infection, and healed rapidly (in about 6
months).
Chapter 24: Pressure Sores
WHAT ARE THEY?
Pressure sores, or ‘bed sores’, are sores that form
over bony parts of the body when a person lies or sits on that part of the body
for too long without moving. Where the skin is pressed against the bed or chair,
the blood vessels are squeezed shut so that the blood cannot bring air to the
skin and flesh. If too much time passes without moving or rolling over, the skin
and flesh in that spot can be injured or die. First a red or dark patch appears.
And if the pressure continues, an open sore can form. The sore may start on the
skin and work in. Or it may start in deep near the bone and gradually work its
way to the surface.

This is a common pressure sore
point - over the top of the thigh bone
Who is likely to get pressure sores?
When a normal healthy person lies or sits in one position for a
long time, it begins to feel uncomfortable, or to hurt. So she moves or rolls
over, and pressure sores are avoided. People most likely to get pressure sores
are:
1. persons who are so ill, weak, or disabled that
they cannot roll over by themselves. This includes persons severely
disabled from polio, brain damage, advanced muscular dystrophy,
or a bad injury.
2. persons who have no feeling in parts of their body,
who do not feel the warnings of pain or discomfort when their body is being
damaged. This includes persons with spinal cord injury, spina bifida, and
leprosy.
|
WARNING: Because persons with spinal cord injury are
at first unable to turn over, and also have lost the ability to feel in parts of
their bodies, they are at very high risk for pressure sores. |
3. persons who have a plaster cast on an arm or leg (to
correct a contracture or to heal a broken bone), when the plaster
presses over a bony spot. At first the pressure will hurt and the child may cry
or complain. But in time the spot will grow numb and the child will stop
complaining - although a sore may be forming.
The risk is greater when using casts on children who have no
feeling in their feet. On these children, even a corrective shoe or brace can
easily cause a pressure sore - unless great care is taken.
|
Casts to straighten contractures and clubbed feet must be very
well padded over bony places to prevent pressure sores.

Figure
|
Where are pressure sores most likely to form?
They can form over any bony area. The places where they form
most often are shown in the pictures.
The points of highest risk, all on the hips, are marked in
CAPITAL LETTERS.

Figure

Figure

Figure
How dangerous are they?
Pressure sores, if not very carefully
cared for, can become large and deep. Because they contain dead skin and flesh,
they easily become infected. If a sore reaches the bone, which it
often does, the bone can also become infected. Bone infections are often very
hard (and costly) to cure, may last for years, and may keep coming back, even
after the original pressure sore has healed. (See “Bone Infections,”
Chapter 19.) Bone infections can lead to severe disabling deformities.
Infections in deep pressure sores often get into the blood and
affect the whole body, causing fever and general illness. This can lead to
death. In fact, pressure sores are one of the main causes of death in persons
with spinal cord injury.

These pressure sores in a
15-year-old girl who is quadriplegic were treated with honey and sugar and
healed in 2 months. PROJIMO
In persons with high spinal cord injuries (quadriplegia) the
irritation from pressure sores can also bring about sudden severe headaches and
high blood pressure (dysreflexia), which can also cause death.
How common are pressure sores?
In persons who have lost feeling in parts of their body,
pressure sores are very common. Most spinal cord injured persons in rich
countries, and nearly all in poor countries, develop pressure sores. Often the
sores start in hospitals shortly after the back injury, due to inadequate
nursing care. Therefore, it is important that families of spinal cord
injured persons, and the persons themselves, learn as early as possible about
the prevention and early treatment of pressure sores, and take all the needed
steps.
PREVENTION OF PRESSURE SORES
|
It is important that both the child and family learn about
the risk of pressure sores and how to prevent them. |
· Avoid staying in the same
position for very long. When lying down, turn from side to side or
front to back at least every 2 hours (or up to 4 hours if padding and cushioning
are excellent). When sitting, lift body up and change position every 10
or 15 minutes.
· Use thick, soft
padding, pillows, or other forms of cushion arranged so as to protect bony
areas of the body.
· Use soft, clean, dry bed
sheets. Try to avoid wrinkles. Change bedding or clothing every day and each
time the bedding gets wet or dirtied. A person who stays wet gets pressure
sores - especially if it is from urine.
· Bathe the child daily.
Dry the skin well by patting, not rubbing. It is probably best not to use body
creams or oils, or talc, except on the hands and feet to prevent cracking, as
these soften the skin and make it weaker. Never use heat-producing
oils, lotions, or alcohol.
· Examine the whole body
carefully every day, checking especially those areas where sores are most likely
to occur. If any redness or darkness is present, take added care to prevent all
pressure over this area until the skin returns to normal.
· Good nutrition is
important for preventing pressure sores. Be sure the child gets enough to eat
(but do not let her get fat). Give her plenty of fruits, vegetables, and foods
with protein (beans, lentils, eggs, meat, fish, and milk products). If the child
looks pale, check for signs of anemia and be sure she gets iron-rich foods
(meat, eggs, and dark green leafy vegetables) or takes iron pills (ferrous
sulphate) and vitamin C (oranges, lemons, tomatoes, etc.)
· As much as is possible, the
child should learn to examine her own body for pressure sores every day and take
responsibility for all the necessary preventive measures herself.
Other precautions
· To avoid pressure sores or
other injuries on feet that do not feel, use well-fitted, well-padded sandals or
shoes. These and other precautions are discussed under “Spina Bifida”
and “Leprosy”.
· To avoid pressure sores when
straightening limbs with casts, put extra padding over bony (2) spots before
casting and do not press on these spots as the cast hardens. Listen to the child
when he says it hurts, and check where it hurts.

Figure
If it hurts in one of the spots marked with an X, it may be a
pressure sore. Remove the cast and see.
If it hurts in these spots (1), it is probably the tight
cord (tendon). A little pain is normal with stretching, but
if it hurts a lot, examine it.

Figure
Changing positions
When a child has recently had a spinal cord injury, he must be
turned regularly, taking great care not to bend his back.
One good way is to roll him over using a sheet under him, like
this (1).

Figure
As the child gets stronger, hang loops and provide other aids,
if needed, so she can learn to turn herself.

Figure
 At first it is important that the person
turn, or be turned, at least every 2 hours, day and night. Later, if
there are no signs of pressure sores, the time between turns can gradually be
lengthened to 4 hours. To avoid sleeping through the night without
turning, an alarm clock can be a big help.
At first it is important that the person
turn, or be turned, at least every 2 hours, day and night. Later, if
there are no signs of pressure sores, the time between turns can gradually be
lengthened to 4 hours. To avoid sleeping through the night without
turning, an alarm clock can be a big help.
When the child begins to sit or use a wheelchair, there
is a new serious danger of pressure sores. The child must get into the habit
of taking the pressure off his butt every few minutes.
Juan has strong arms. He can lift up his whole body and hold it
up for a minute or two. This lets the blood circulate in the butt.

Figure
Jos�’s arms are weak. He takes the pressure off his butt by
leaning his whole body over the armrest, first on one side, and then on the
other.
When doing this, one buttock lifts in the air.
Figure
Carlota has a wheelchair with a low back, so she can lean back
and lift her hips off the seat.
Figure
If the chair has no armrests, or they can be removed, the child
can lie sideways over a pillow on a high bed. He can rest for 15 to 30 minutes
like this.

Figure
If he has very little arm and body control, he can put his feet
on the floor (with help if needed) and lean forward with his chest on his knees.
This takes the pressure off his butt.

Figure
Or have someone tip his chair backward for one minute or more.
For a longer ‘nap’ that rests the butt, someone can tip his chair
backward onto a cot.

Figure
|
To prevent pressure sores when sitting, take the weight off
your butt for one whole minute at least once every 15 minutes! |
Padding and cushions for lying
To prevent pressure sores, it is essential that the person who
has lost feeling lie and sit on a soft surface that reduces pressure on bony
areas.
· It is best to lie on a flat
surface with a thick, spongy mattress.
A thick foam rubber mattress often works well. However,
some foam is so spongy that it sinks completely down under weight. Then the bony
area is not protected from the hard board. A firm sponge with very small air
bubbles (microcell rubber) works well, but is expensive.

Figure
A ‘waterbed’ (bag-like mattress filled with water) or
air mattress also works well.
In some countries, an excellent mattress material is made of
rubber-coated coconut fiber. Urine can be washed out by pouring water through it
(1). Because this material is costly, a rehabilitation program in
Bangladesh cuts a square out of a cheap mattress and fits in a square of the
coconut fiber sponge.
Figure
· Careful placement of
pillows, pads, or soft, folded blankets can also help prevent
pressure sores. These are especially important in the first weeks or months
after a spinal cord injury when the person must lie flat and be moved as little
as possible. Pillows should be placed to avoid pressure on bony places, and to
keep the person in a position that is healthy and that helps prevent
contractures.

BACK-LYING
SIDE-LYING
BELLY-LYING
Chair and wheelchair cushions
For the child who has lost feeling in his butt, the type of seat
cushion he uses is very important - especially if his
paralysis makes it difficult to lift up or change positions.

Figure
All spinal cord injured persons should use a good
cushion.
Sitting directly on a canvas or a poorly padded wood seat causes
pressure sores.
Special cushions are made with ‘soft spots’ of an
almost-liquid ‘silicone gel’ in the areas of greatest pressure.
However, these cushions are very expensive. Also, the gel may get too soft and
liquid in hot weather.
Good cushions can be made of ‘microcell’
rubber, which is fairly firm. It works best if it is cut and shaped to
reduce pressure on bony areas:
(1) Dip at back keeps hips from slipping forward.
(2) Hollow in back keeps pressure off butt bones.
(3) Raised ‘shelf’ here puts more pressure under
thighs, less on butt. It also helps keep the hips from slipping forward.
(4) A ‘thigh separator’ can be included if
needed.

Figure
A good, low-cost way to make a fitted cushion is to build a base
out of many layers of thick cardboard glued together. Cover it with a 2
or 3 cm. - thick layer of sponge rubber.
Wet the cardboard and sit on it wet for 2 hours, so it forms to
the shape of the butt. Then let it dry, and varnish it.

Figure
Before making a specially-fitted cushion, you can make a
‘mold’ of the person’s butt by having him sit in a shallow
container of soft clay, mud, or plaster. Note the bony hollows and form the seat
to fit them.

Figure

Figure
Air cushions made from bicycle inner tubes are excellent
for prevention of pressure sores, and for bathing on a hard surface. Use 1, 2 or
more tubes, depending on size of tube and size of child.
Figure
Bind loops of the tubes together with thin straps of inner tube
(1).
Pump in enough air so that the whole butt is held up by air.
(Idea from wheelchair rider-builders at Tahanan Walang Hagdanang
(House With No Stairs), Quezon City, Philippines)

Figure
TREATMENT OF PRESSURE SORES
Watch for the first signs of a pressure sore by examining the
whole body every day. Teach the child to do this using a mirror.

Figure
If early signs of a sore appear (redness, darkness, swelling, or
open skin), change body positions and use padding to protect that area from
pressure.
For larger areas (like the bones near the base of the spine),
you can try using a small (motor scooter) inner tube to keep weight off the sore
area. Put a towel over the tube to soak up sweat. (Sweaty skin against the
rubber can also cause sores.)

Figure
|
WARNING: For small areas such as heels,
never use a ring or ‘donut’ of cloth to keep weight off the
sore. This can cut off blood supply to the skin inside the ring and make the
sore worse.

Figure
|
IF A PRESSURE SORE HAS ALREADY FORMED:
· Keep pressure
off the sore area completely and continuously.
· Keep the area completely
clean. Wash it gently with clean or boiled water twice a day. Do not
use alcohol, iodine, merthiolate, or other strong antiseptics.
· Eat well. If lots of
liquid comes out of the sore, a lot of protein and iron are lost with it. These
must be replaced for quicker healing. Also take iron pills if signs of anemia
are present. Eat foods rich in protein: beans, lentils, eggs, meat, fish, milk
products.
· Do not rub or massage
areas where pressure sores might be forming. This could tear weakened flesh and
make the sore inside bigger.

This paraplegic young man has a
large pressure sore on his butt. Until it heals, he must not sit. Village
rehabilitation workers made this wheel lying cart for him to move about on. Here
he helps a boy learn to walk. (Photo, John Fago.)
IF A SORE IS DEEP AND HAS A LOT OF DEAD FLESH:
· Clean the sore 3
times a day.
· Each time, try to scrape and
pick out more of the dead rotten flesh. Often, you will find the sore is much
bigger inside than you first thought. It may go deep under the edges of the
skin. Little by little remove the dead flesh until you come to healthy red flesh
(or bone!).
· Each time after cleaning out
the dead flesh, wash the sore out well with soapy water. Use liquid surgical
soap if possible. Then rinse with clean (boiled and cooled) water.
Figure
A large plastic or glass syringe works well for washing out the
sore. Wash the syringe well with soap and water after each use.
Figure
If the sore is infected (pus; bad smell; swollen; red;
hot area around the sore; or the person has fevers and chills):
· Clean out the sore
3 times a day as described.
· If possible, take the person
to a ‘clinical laboratory’ where a sample from the sore can be removed
and ‘cultured’ to find out what germs are causing the infection and
what medicine is most likely to fight it well.
· If a ‘ culture’ is
not possible, try treating the person with penicillin, tetracycline, or (if
possible) dicloxacillin. (See WTND)
· Follow the advice of an
experienced health worker.
If the sore does not get better, or keeps draining liquid or
pus from a deep hole, the bone may be infected. In this case, special
studies, treatment, and possible surgery may be needed. Try to take the person
to a capable medical center. (See Chapter 19.)
Two folk treatments that help in curing pressure sores
PAPAYA (PAW PAW)

Figure
Papaya has chemicals (enzymes) that digest dead meat. Cooks use
it to soften meat. The same chemicals can help soften the dead flesh in a
pressure sore, and make it easier to remove.
First clean and wash out a pressure sore that has dead flesh in
it. Then soak a sterile cloth or gauze with ‘ milk’ from the trunk or
green fruit of a papaya plant and pack this into the sore. Repeat cleaning and
repacking 3 times a day.
HONEY AND SUGAR
Once a pressure sore is free of dead flesh, filling it 2 to 3
times a day with honey or sugar helps prevent infection and speeds healing.
This treatment, used by the ancient Egyptians, and recently rediscovered by
modern doctors, works remarkably well. It is now being used in some American and
British hospitals.
To make filling the sore easier, mix honey with ordinary sugar
until it forms a thick paste. This can easily be pressed deep into the sore.
Cover the sore with a thick gauze bandage.

A village rehabilitation worker
treats a young man’s pressure sores with a paste made by mixing honey and
sugar.
|
CAUTION: It is important to clean out and refill the
sore at least 2 times a day. If the honey or sugar becomes too diluted with
liquid from the sore, it will feed germs rather than kill them. |
Molasses can also be used. In Colombia, South America, doctors
shave thin pieces off blocks of raw sugar and put these into the
sore.
Chapter 25: Urine and Bowel Management: With Spinal Cord Injury and Spina Bifida
Most persons with spinal cord injury or spina
bifida do not have normal bladder or bowel control
(control for peeing and shitting). This loss of control can be inconvenient,
embarrassing, and cause social and emotional difficulties. Also, the loss of
control can cause skin problems and dangerous urinary infections.
For these reasons, it is important to learn ways to stay clean, dry, and
healthy. Most of the methods are not difficult, so children should be able to do
it themselves. This will help them feel more self-reliant.
URINE MANAGEMENT
The main goals of urine management are:
1. to prevent urinary infection, and
2. self-care
in staying as dry as possible.
Prevention of urinary infection is extremely important.
Infections of the urinary system (bladder and kidneys) are very common in both
spinal cord injury and spina bifida, and are one of the main causes of early
death. Therefore, any method used for self-care or staying dry must also
help prevent urinary infections. Make every effort to prevent germs from getting
into the bladder. Keeping clean is essential. Also, it is important to
empty the bladder regularly as completely as possible. If some urine stays in
the bladder, bacteria will grow in it and cause infection.
|
The ideal method of urine control empties the bladder completely
and in a clean, regular, easy, and self-reliant way. |
Different methods work best for different persons - depending
mostly on what ‘type’ of bladder a person has.
Figure
‘Types’ Of bladder - in persons whose feeling
and control have been partly or completely lost.
|
AUTOMATIC BLADDER: A person with paralysis
whose legs have ‘reflex spasms’ (uncontrolled stiffening or jerking)
usually also has reflex spasms in his bladder. As the bladder fills with urine,
the walls of the bladder stretch and cause a reflex spasm. As the bladder
squeezes, the muscles that hold back the urine relax, letting the urine flow
out. This is called an ‘automatic bladder’ because it empties
automatically when it gets full. |
LIMP BLADDER (flaccid bladder): When a person’s
paralyzed legs are limp and do not have spasms, usually the bladder is also
limp, or flaccid. No matter how much urine fills the bladder, it will not
squeeze to empty. The bladder stretches until it cannot hold any more and the
urine begins to drip out. The bladder does not completely empty this way. Some
urine stays in the bladder, increasing the chance of infection. |
The most simple methods of bladder management work well with an
automatic bladder but do not work with a limp bladder. So try to figure out
which type of bladder a child has.
For the first few days or weeks after the spinal cord has been
injured, the bladder is almost always limp. Urine either drips out or does not
come out at all. Then, as the ‘spinal shock’ wears off, persons with
higher back injuries (above the 2nd lumbar vertebra) usually develop automatic
bladders. In persons with lower back injuries, the bladder usually stays limp.
During the first weeks, usually a ‘Foley catheter’ is
kept in the bladder all the time. However, after about 2 weeks, it is a good
idea to test how the bladder works by removing the catheter and trying one of
the methods described in this chapter. If the person is often wet, try another
method for that type of bladder.
|
A catheter is a flexible rubber tube used for draining
urine out of the bladder.

Standard catheter
A ‘Foley’ catheter has a small balloon near the tip
(1). This balloon is filled with water when it is inside the bladder, so that it
can be left inside and will not slip out.
Water is injected into the balloon here (2).
Urine drains out here (3).
Foley catheter
|
Methods for automatic bladder
1. TRIGGERING: This method usually causes the
bladder-emptying reflex to work when the person is ready to pee. It can be done
using a urinal, toilet, potty or jar. This is the first method to try
because nothing is put into the bladder. It is easy, so a child can do it alone.

Figure
· Tap the lower
belly (over the bladder) firmly with your hand for about 1 minute. Stop and wait
for the urine to come.
· Tap again. Repeat several
times until no more urine flows.
If possible, once a week after triggering use a catheter to see
how much urine is left. If there is less than a cupful (150 cc.), continue the
triggering program. If there is more than a cupful on several occasions, then
the bladder is not emptying well enough. Try another method.
2. PERIODIC USE OF A CATHETER: This method allows the
bladder to be emptied completely before becoming too full. Sometimes it can be
used to prepare the body for triggering. Put a clean or sterile standard
catheter into the bladder every 4 to 6 hours to empty the urine.
|
CAUTION: If you drink more liquid than usual, put
in the catheter more frequently to keep the bladder from stretching too much.
|

Figure
Note: To reduce risk of urinary infections, regular frequent
use of the catheter is more important than using a sterile catheter. It is a
mistake to stop using the catheter only because you don’t have a chance to
boil it (for example, when traveling, or at school). Just wash out the catheter
with clean drinkable water after use, and keep it in a clean jar or towel. Do
not go too long without catheterizing, and do not stop catheterizing
altogether. It is important for your bladder not to interrupt your program.
How to put in a catheter
Health workers and parents can easily be taught to put in a
catheter. With a little practice, paraplegic and some quadriplegic children can
also learn.
Note: The best catheter size is usually
from #8 or #10 for a small child to #14 or #16 for a large child.

Children as young as age 5 can
learn to catheterize themselves

A mirror can help girls to find
the urine hole
|
Note: The great care with cleanliness shown here (boiling the
catheter, wearing gloves) is important when using a fixed (Foley) catheter.
However, for periodic use of a regular catheter, a clean rather than
sterile technique is more practical (and therefore may be safer). Wash
the catheter well with clean water after each use and keep it in a clean
container. Wash your hands well before using it. |
1. If possible boil the catheter (and any syringe or instrument
you may be using) for 15 minutes, or at least wash them well and keep them
clean.
Figure
2. Bathe well (at least daily). Wash well under foreskin or
between vaginal lips and surrounding areas.

Figure
3. Wash hands with soap. After washing touch only things that
are sterile or very clean.
Figure
4. Put very clean cloths under and around the area.
Figure
5. Put on sterile gloves-or rub hands well with alcohol or
surgical soap.
Figure
6. Cover the catheter with a lubricant (slippery cream) like
K-Y Jelly that dissolves in water (not oil or
Vaseline).

Figure
7. Pull back foreskin or open the vaginal lips,

Figure
8. Holding the lips open or the foreskin back, gently put the
catheter into the urine hole. Twist it as necessary but DO NOT FORCE IT.
Figure
9. Push the catheter in until urine starts coming out - then 3
cm. more.

Figure
10A. If using a regular catheter, each time you pee tighten your
stomach muscles or gently massage the lower belly to empty all
urine. Then take out the catheter, wash it well, boil it, and store it in a
clean jar or towel.
10B. If using a Foley (permanent) catheter, inject 5 cc. of
sterile water into the little tube, to fill the balloon (or up to 10 cc. if it
is a 30 cc. Foley), and connect the bigger tube to the collection tube or leg
bag.
Change the catheter every 2 weeks (or more often if there is an
infection).

Figure
|
To avoid infections when using a catheter, it is important to
be very clean and to use only a catheter that is sterile, boiled, or very
clean. |
3. FOLEY CATHETER (fixed catheter): With this method, the
catheter is left in all the time to drain the urine from the bladder
continuously. A Foley is often used immediately after injury, and in some cases,
for many months or years. The catheter connects to a collection bag that can be
attached to the leg and worn under the clothes.
In many areas this is the easiest method because other supplies
are difficult to get. However, a Foley can cause many problems, including:
· Bacteria can get
into the bladder, causing a high risk of infection.
· Continuous bladder
irritation can cause bladder stones to form.
· The catheter may cause a
sore on the underside of the penis through which urine leaks. This may need
surgery to correct.
If you have tried other methods unsuccessfully or no other
equipment is available, a Foley catheter may be the only choice. To prevent
complications it is very important that it be used carefully:
· Always wash your
hands well before touching the catheter.
· Clean the skin around the
catheter with soap and water at least twice a day and after each bowel movement.
· Do not disconnect the
collection bag except to empty and wash it. Wash it out with soap or bleach
(Clorox) and water once a day.
· If the catheter must be
clamped, use a sterile plug, never a glass ampule (small bottle).
It may break and cause injury.
· Keep the collection bag below
the level of the bladder to keep the urine from flowing back.
· Tape the catheter to the leg
when in a wheelchair. Boys should tape the catheter on belly when lying down.
· Check regularly to make sure
the urine is emptying and that the catheter is not plugged up. Avoid sharp bends
or folds in the tubing.
· When turning, lifting, or
moving the person, remember to move the bag too. Do not let it pull at the
catheter or stay under the person.
· If the catheter gets plugged
up, take it out, squirt boiled water through it, and put it back. Or use a new
one. In emergencies, you can squirt a little (cool) boiled water back through
the catheter while it is in place. Use a sterile or very clean
syringe.
4. CONDOM CATHETER: This is a practical method for men
and boys who cannot control their urine. It can be used in combination with
triggering, to avoid accidental wetting.
condom catheter
A condom catheter is a thin rubber bag that fits over the penis.
It has a tube that connects to a collection bag. They come in different sizes.
If condom catheters are too costly or not available, a regular
condom (‘rubber’, ‘sheath’, or ‘prophylactic’ for
family planning) can be attached to the collection tube with a rubber band or
tape.

regular condom
Or a thin, very clean plastic bag can be used. Or, on a child,
use the finger of a rubber glove (or a ‘fingercot’).

polyethyene bag
Figure
To hold the condom on the penis, a special very stretchy
adhesive tape can be used as shown in this series of drawings.
|
How to put on a condom using Con-stay tape |
|
Warning: Use only Con-stay or another easily
stretchable adhesive tape. (Ordinary adhesive tape can stop blood flow when the
penis swells.) |
|
1. Cut off hair.
Figure
|
|
2. Pull back skin. Wash with soap and water and dry well.
Figure
|
|
3. Apply ‘skin prep’ (tincture of benzoin) to help
condom stick to skin.

Figure
|
|
4. Pull foreskin forward over head of penis.
(a) Roll on condom leaving some space here.

Figure
|
|
5. Loosely wrap Con-stay tape around condom so it sticks
to itself.

Figure
|
|
6. Roll the condom back over the tape.

Figure
|
|
7. Add a second strip of tape, ½ on the condom and ½
on the skin.

Figure
|
|
8. Cut off the rubber rim.
Figure
|
|
9. Connect condom to leg bag.

Figure
|
One of the safest and cheapest ways to hold a condom on the
penis is to cut a ring out of soft foam rubber. Pass the condom under the ring
and turn it back over it.

Figure
The ring can be used again and again. So can the condoms if they
are carefully washed.

Figure
IMPORTANT PRECAUTIONS FOR CONDOM USE:
· Be sure it is
not too tight - it could stop blood flow and severely harm the penis. Avoid
non-stretch tape.
· If the penis has erections
(gets hard and bigger), try to put on the condom when it is big.
· Remove the condom once a day
and wash the penis well.
· If possible, remove it at
night. Use a bottle or urinal to catch the urine.
· Check the condom and penis
often to be sure everything is all right.
· If the penis becomes injured,
swollen, or looks sore, remove the condom until the penis is
healthy.
Methods for the limp bladder
If the person’s bladder is limp (flaccid), it never empties
by reflex. The bladder will constantly have urine sitting in it unless an
effective emptying method is used.
Boys:
1. Put in a regular catheter every 4 to 6 hours to
empty the bladder. Between catheter use, the boy can put on a condom to catch
any leaking urine, as described.
2. A Foley catheter can be used, but may lead to problems.
3. Other alternatives include a surgical operation, which allows
the urine to come out through a small opening on the belly into a bag. Or a
special catheter is put into the bladder through a small hole in the lower
belly.
Girls:
1. They can use a Foley catheter. This is often the
simplest method, but can lead to urinary infections.
2. Or try an ‘intermittent’ (in and out) program,
using a regular catheter every 4-6 hours. If there is leaking in between
catheter times, use diapers, rags, or a thick sanitary pad to catch the urine.
Change them often and wash often to protect the skin and prevent sores.
3. The surgical procedures mentioned for boys can also be done
in girls.
OTHER SUGGESTIONS FOR THE LIMP BLADDER-BOTH SEXES
· The push method:
Push down over the bladder with the hands.

Figure
Or strain to push urine out by tightening the stomach muscles.
Or put a fist over the lower belly and gently press it by
bending forward.
Figure
This method is recommended by many professionals, but it can
cause problems. If the muscles do not relax to let the urine out, pushing on the
bladder can force urine back into the kidneys - causing kidney infection and
damage. Therefore, the push method should only be used if the urine comes out
easily with gentle pressure - or if there is no other way possible.
· With boys with a limp bladder,
the condom method can be used. But it is best to also use a regular catheter at
least 3 times a day. This is because the bladder does not empty completely,
which makes infection more likely.
URINARY INFECTIONS
Persons with spinal cord injury or spina bifida have a high risk
of urinary (bladder) infections, for the reasons we have discussed. Long-term or
untreated infections and kidney problems are a common cause of early death.
Preventive measures are essential (see the bottom of the next page); but even
when precautions are taken, some urinary infections are still likely to happen.
Therefore, it is very important to recognize the signs and provide effective
treatment.
Signs
When a person who has normal feeling has a urine infection, it
burns when he pees. The person with spinal cord damage may not feel this burning
and therefore has to use other signs to know when he has an infection. He may
learn to recognize certain unpleasant feelings, or may only know that he does
not feel as healthy as usual. Parents and health workers should learn to listen
to the child and be aware of changes in behavior or other signs that might mean
that he has an infection.
|
Possible urinary signs |
Possible other signs |
|
· cloudy urine, possibly with
pieces of mucus, pus, or blood specks
· dark or red urine
· strong or bad smelling urine
· increased bladder spasms
(cramps)
· increased wetting or changes
in bladder function
· pain in the mid-back (kidneys)
or side (urine tubes) |
· body aches
· general discomfort
· increased muscle spasms
· fever
· dysreflexia (headache,
goosebumps when sweating, high blood pressure) |
Treatment
At the first signs of infection, drink even more water than
usual. Antibiotics (medicines that fight bacteria) may also be
necessary. But avoid frequent use of antibiotics because they may become less
effective (bacteria may become resistant).
If a person has had urinary infections before, he can start with
the last medicine that was effective. If not...
· Start with one of
the medicines in Group 1 on the next page. If after 2 days the person is
still getting worse, try another medicine in Group 1.
· If that does not help, try one
of the medicines in Group 2.
· If none of the medicines of
Group 2 help, take the person to a medical laboratory for a ‘culture’
and ‘sensitivity test’ of the urine.
· If that is not possible, try a
medicine in Group 3. If possible, consult a specialist in urinary
problems.
If a medicine seems to help, continue taking it for at least a
week, or for 4 days after the last signs have disappeared. Do not change from
one medicine to another unless the medicine is not working or causes serious
side effects.
CAUTION: Many of these medicines sometimes cause
serious side effects. Find out about their risks and precautions before using
them.
* The medicines marked with a star (*) can cause kidney damage
unless the person drinks lots of water.
Be sure to give the medication in the correct dosage.
|
TREATMENT FOR URINARY INFECTIONS |
|
Medical name (and common brand) |
Age |
Dose |
Repeat the dose |
|
Group 1 |
A. * Sulfisoxazole (Gantrisin) |
up to 5 years |
500 mg. |
4 times |
|
|
5 to 10 years |
750 mg. |
a day |
|
|
over 10 years |
1000 mg. |
|
|
B. Nitrofurantoin (Furadantin, Macrodantin) |
up to 5 years |
25 mg. |
4 times |
|
|
over 6 years |
50 mg. |
a day |
|
Group 2 |
A. Ampicillin (many brands) |
up to 4 years |
125 mg. |
4 times |
|
|
4 to 8 years |
250 mg. |
a day |
|
|
over 8 years |
500 mg. |
|
|
Caution: Do not use for persons allergic to
penicillin |
|
B.* Sulfamethoxazole 400 mg. with trimethoprim 80 mg.
(Bactrim or Septra) |
up to 4 years |
½ tablet |
|
|
|
4 to 9 years |
1 tablet |
2 times |
|
|
9 to 12 years |
1½ tablets |
a day |
|
|
over 12 years |
2 tablets |
|
|
Note: This medicine also comes in double
strength
(Bactrim DS and Septra DS). Adjust doses if using
double strength. |
|
C. Cephalexin (Keflex) or a similar
‘cephalosporin’ |
up to 5 years |
125 mg. |
4 times |
|
|
over 5 years |
250 mg. |
a day |
|
Group 3 |
A. Carbenicillin (Geocillin) |
up to 6 years |
¼ tablet |
4 times |
|
|
6 to 10 years |
½ tablet |
a day |
|
|
over 10 years |
1 tablet (382 mg.) |
|
|
Note: Take 1 hour before or 2 hours after
eating. |
|
B. Tetracycline (many brands) |
over 8 years |
500 mg. |
4 times a day |
|
Caution: Do not give to children under 8
years, or to women who are pregnant or breast feeding. If possible, avoid taking
milk products with tetracycline. |
|
All persons with a urinary infection Should always drink lots of
water while they are taking medicine. After the infection is gone, continue
drinking lots of water, and take all preventive measures. |
PREVENTION OF URINARY INFECTIONS

To prevent urinary infections,
drink LOTS OF WATER
· Drink lots of liquid - adults,
at least 2 liters (8 glasses) a day.
· Eat apples, grapes, or
cranberries - or drink their juices - or take vitamin C tablets to make urine
more acid. Bacteria grow with more difficulty in acid urine.
(Note: Orange or lemon juice and other citrus
fruits and juices do not work! They make the urine less acid.)
· Keep hands, catheter, and
collection bags very clean before, during, and after your bladder program.
· Do not lie in bed all day.
Stay active.
· Do not clamp the Foley
catheter or plug it with anything - unless absolutely necessary - then use a
sterile plug.
· Stick to your bladder program.
Do not allow urine to sit in bladder.
· Do not let the catheter get
bent or twisted so that urine cannot come out.
· If using a standard catheter
periodically, be sure to put it in regularly, at least every 4 to 6 hours. To
prevent infections, frequency of catheter use is even more important than
cleanliness. It is safer to put in the catheter without boiling it, than not to
put it in. If infections are common, catheterize more often.
BOWEL MANAGEMENT IN SPINAL CORD INJURY AND SPINA BIFIDA
When there is damage to the spinal cord, almost always a person
loses control over when he will have a bowel movement (pass stool or shit). This
makes it hard to stay clean, which can be inconvenient or embarrassing. Although
he can never get back complete control over the muscles that hold in or push out
the stool, a person can learn to help the stool come out, with assistance, at
certain times of day. This kind of ‘bowel program’ can
greatly increase the person’s self-confidence and freedom for school, work,
and social activities.
Persons with spinal cord damage also often have problems with
constipation, or the formation of hard stools that may wait days before coming
out. Some constipation can be an advantage when a person lacks bowel control.
But sometimes it can lead to serious problems, such as impaction or dysreflexia.
It is therefore important to prevent serious constipation:
· Drink lots of
water.
· Eat foods high in fiber (such
as bran, whole grain cereals, fruits, vegetables, cassava, beans, nuts).
· Stick to a scheduled bowel
program.
· Keep active.
Planning a bowel program
Any bowel program will work better if you:
· Do the program
every day (or every other day) and at the same hour. Do it even if
the person has had an accidental bowel movement shortly before, or has diarrhea.
· Do the bowel program at the
same time of day that the person usually had bowel movements before his injury.
Often the bowels move best after a meal or a hot drink.
· If possible, do the program on
a toilet or pot. The bowels work better sitting than lying.
· Be patient. The bowels
sometimes take days or weeks to change their pattern.

An 8-year-old paraplegic girl,
Vania, helps a 5-year-old paraplegic girl with her daily bowel program. (See
Story of J�sica)
Types of bowel
Different persons require different types of bowel programs,
depending on whether their bowels are ‘automatic’, ‘limp’,
or ‘pull back’.
· Automatic
bowel usually occurs in persons who have muscle spasms in their legs, and an
‘automatic bladder’. The muscle or ‘sphincter’ in the anus
(asshole) stays shut until there is a stimulation in the bowel to make it open,
so that the stool can come out. An automatic bowel will ‘move’ in
response to a suppository or stimulation by a finger.
· Limp or ‘flaccid’
bowel usually occurs in persons with low spinal cord damage who have limp
(not spastic) legs and bladder. The sphincter muscle in the anus is also limp.
So the person tends to ‘ooze’ or ‘dribble’ shit. A limp
bowel does not respond to finger stimulation.
· A bowel that pulls back
is neither automatic nor limp. When you put a finger up the anus, you can feel
the stool move back up instead of coming out.
PROGRAM FOR AN AUTOMATIC BOWEL
|
SUPPLIES NEEDED
· non-sterile glove, finger
glove, or plastic bag
· lubricant (vegetable or
mineral oil works well)
· old paper or newspaper
· soap and water
· if available,
suppositories such as Dulcolax or glycerin. These are
bullet-shaped pills that are pushed into the anus. They stimulate the bowel and
cause it to push out the stool (shit).

suppository
|
· Start with a
suppository if available. With a finger covered with a glove or plastic bag, and
then oil, push the suppository about 2 cm. (1 in.) up the anus. Do not push it
into the stool, but push it against the wall of the bowel. (Or try the program
without a suppository; usually finger stimulation is enough.)
· Wait 5 or 10 minutes. Then
help the person sit on a toilet or pot. If he cannot sit, have him lie on his
left side (on top of old paper).
· Put an oiled finger into the
anus about 2 cm. Gently move the finger in circles for about 1 minute, until the
anus relaxes and the stool pushes out.
· Repeat the finger action 3 or
4 times, or until no more stool is felt.
· Clean the butt and anus well
and wash your hands.
PROGRAM FOR A LIMP BOWEL
Since the bowel does not push, the stool must be taken out with
a finger. It is best done after each meal, or at least once a day.
· If possible, do it
sitting on a toilet or pot, or lying on your left side.
· With a gloved and oiled
finger, remove as much stool as you can.
· Since a limp bowel tends to
ooze stool, eat foods that make the stool firm or slightly constipated (not much
stool-loosening foods).
A thin rubber glove or ‘fingercot’ (1) helps keep the
finger clean.

Figure
If possible, have the child lie on his left side.

Children can learn to do their
own ‘bowel program’.
PROGRAM FOR A BOWEL THAT PULLS BACK
For this kind of bowel, the bowel programs already described
usually do not work. Finger stimulation makes the bowel act in the opposite
direction, and pull the stool back in. The person will have
‘accidents’ during the day. Often it works better to,
· First, put some
anesthetic jelly (such as Xylocaine) up the anus. If you cannot
get the jelly, you can mix some liquid injectable Xylocaine
(lidocaine) with Vaseline or any other jelly.
· Wait several minutes. Then do
the automatic bowel program.
OTHER IMPORTANT POINTS
· Do not use enemas
or strong laxatives regularly. They stretch the bowel, injure its muscles, and
make following a regular program more difficult. A mild laxative may be taken
occasionally, when needed. However, drinking more liquid and eating food
high in fiber is usually enough.
· If there is bright red blood
in the stool, probably a blood vessel was torn during the program. Be more
gentle! If there is dark, old blood and the stools are black and tar-like, seek
medical advice.
· A small amount of liquid stool
(diarrhea) may be a sign of ‘impaction’ (a ball of hard stool stuck in
the gut). Only liquid can leak around it. Do not give medicine to stop diarrhea;
this could make the impaction worse. Try to get it out with a
finger.
|
A bowel program may at first seem difficult and messy. But it
soon becomes an easy habit. It is very important both for the person’s
health and his social well-being. Start now, do it regularly at the same hour,
and DO NOT MISS A DAY. |
Chapter 26: Leprosy: Hansen’s Disease
What is leprosy? It is an infectious
disease that develops very slowly. It is caused by germs (bacilli) that
affect mostly the skin and nerves. It can cause a variety
of skin problems, loss of feeling, and paralysis of the
hands and feet:
|
loss of feeling (1) (burns and scars) |
|
deformities of hands and feet |
painless ulcers of the feet (2) |
|
Figure
|

Figure
|
Figure
|

Figure
|
How do people get leprosy? It can spread only from some
persons who have untreated leprosy, and only to other persons who have ‘low
resistance’ to the disease. It is probably spread either through sneezing
or coughing, or through skin contact. Most persons who come into contact with
leprosy have a natural ability to resist it. Either they do not get it at all,
or they get a small unnoticeable infection that soon goes away completely.
From the time a person is first infected with leprosy germs, it
often takes 3 or 4 years for the first signs of the disease to appear.
Leprosy is not caused by evil spirits, by doing something bad,
by eating certain foods, or by bathing in river water, as some people believe.
It is not hereditary and children of mothers with leprosy
are not born with it. However, children who live in close contact with
someone who has untreated leprosy are more likely to get it.
How common is leprosy? Leprosy is much more common in
some parts of the world than others. It is more common where there are crowded
living conditions and poor hygiene. But rich people can also get it.
Even with improved methods for treatment, today there may be
more persons with leprosy than ever before. More than 12 million people have
leprosy. In some villages in Asia, Africa, and Central America, 1 person in 20
has leprosy.
Can leprosy be cured? Yes. There are medicines that kill
leprosy germs. Usually within a few days of beginning treatment, a person can no
longer spread the disease to others. (In fact, most persons, when their leprosy
is first diagnosed, can no longer spread it.) However, treatment in some
persons must be continued for years to prevent the disease from coming back.
Is early treatment important? Yes. Early treatment stops
the spread of leprosy to others. Also, if treatment starts before loss of
feeling, paralysis, and deformities have appeared, recovery is usually complete
and the person is not physically or socially disabled.
|
Persons receiving regular, effective treatment do not spread
leprosy. |
Checking children for signs of leprosy
In areas where leprosy is common, health and
rehabilitation workers should work together with parents
and schoolteachers to check all children regularly for early signs of
leprosy. Most important are regular checkups of children in homes where
persons are known to have leprosy. Checkups should be done every 6 to 12 months
and should be continued for at least 3 years.
|
EARLY SIGNS |
WHAT TO LOOK FOR |
|
A slowly growing patch on the skin that does not itch or
hurt.
The patch may be somewhat different in color from the surrounding
skin. (Patches of leprosy are never completely white, and are not scaly, except
during a reaction) |
Examine the whole body for skin patches, especially the
face, arms, back, butt, and legs. |
|

Figure
If you find a slightly pale patch (1) without a clear edge, keep
watching the spot. Unless feeling is reduced inside the patch, look for other
signs before deciding it is leprosy. (Many children have similar pale spots on
cheeks and arms that are not leprosy.) |

Figure
ringworm-like patches (2), with or without raised border |
|
Note: In early skin patches, feeling is
often normal, or nearly so. If feeling is clearly reduced inside a patch,
leprosy is almost certain |
|
LATER SIGNS |
TEST INSIDE THE SKIN PATCHES FOR REDUCED FEELING. |
|
1. Tingling, numbness, or some loss of feeling in the hands
and feet.
Or definite loss of feeling in skin patches. |

Figure
|

Figure
|
|
(1) With the tip of a feather or stiff thread, lightly touch the
skin inside and outside the patch and have the child tell you (without looking)
where he feels the touch.
(2) Thread tied to stick |
If the child cannot feel the thread, try pricking lightly with a
sterile needle. |
In a similar way, test for a numbness or reduced feeling in the
hands and feet. |
|
WARNING: Sterilize the needle in a flame
before testing another child. |
|
2. Slight weakness or deformity in the hands and feet.
(1) drop foot (Child cannot raise it.)
(2) weakness or clawing of toes. |
Have the child straighten her fingers. If she cannot do this, it
may be a sign of paralysis from leprosy. |
Also have the child try to touch the base of her little finger
with her thumb. |

Figure
(1) Muscle weakness here makes this movement difficult
and may be a sign. |
|

Figure
|

Figure
|

Figure
|
|
|
(CAUTION: These weaknesses may also be
caused by polio, muscular dystrophy, or other problems.) |
|
3. Enlargement of certain nerves, with or without pain or
tenderness. The affected nerve feels like a thick cord under the skin. When they
are quite thick, they may be easily seen. |

thickening nerve below the ear
(From A Manual of Leprosy)
|
Check for large nerves in these places. |
Figure
(1) Also check for large nerves in or near skin patches. |
Diagnosing leprosy
Although skin patches are often the first sign of leprosy, many
other diseases can cause similar patches. Only when there is a loss of feeling
inside the skin patch, as compared with the skin outside the patch, can we be
almost sure the person has leprosy. However, in some forms of leprosy, loss of
feeling in skin patches may develop only years later, or not at all. Therefore,
other evidence of leprosy must be looked for.
Another sign of leprosy - tingling, numbness, or loss of feeling
in hands and feet-may also have other causes.
To make a fairly certain diagnosis of leprosy, the person
should have at least 1 of these 3 major signs:
1. definite loss or change of feeling in skin patches

Figure
Note: Leprosy patches on face often do not lose
feeling as much as on other parts of the body.
2. definite enlargement of nerves
Figure
(For nerves to check)
3. presence of leprosy bacilli in a ‘skin
smear’
A ‘split skin smear’ is prepared by cutting a thin
layer of skin from a skin patch. Less commonly it is taken from the moist skin
deep inside the nose - an area that is often heavily infected. The skin sample
is placed on a glass slide, colored with special stains, and examined with a
microscope.

Figure
The bacteria (bacilli) of leprosy, if present, can be seen under
the microscope.

taking a ‘split skin
smear’ from a skin patch

leprosy bacilli as seen in the
microscope
|
Whenever you suspect leprosy but the diagnosis is
uncertain, a ‘skin smear’ should be taken (by a trained worker).
|
Note: Not many persons with leprosy show all 3 of
these signs. Persons with loss of feeling in skin patches usually have no
bacilli in their skin smears.
Types of leprosy
Depending on how much natural resistance a person has, leprosy
appears in different types. Here are the characteristics of the main types.
|
TUBERCULOID LEPROSY (TT)
· in persons with relatively
high resistance
· no bacilli in skin smear
· Person cannot pass leprosy on
to others.
· Skin patches are few. They may
be very variable in appearance, but often have raised margins and (1) and flat
centers (2)
Figure
· Feeling is usually reduced or
absent in centers of the skin patches. (1)

Figure
· Skin patches usually lose hair
and are dry (do not sweat).
· Skin on the face is not
usually thickened.
· Nerve damage appears early,
but usually only involves loss of feeling in skin patches. Usually it does
not affect the eyes, hands, or feet. When it does, it often happens early
and causes loss of feeling or strength in only one hand or foot.
· Usually responds quickly to
treatment because the body helps fight the disease. |
‘BORDERLINE’ LEPROSY
combines features of
both tuberculoid and lepromatous leprosy.
· few to many bacilli in skin
smears
· many skin patches, raised or
flat with well-marked, often irregular edges, and some feeling loss; patches
about the same on both sides of the body
Figure
· Borderline leprosy may
suddenly shift toward one or the other extreme. When these shifts occur,
‘leprosy reactions’ are especially likely to appear.
· Severe nerve damage often
results, with loss of feeling and loss of strength in both hands and both
feet, with deformities.

Figure
Depending on where it falls along the line between the two
extremes, borderline leprosy is divided into:
borderline tuberculoid (BT),
borderline (BB), and
borderline lepromatous (BL). |
LEPROMATOUS LEPROSY (LL)
· in persons with very low
resistance
· bacilli - very many in skin
smears
· Person can pass leprosy to
others (until treated).
· There are usually very many
skin patches - variable in appearance, but often with raised lumps or thickened
areas. In early stages, feeling is usually normal inside these patches.

Figure
· The skin of the face may
become thick, lumpy, reddish, especially over the eyebrows, cheeks, nose, and
ears.

Figure
· The bridge of the nose may
gradually sink in.
· Nerve damage and paralysis
often appear late, if the leprosy is not treated.
· Loss of feeling and strength
affects both hands and both feet equally.
· Response to treatment is often
slow. Treatment must usually be continued for at least 2 years. |
Leprosy reactions
Sometimes persons with leprosy have sudden periods of increased
problems. These may be something like an allergic reaction to the leprosy
bacilli. Leprosy reactions can happen in untreated persons, during treatment, or
after treatment has stopped. Reactions can occur when there are changes in the
body, such as puberty in boys, in late pregnancy or following childbirth, during
illness from other causes, after vaccination, or at times
of emotional stress.
There are 2 types of leprosy reactions:
Type 1 reactions happen in persons with borderline
leprosy when the body increases its fight against the leprosy germs. There is
danger of new weakness and loss of feeling.
Signs to watch for are:
· skin patches may
become swollen and red (1)
· swollen hands
and feet
· new tingling or weakness of hands
and feet
· pain or discomfort along nerves
(Rarely, lumps along the nerves form sores and drain pus.)

Figure
|
IMPORTANT: Reactions sometimes cause new
weakness and loss of feeling without nerve pain. |
Type 2 reactions happen with lepromatous leprosy. The
body is reacting against too many bacilli.
Signs may include:
· swollen, reddish,
or dark lumps under the skin, especially on the face, arms, and legs
· fever
· pain in
testicles, breasts, or fingers
· stuffiness
or bleeding of the nose
· red eye, with or
without pain.
Danger: This may lead to iritis or loss of
vision unless treated early.
Rarely, this reaction causes death due to swelling of the mouth,
throat or lungs, or to kidney problems.
|
IRITIS (INFLAMMATION OF THE IRIS)
NORMAL EYE
EYE WITH IRITIS
Pain may begin suddenly or gradually. The eye waters a lot. It
hurts more in bright light. There is no pus as with conjunctivitis. Vision is
usually blurred.
This is a medical emergency. Antibiotic ointments do not
help. Get medical help. |
If untreated, leprosy reactions can quickly lead to permanent
nerve damage with increased paralysis of the hands, feet, or eye muscles, or to
permanent damage to the eyes.
|
Early treatment of leprosy reactions is very important to
prevent paralysis, deformity, and blindness. |
Treatment of leprosy reaction is discussed.
TREATMENT AND MANAGEMENT OF LEPROSY
Treatment and management of leprosy include 4 areas.
1. Long-term medical treatment to control the
leprosy infection should begin as early as possible.
2. Emergency treatment when necessary to control and
prevent further damage from leprosy reactions.
3. Safety measures, aids, exercises, and education to prevent
deformities (sores, burns, injuries, contractures).
4. Social rehabilitation: Work with the individual, the
parents, the schools, and the community to create a better understanding of
leprosy, to lessen people’s fears, and to increase acceptance, so that the
child or adult with leprosy can lead a full, happy, meaningful
life.
Medical treatment
Medical treatment of leprosy varies according to the policies
and resources of the particular country and health ministry. For years, DDS
(dapsone) has been the main drug used. Unfortunately, in some areas the
leprosy bacilli are becoming ‘resistant’ to DDS (are not harmed by
it).
Rifampin usually works much faster against leprosy.
However, it is more costly and can also cause serious side effects. Still, where
possible, it should be used. To prevent development of resistance, it is usually
given in combination with other anti-leprosy medicines. When given in
combination with DDS, rifampin probably needs to be given only once a month.
This reduces both cost and side effects.
Clofazimine, although less effective in killing leprosy
bacilli than rifampin, has the advantage that it also helps control leprosy
reaction.
Multi-drug treatment, consisting of rifampin, DDS, and
clofazimine, is now recommended by the World Health Organization. It greatly
reduces the time needed for treatment, especially for tuberculoid leprosy.
Instruction for the dosage and precautions for these different
medicines should be obtained from the local leprosy control program. Usually it
is wise to cooperate with these programs instead of trying to treat leprosy by
yourself.
Importance of long-term treatment
Treatment to cure leprosy takes a long time: from 1 to 2 years
or more, depending on the type of leprosy and the medicine used. If treatment is
stopped too soon, not only can leprosy return, but sometimes a leprosy reaction
may result which can cause even more nerve damage and paralysis or blindness.
It is therefore essential that health and
rehabilitation workers make sure the person with leprosy and her family
understand the importance of taking the medicines regularly.
Health centers should take care always to keep a reserve supply
of medicines on hand.
|
TREATED EARLY, LEPROSY NEED NOT BE A DEFORMING OR DISABLING
DISEASE. |
Treatment of leprosy reactions
As we mentioned, feeling loss, paralysis, and deformities need
not happen to a person with leprosy. Early diagnosis and treatment together
with quick care of leprosy reactions should prevent the development of many
deformities.
Care of a leprosy reaction has 4 objectives:
· Prevent nerve
damage that causes loss of feeling, paralysis, and contractures.
· Stop eye damage and prevent blindness.
· Control pain.
·
Continue with medicine to kill leprosy bacilli and prevent the disease from
getting worse.
Care includes:
1. Medicine to reduce pain and inflammation
For mild reactions (skin inflammation but not pain or
tenderness of nerves) aspirin is the best and cheapest drug.
Chloroquine (a medicine for malaria) is also effective.
To adults, give 2 tablets of 250 mg. at night (to avoid dizziness) for no more
than 2 or 3 weeks. Give less to children, according to their weight.
For severe reactions (pain along nerves, increasing
tingling, numbness or weakness, eye irritation, or painful testicles)
corticosteroids (prednisolone) may be needed. Because this is a medical
emergency and because corticosteroids are dangerous and often misused
medicines, if at all possible get experienced medical advice before using
them.
2. Anti-leprosy medicine should be continued throughout the
leprosy reaction.
Clofazimine can be used instead of DDS, as clofazimine
helps to reduce reactions and fights the leprosy bacilli. The dose of
clofazimine can often be increased (to 200 mg. daily in adults) and later
reduced as the reaction lessens. However, for severe reactions that damage
nerves, prednisolone is needed.
3. Splinting and exercise
Holding the affected limbs in splints during a severe reaction
helps reduce pain and prevent nerve damage and contractures. (See Chapter 8.)
Joints should be splinted in the most useful position. Splints
can be made of plaster bandage or molded plastic. Very carefully pad splints for
hands or feet that do not feel pain.

A good splint for the hand - to
avoid contractures and maintain a useful position.
Leave the splint on day and night until pain and
inflammation are gone. Remove only for gentle range-of-motion exercise at least
once a day. (See Chapter 42.)
Cause of deformities
When most people think of leprosy, they think of the severe
deformities of the advanced case: deep open sores (ulcers), clawed fingers,
gradual loss of fingers and toes, and eye damage leading to blindness. Actually,
these deformities are not caused directly by leprosy germs, but result from
damaged nerves. Nerve damage causes 3 levels of problems, one leading to the
next:
|
LEVEL 1: loss of feeling, of sweating, and of strength in
certain muscles |
LEVEL 2: injuries, joint stiffness |
LEVEL 3: progressive deep infections with bone
destruction and loss of vision |
|

Eyes do not blink normally
|
leads to ® |

eye irritation and infection
|
leads to ® |
scarring and blindness
|
|

Hands do not feel; skin dry;
weakness of fingers and thumb
|
leads to ® |

stiffness and contractures of
fingers and thumbs; also burns and injuries
|
leads to ® |

loss of bone
|
|

Feet do not feel; skin dry;
|
leads to ® |

painless sores and injuries
stiffness and contractures; |
leads to ® |

loss of bone
|
|
often PREVENTABLE with medical treatment of leprosy
before there is nerve damage |
often PREVENTABLE with protective eye and skin care and exercise
to keep full movement of joints |
often PREVENTABLE with careful early treatment of sores, burns,
and infections |
When there are level 1 problems, there is a lifelong danger
of level 2 and 3 problems. Because feeling has been lost, the person no
longer protects herself automatically against cuts, sores, thorns, and other
injuries. And because they do not hurt, these injuries are often neglected.
For example, if a person with normal feeling walks a long way
and gets a blister, it hurts, so he stops walking or limps.
|
But when a person with leprosy gets a blister, it does not hurt.
|
So he keeps walking until the blister bursts and becomes
infected. |
Still without pain, the infection gets deeper and attacks the
bone. |
In time the bone is destroyed and the foot becomes more and more
deformed. |
|

Figure
|

Figure
|
Figure
|

Figure
|
Usually, leprosy bacilli cannot be found in these open sores.
This is because the sores are not caused by the bacilli. Instead, they are
caused by pressure, injury, and secondary infection.
PREVENTION OF INJURY for persons with loss of feeling and
strength
Eyes: Much eye damage comes from not blinking enough,
because of weakness or loss of feeling. Blinking keeps the eyes wet and clean.
If the person does not blink well, or his eyes are red, teach him to:
· Wear sunglasses
with side shades, and maybe a sun hat.

Figure
· Close the eyes
tightly often during the day, especially when dust blows.
· Roll the eyeballs up as you
try to close eyes tight.

Figure
· Keep eyes clean.
Wash well around eyes, keep flies and dirty hands away.
Hands: When you work with your hands, or cook meals, take
special care. Never pick up a pan or other object that might be hot
without first protecting your hand with a thick glove or folded cloth. If
possible, avoid work that involves handling sharp or hot objects. Do not
smoke.
· Use tools with
smooth, wide handles, or wrap cloth around handles.
To help the person with weak or deformed fingers hold a tool or
utensil, you can mold a handle to the shape of the person’s closed hand.
Use epoxy putty, or plaster of Paris mixed with a strong glue.
Have the person grip the handle while it is still soft. Then let it
harden.

Figure
For more aids for gripping.
Feet:
· Avoid going
barefoot. Use shoes or sandals. (For suggestions on appropriate footwear,
see the next page.)

Figure
· Learn to take
short steps.
This helps protect the feet.

Figure
INJURY CARE
Eyes: Close eyes often. If necessary, use a simple eye
patch. If eye gets infected (forms pus) use an antibiotic eye ointment. Put the
ointment into lower lid without touching the eye.

Figure
Figure
Hands and feet: If you have a cut or sore, keep the
injured part very clean and at rest until it has healed completely. Take care
not to injure the area again.
Things to do every day
· Checkups:
At the end of each day (or more often if you work hard or walk far)
examine your hands and feet carefully - or have someone else
examine them. Look for cuts, bruises, or thorns. Also look for spots or areas on
the hands and feet that are red, hot, swollen, or show the start of blisters. If
you find any of these, rest the hands or feet until the skin is completely
normal again.
Figure
· If the skin gets
dry and cracks, soak the feet daily in water for at least 20 minutes.
Then rub cooking oil, Vaseline, or lanolin hand cream into
them (not butter or animal fat. These attract insects and rats).

Figure
· As you rub oil
into the hands and feet, do stretching exercises to keep the complete range of
motion in the joints.
|
With continued daily care, most deformities of leprosy can
be prevented. |
PREVENTION of contractures and deformities in persons with
paralysis
Prevention of contractures from paralysis
due to leprosy is similar to prevention of hand and foot contractures due to
polio and other forms of paralysis. However, loss of feeling makes prevention
more difficult.
Exercises to maintain full range of motion are covered in
Chapter 42.
· Exercises to
prevent fixed clawing of the hands can be done by ...
|
... gently straightening the fingers like this: |
and like this: |
|
|

Figure
|

Figure
|
Open your fingers as much as you can without help. Then use your
other hand to open them the rest of the way. Close fingers and repeat |
· A good exercise to
prevent ‘tiptoe’ contractures with ‘foot drop’ is to stretch
the heel cords by leaning forward against a wall or by
squatting with heels on the ground.

Figure
Footwear for persons without feeling in their feet
The best footwear has:
· a well-fitted
upper part that does not rub and has plenty of toe room (or leaves toes open).
(1)
· a soft innersole about 1 cm.
thick.(2)
· a tough under-sole so thorns,
nails, and sharp rocks do not injure foot.(3)
· Footwear should be acceptable
(not look too strange or unusual) so that the person will use it.

Figure
|
AVOID:
· plastic shoes or sandals
· soft-soled sandals or thongs
that thorns can pass through
· using nails to fasten heels
and soles (These might poke through and injure the foot. Better to sew on soles
or use glue.)

NO!
|
Possible ways to get footwear
· Contact a leprosy
hospital with a footwear workshop. They can make sandals if you send a tracing
of the foot. (1)

Figure
· Check the market.
You may find a canvas shoe or tennis shoe that already has a good
insole.

Figure
· Or you can put
soft insoles into the shoes. But CAUTION: If you put an
insole that is thick into a standard shoe, there may not be enough room for the
toes - unless you cut out the part over the toes and leave them
open.
Figure
· Make (or have a
local shoemaker make) special footwear.
For the inner sole, you can use a soft sponge sandal or
‘thong’. Or buy ‘microcell’ rubber, which is soft but firm.
(1)

Figure
For the under-sole you can use a piece of old car
tire.

Figure
· For persons who
have developed sores on their foot here (1), a bar here (2) or a foot (3)
support here may help take pressure off the ball of the foot and prevent new
sores.

Figure

Figure

Figure
· A very helpful
lining for preventing sores is a soft, heat-moldable foam plastic called
‘Plastazote’. For instructions on making footwear
with Plastazote, see Insensitive
Feet.

Figure
· For persons with a
‘drop’ foot, a brace or ‘lift’ can help prevent sores
and injuries.
|
You can get a brace or support at a rehabilitation workshop, or
make a specially-fitted, well-padded plastic brace. |

Figure
|
Or make a simple device to hold the foot up. |
Figure
|
LEPROSY AND THE COMMUNITY
Historically, there has been a lot of fear and misunderstanding
about leprosy. Persons with leprosy have often been thrown out of towns or
treated with cruelty. Until recently, governments took persons with leprosy away
from their families and locked them up in special institutions or
‘leprosaria’. All this added to people’s fears.
Today, leprosy can be cured - without any deformities or
disabilities if treatment is begun early. It can be treated in the home. The
person can continue going to school or to work. Having leprosy need not disable
the person physically or socially.
But in many communities fear and misunderstanding remain.
Persons still refuse to admit - even to themselves - the early signs of leprosy.
They delay in getting treatment until permanent deformities appear. The disease
continues to be spread to others by those who are not yet treated. And so the
myth and the fear of leprosy are kept alive.
To correct this situation will require the efforts of all health
and rehabilitation workers, schoolteachers, religious and community leaders,
families of persons with leprosy, and organizations of the disabled. These steps
are needed:
1. Information and Education Schools, health
centers, comics, radio, and television can be used to help educate the community
about leprosy. Information should:
· try to
lessen the fears people have about leprosy and let them know it is
curable.
· stress the importance of early
diagnosis and treatment.
· tell people how to
recognize early signs and where to get treated.
· include popular stories of persons who think they
might have leprosy, decide to get help, and are cured.
2. Integration of leprosy programs into general
health care. Too often leprosy control is done as a separate program. It is
important that people (and health workers) begin to see leprosy as ‘just
another serious health problem’ - like diarrhea in children.
3. Regular screening (mass checkups) of children for skin
patches and other early signs of leprosy. This can be part of a
‘CHILD-to-child’ program (see Chapter 47) in which school children
learn first to examine each other, and then their younger brothers and sisters.
A ‘CHILD-to-child Activity Sheet on Leprosy’ is available from
TALC.

Screening school children for
leprosy, India. (Photo, The Leprosy Mission.)
4. Community pressure and government orders
to let children being treated for leprosy attend school, find work, attend
festivals, and take part in public functions. (Organizations of disabled persons
can help make this happen.)
5. Community support groups to help persons with leprosy
feel accepted, cared for, and respected; also to make sure that they take their
medicines regularly and learn to prevent deformity. Where needed, support groups
can help persons with leprosy get the schooling, health care, work, and social
rights they deserve.
|
The example of a health worker who welcomes persons with leprosy
and is not afraid to touch them can do much to calm needless fears and encourage
acceptance. |
Chapter 27: Amputations
An amputation is the loss of some part of the body. Rarely,
children are born without one or both hands or feet. More often, children lose
an arm or leg because of accidents. Or limbs must be cut off because of advanced
bone infections or dangerous tumors (cancer).
Deciding what to do for a child with an amputation depends on a
number of things, including the age of the child at the time of amputation, the
amount of amputation, and above all, what the child (and parents) want and
accept.
|
MISSING BOTH HANDS (any age)
Figure
|
He will probably want and accept hooks, or whatever can help him
hold things better.

Figure
|
Until he can get gripping hooks, figure out ways to attach tools
and utensils to his stumps so he can do more for himself.

Figure
|
A child with high arm amputations from birth often learns to use
his feet almost as well as his hands.

Figure
|
|
MISSING ONE HAND

Figure
|
If she was born that way and is given an artificial limb early,
she will usually accept it and keep using it.

Figure
|
But if her hand was amputated as an older child or she has gone
for a long time without an artificial limb...
Figure
|
... she may prefer to keep using the stump, and refuse a limb
even if one is made for her.
|
|
AN AMPUTATION BELOW THE KNEE (one or both legs)

Figure
|
He should get an artificial leg as soon after the amputation as
possible - or by one year: of age.

Figure
|
A growing child will often need a new, larger limb. Therefore,
try to fit him with low-cost limbs that are easy to replace.

Figure
|
Limbs with detachable feet - although often expensive - can be
lengthened.

Figure
|
|
ONE LEG AMPUTATED ABOVE THE KNEE

Figure
|
Up to age 10 (or more) she can walk well with a straight leg (no
knee joint).

Figure
|
When older, she may prefer and will often walk better on a leg
with a knee joint (if the family or program can pay for it and can keep
replacing it as the child grows).

Figure
|
|
|
BOTH LEGS AMPUTATED ABOVE THE KNEES

Figure
|
When very young, he may move about most easily on short
‘stump’ limbs.

Figure
|
When older, he may prefer longer limbs that make him as tall as
other children-even if this means using crutches.

Figure
|
Children with very high amputation of the legs may do best in
wheelchairs.
|
CARE OF THE AMPUTATED LIMB
The goals in caring for the stump are to maintain a good
shape and good position for fitting an artificial limb. This means
taking active steps to:
1. avoid swelling,
2. keep the full
range of motion (prevent contractures), and
3. maintain
strength.
WRAPPING THE STUMP
To prevent swelling and keep a good shape for fitting an
artificial limb, it is important to wrap the newly amputated limb for a long
time after it has been cut off.
The leg should be wrapped in a way that squeezes the liquid in
the leg upward (rather than trapping it at the end). Use an elastic bandage in
this manner:

Figure
Below knee

Figure
Above knee

Figure
ELEVATING THE STUMP
In addition to being wrapped, a newly amputated limb should be
kept lifted high up most of the time. Avoid spending a lot of time with the arm
or leg hanging down.
Figure

Figure
PREVENTION of contractures
A child with an amputated leg does not use his leg normally. He
usually keeps it bent, and he tends to develop contractures of the hip or knee
(or both).
Therefore, special positioning and exercises are
needed to prevent contractures and maintain full range of motion.
Contractures here and here will need to be straightened before
this child can be fitted with a limb. (1)

Figure
POSITIONS
Encourage positions that keep the joints stretched, and avoid
those that keep the joint bent.
|
CORRECT |
CORRECT |
WRONG |
CORRECT |
|

Figure
|
Figure
|

Figure
|

Figure
|
|
WRONG |
WRONG |
CORRECT |
|

Figure
|
Figure
|

Figure
|
|
ONLY WHEN NECESSARY FOR MOVING ABOUT |
BETTER
(But it can still cause hip contractures.) |
CORRECT |
|
Figure
|

Figure
|

Figure
|
|
If contractures have already developed, try to position the
child in ways that stretch them. |

Figure
|

Figure
|
STRETCHING EXERCISES
|
Figure
|
|
|

Figure
|

Be sure hips are straight.
|

Figure
|
STRENGTHENING EXERCISES
Try to strengthen especially those muscles that straighten the
joints, and those muscles needed for walking.
|

Figure
|

Figure
|

Figure
|
|

Figure
|
Figure
|
Figure
|
Figure
|
|
WARNING about walking aids
Walking aids or artificial limbs, like these, that keep the
stump bent may be useful until the child can get a limb that keeps the joint
straight. (1)

Figure
However, it is very important that the child do stretching
and strengthening exercises daily if he uses a bent-joint aid.
Figure
With a well-fitted stump-in-socket limb, normal activity usually
provides all the stretching and exercise that are needed.
Instructions for making simple stump-in-socket limbs using
bamboo and other local materials are in Chapter 67. |
ALTERNATIVES FOR A CHILD WITH AMPUTATED HANDS
|

Figure
|

Figure
|

Figure
|

Figure
|
|
simple tool and utensil holders made of cloth, leather, or
plastic |
cuff with changeable tips |
hooks that open and close to grip (operated by movements of
shoulders and back) |
surgery that turns the 2 bones of the forearm into pinchers
|
|

Figure
|

Figure
|
|
|
rubber or wood hand, not for use but for looks |
instead of hooks, an artificial hand with a thumb that opens and
closes against 2 fingers (expensive and may not last) |
|
This is a grasping aid for a child whose fingers have been lost
but the base of the hand and wrist joint remain.
Child presses stump against
post

Figure
|
The type of aid a child and her parents choose for an amputation
will depend on several things, such as availability, cost, usefulness, looks,
and local cultural factors. For help in choosing an appropriate aid,
see Chapter 56, “Making Sure Aids and Procedures Do More Good Than
Harm”. |
Chapter 28: Burns and Burn Deformities
Serious burns are common in villages where people cook, warm
themselves, or sleep by open fires.
First aid for burns is discussed in health care manuals,
including Where There Is No Doctor. Here we discuss only
the precautions that can be taken to help prevent deformities and
disabilities from burns.
The most common deformities resulting from severe burns are
contractures, and the scarring, or sticking together, of skin around
joints. For example:
|

Figure
|

Figure
|

Figure
|

Figure
|
|
Lupito slept too close to the fire and his blanket caught fire.
|
He was badly burned under the arm and behind the knee. |
As he was healing, Lupito lay with his arm and leg bent. This
kept the air away from the burns, and they hurt less. |
But as a result, the skin scarred to itself. After the burns
healed, Lupito could not lift or straighten his arm or straighten his leg. |
TO PREVENT SCARRING TOGETHER OF THE SKIN AT JOINTS:
|
Figure
|

Figure
|

Figure
|
|
Keep the joints extended (straight) while the burns heal. You
may have to support or tie the limbs so that the child does not bend them in his
sleep. |
For burns between fingers or toes, keep them separated with
sterile cloth pads with Vaseline. |
To keep the chin from scarring to the chest, it is very
important to keep the head tilted up as the burns heal. |
TO HELP BURNS HEAL: When possible, leave the burns
open to the air.
|

Figure
|
Protect against flies and dust with mosquito netting or by
covering the burns with light gauze. |
Figure
|
To keep the blanket or mosquito netting off a burned part of the
body, cut a cardboard box or make a frame to hold it up. |
If burns need to be covered, you can put petroleum jelly
(Vaseline) on sterile gauze or sterilized cloth and gently
cover the burn.
|
To help healing, and to prevent or control infection of deep or
open burns, you can put bees’ honey or sugar directly on the burn.
Or make a paste of bees’ honey mixed with sugar. It is important to wash
the burn with water that has been boiled and cooled, and to put on fresh honey 2
or 3 times each day. (If the honey gets too diluted with oozing from the
burn, it will breed germs rather than kill them.) |

Figure
|
BEES’ HONEY IS EXCELLENT FOR HEALING BURNS AND OPEN SORES
|
Ways to help burns heal faster and better
|
Skin grafts
Large deep burns heal very slowly and form ugly stiff scars.
Healing can be faster and scarring reduced by using ‘skin grafts’. A
very thin layer of skin from another part of the body is stretched over the
burn. Usually this is only done by a surgeon (although some village health
workers have been taught how to do it). |

Figure
|
Also, to speed healthy healing, you can use the fresh ‘bag
of waters’ or transparent membrane that comes out with the placenta after
childbirth.
This sac must be kept clean. Wash it in boiled and cooled,
slightly salted water, and put it on the burn as soon as you take it out of the
water. |
RANGE-OF-MOTION EXERCISES
As soon as burns are covered with new skin or by a scar, gently
begin range-of-motion exercises. Slowly straighten and bend the affected joint -
a little more each day.
|
Figure
|
For exercise details, see Chapter 42. If scarring is severe, you
may need to continue range-of-motion exercises for years after burns are healed.
Scar tissue does not grow and stretch like normal skin. Skin contractures
often form and may slowly get worse - sometimes even with exercises.
Before beginning exercises, it helps to rub body oil or cooking
oil into the healed burn (but never into a fresh burn). Reports from several
parts of the world claim that fish oil on healed burns helps prevent thick
scarring and skin contractures. |
SURGERY
|
When joints are scarred down or severe contractures form after
burns, ‘plastic surgery’ may be needed. Sometimes skin is taken
from another part of the body and used to add more skin over the joint area (a
skin transplant).
In case of severe burns that have destroyed fingers or thumb,
special ‘reconstructive’ surgery may help to return use of the hand.
(This surgery is very costly and usually can only be done by special surgeons in
larger hospitals.) |

Figure
For example, if the thumb has been destroyed, sometimes a finger
(or toe) can be attached to the end of the stump so that the child can grasp
things better. (1)
index finger moved to form thumb (2) |
PREVENTION of burns is important:
|

Figure
|
Figure
|
Figure
|
|
Keep small children away from fires. Where there are open fires,
be sure an older child or someone else watches the young children carefully.
|
Keep matches and explosives out of reach of children. |
Turn handles of pans on stove so that the small child does not
pull them. |
Chapter 29: Fits: Epilepsy
Epilepsy
What are they? Fits (also called seizures or convulsions)
are sudden, usually brief, periods of unconsciousness or changes in mental
state, often with strange jerking movements.
One out of every 10 or 20 children has at least 1 fit by age 15.
But only 1 in 50 of these children goes on to have chronic fits (repeated fits
over a long period of time) - a condition known as epilepsy.
Figure
CAUSES OF CHRONIC FITS (EPILEPSY)
Fits come from damage to, or an abnormal condition of, the
brain. Common causes include:
· Injury to the
brain. This causes at least 1/3 of epilepsies. Injuries may be before birth,
during birth, or at any time after. The same causes of brain damage that result
in cerebral palsy can cause epilepsy. In fact, cerebral palsy and epilepsy
often occur together. Meningitis is a common cause of this combination. In
small children common causes of fits are high fever or severe dehydration
(loss of liquids). In very ill persons, the cause may be meningitis,
malaria of the brain, or poisoning (see Where There Is No
Doctor). Epilepsy that steadily gets worse, especially if other signs of
brain damage begin to appear, may be a sign of a brain tumor (or of
hydrocephalus in a baby). Fits caused by a tumor usually affect one side
of the body more than the other. Rarely, fits may be caused by pork tapeworms
that form cysts in the brain (see WTND).
· Hereditary. There is a
family history of fits in about 1/3 of persons with fits.
· Unknown causes. In
about 1/3 of epilepsies, no family history or history of brain damage can be
found.
Fever fits. Children who have once had a fit with a high
fever often will have fits again when they have a fever-especially if other
persons in the family have had fits with fever. Be sure to check for
infections of the ears and throat, as well as bacterial dysentery
(diarrhea with blood and fever), and treat the cause.
Fits that come only with fever usually stop occurring by the
time the child is 7 years old. Sometimes they may develop into
‘non-fever-related epilepsy’, especially if the child has signs of
brain damage (see “Cerebral Palsy,”).
|
WARNING: Fits in a very ill child may be a
sign of meningitis - for which immediate medical treatment is
necessary to save his life. Learn how to check for signs of meningitis (see
Where There Is No Doctor).

MENINGITIS
The spasms of tetanus can be mistaken for fits. The jaw
shuts tightly (lockjaw) and the body suddenly bends back. Learn to spot early
signs of tetanus (see WTND).

TETANUS
|
MORE ABOUT FITS (EPILEPSY)
Mental ability. Some children with epilepsy are
intelligent. Others are mentally slow. Occasionally, fits that are very frequent
and severe can injure the brain and cause or increase
retardation. Treatment to control fits is important.
Types of fits. Fits may appear very differently in
different children. Some may have severe, ‘big’ or ‘major’
fits with strong, uncontrollable movements and loss of consciousness. Others may
have smaller or ‘minor’ fits. These can be ‘brief spells’
with strange movements of some part of the body. They can be sudden unusual
behavior such as lip-sucking or pulling at clothes. Or they can be brief
‘absences’ in which the child suddenly stops and stares - perhaps with
blinking or fast movement of the eyelids.
Some children will have both minor and ‘big’ fits or
they may first have minor ones and later develop big ones.
Warning signs or ‘aura’. Depending on the kind
of fits, the child (and parents) may be able to sense when a fit is about to
begin. Some children experience a ‘warning’ in which they may see
flashes of light or colors. Or they may suddenly cry out. In one kind of fit,
the ‘warning’ may be fear or imagined sights, sounds, smells, or
tastes. In some kinds of fits there is no ‘warning’. The child’s
body may suddenly jerk or be thrown violently. These children may need to
continuously wear some kind of safety hat or other head protection.
Timing of fits. Fits may happen weeks or months apart, or
very often. Minor fits or ‘absences’ may come in groups - often in the
early morning and late afternoon.
Fits are usually short. Minor fits may last only a few seconds.
Big fits seldom last more than 10 or 15 minutes. Rarely, however, a child may
enter into a long ‘epileptic state’ which may last hours. This is a
medical emergency.
Some kinds of fits may appear at any age. Others begin in early
childhood and usually disappear or change to other patterns as the child grows
older.
Many persons have epilepsy all their life. However, some
children stop having fits after a few months or years.
Usually there is no need to know the exact kind of fits a child
has. However, some kinds of fits require different medicines. The chart
describes the main types of fits, when they begin, and their treatment.
WHEN ARE SPECIAL MEDICAL STUDIES NEEDED?
In some poor countries, doctors sometimes prescribe medication
for fits without properly checking for signs of causes that may need attention.
However, more and more doctors regularly order expensive testing such as an
‘EEG’ (electroencephalogram). Even if these services are
‘free’, they are often only available in a distant city, which causes
the family much time and expense. Such tests do not usually help much in
deciding treatment - unless a brain tumor is suspected. And even if it is a
tumor, the possibilities of surgery or successful treatment may be very small,
and the costs are often much too high.
|
Usually EEG’s and other costly testing are not
helpful. |
WHAT TO DO WHEN A CHILD HAS A FIT
· Learn to recognize
any ‘warning signs’ that a fit is about to begin, such as sudden fear
or a cry. Quickly protect the child by lying her down on a soft mat or other
place where she cannot hurt herself.
· When a ‘big’ fit
starts, do not try to move the child unless she is in a dangerous place.
· Protect the child as best
you can against injury, but do not try to forcefully control her movements.
Remove any sharp or hard objects near her.
· Put nothing in the
child’s mouth while she is having a fit - no food, drink,
medicine, nor any object to prevent biting the tongue.
· Between spasms, gently turn
the child’s head to one side, so that spit drains out of her mouth and she
does not breathe it into her lungs.
· After the fit is over, the
child may be very sleepy and confused. Let her sleep. For headache,
which is common after a fit, give acetaminophen (paracetamol) or
aspirin.
|
HEAD PROTECTION
To protect the head of a child who falls hard when she has a
fit, it may be wise for her to wear some kind of head protection most of the
time. |
Figure
|
|
A child who often injures his face with fits may need a
‘hard hat’ helmet with a face mask.

Figure
|
|
You can make a ‘cage’ of stiff wire and wrap it with
strips of inner tube, soft cloth, or sponge rubber. |

Figure
|
Or cut a piece of old car tire something like this.

Figure
|
Or sew strips of cloth filled with padding. |

Figure
|
MEDICINES TO PREVENT FITS
There are no medicines that ‘cure’ epilepsy. However,
there are medicines that can prevent the fits of most children - as long as they
keep taking the medicine regularly. As long as a child has epilepsy - which
may be for years or all his life - he must continue to take anti-fit
medicines.
Sometimes preventing fits for a long time seems to help stop
epilepsy permanently. For this reason, if the child has had many fits in the
past, it is usually wise for him to keep taking anti-fit medicines regularly for
at least one year after the last fit. Only then should you gradually lower and
stop the medication to see if he still needs it.
|
CAUTION: Great care is needed to select the
medicines that help the individual child most, and which do her the least harm.
Try to avoid giving so much medicine that she always seems sleepy, dizzy,
slow-moving, or loses interest in things. A few fits may be better than too much
medicine - which can poison the child. |
Choosing medicines
The best medicine (or medicines) for a child with epilepsy is
one that is:
· effective
(prevents the fits).
· safe (has few side
effects).
· cheap (because it must be taken
for years).
· easy to take (long-acting, few
doses a day).
· easy to get.
|
WARNING: When a child is having a fit do
not put his feet into a fire. It will not ‘frighten him back to
life’ but will severely burn him.

Figure
|
Many different medicines are used for epilepsy. Some types of
fits are controlled better by one medicine and some by another medicine, or by a
combination of medicines. Some children’s fits are easy to control. Others
are very difficult. It may be necessary to try different medicines and
combinations to find the most effective treatment. In a few children, no
medicines will control the fits completely.
The best medicine to try first for almost all types of fits
is usually phenobarbital. Often it is very effective, and is relatively
safe, cheap, and easy to take. Its effects last for 24 hours, so that one dose a
day is usually enough.
The next best medicine for ‘big’ fits is usually
phenytoin. It is also fairly safe, cheap, and usually needs to be taken only
once a day. (For some kinds of epilepsy, however, phenytoin may make fits
worse.)
For most epilepsies, phenobarbital and phenytoin are often
the best drugs. First try each alone, and if that does not work, try both
together. Most other drugs are less likely to be effective, are often less safe,
and are much more expensive.
Unfortunately, many doctors prescribe more expensive, less safe,
and often less effective medicines before trying phenobarbital or phenytoin.
Partly this is due to drug companies that falsely advertise their more expensive
products. In some countries, phenobarbital is difficult to get - especially in
pill form. The result is that many children’s fits are poorly controlled,
using drugs that cause severe side effects and that are very costly.
Rehabilitation workers need to realize this and do what they can
to help provide the safest, cheapest medicines that will effectively control
each child’s fits.
|
CAUTION: To prevent choking, do not give medicines
to a child while she is lying on her back, or if her head is pressed back.
Always make sure her head is lifted forward. Never give medicines by mouth to a
child while she is having a fit, or while she is asleep or unconscious. |
It is usually best to start with only one anti-fit medicine -
usually phenobarbital, if available. Start with a low to medium dose, and
after a week, if fits are not controlled and if there are no serious side
effects, increase to a higher dose. After a few days, if the fits are still
not controlled, add a second medication - usually phenytoin, for ‘big
fits’. Again, start with a low to medium dose and gradually increase as
needed.
|
CAUTION: When you stop or change a child’s
medicine, do so gradually. Sudden stopping or changing the medicine may make
fits worse. Also, it may take several days for a new medicine to have its full
effect. |
|

|
WARNING: All anti-fit medicines are poisonous if a
child takes too much. Be careful to give the right dose and to keep medicines
out of reach of children. |
INFORMATION ON DOSAGE AND PRECAUTIONS FOR ANTI-FIT
MEDICINES
|
Phenobarbital (phenobarbitone, Luminal)
For all types of fits. Usually comes in: |
|
tablets of 15 mg. |
|
|
tablets of 30 mg. |
(It costs less to buy 100 mg. tablets and cut them into pieces).
|
|
tablets of 100 mg. |
|
|
Dosage: Because tablet sizes differ, we
give the dosage in milligrams (mg.).
The usual dose is 3 to 6 mg. for each kg. of body weight every
day (3 to 6 mg./kg./day) - usually given in 2 doses (morning and
evening):
Give 2 doses a day. In each dose give: |
|
children over 12..... |
50 to 150 mg. |
|
children 7 to 12 years... |
25 to 50 mg. |
|
children under 7 years... |
10 to 25 mg. |
|
SIDE EFFECTS AND COMPLICATIONS
· Too much can cause
sleepiness or slow breathing.
· Some very
active children become over-active or behave badly.
· Rare side effects include mild dizziness,
eye-jerking, and skin rash.
· Bone growth
problems may occur - especially in retarded children. Extra vitamin D may
help.
· Bitter taste. It may help to grind up
the tablet and give it with honey or jam.
· Mildly habit
forming. |
|
|
CAUTION: If tablets of 100 mg. are used, be
very sure the family understands that they must be cut into pieces. Show them
first and then have them do it. |

|
Giving a whole tablet instead of a small piece can poison the
child. |
|
|
Phenytoin (diphenylhydantoin, Dilantin)
For all types of fits except brief fits
that suddenly throw the child out of balance (‘jolt fits’) or
‘minor fits’ with staring, blinking, or fast movement of eyes.
(Phenytoin may make these kinds of fits worse.) |
|
Usually comes in: |
capsules of 30 mg. |

Figure
|
|
|
capsules of 100 mg. |
|
|
syrup with 125 mg. in each 5 ml. (1 teaspoon) |
|
Dosage: using capsules of 100 mg. 5 to
10 mg./kg./day
Start with the following dose once a day:
children over 12 years..... 100 to 300 mg. (1 to 3
capsules)
children 7 to 12 years...... 100 mg. (1 capsule)
children 6 or
under.......... 50 mg. (1/2 capsule)
After 2 weeks, if the fits are not completely prevented, the
dose can be increased, but not to more than twice the amount.
If child has no fits during several weeks, try lowering the dose
little by little until you find the lowest dose that prevents the fits.
SIDE EFFECTS AND COMPLICATIONS
WARNING: Watch for dizziness,
eye-jerking, seeing double, and severe sleepiness. Lower the dose if
any of these occur. They are early signs of poisoning, which could cause
permanent brain damage.
· Swelling and
abnormal growth of the gums often occurs with long-time use. It can be
partly prevented by good mouth care. Be sure the child brushes or cleans his
teeth and gums well after eating. If he cannot do it by himself, help him,
or better, teach him. If the gum problem is severe, consider changing medicines.
(See Where There Is No Dentist.)
very swollen, sore gums almost
covering teeth-caused by not keeping teeth clean while taking phenytoin (1)
· Occasional side
effects: increased body hair, rash, loss of appetite, vomiting.
· High dosage may cause liver
damage.
· Bone growth problems sometimes
occur - especially in retarded children. Extra vitamin D may help.
WARNING: Sudden stopping of phenytoin may
cause the child to have a long-lasting fit. Therefore, when stopping or
changing the medicine, lower the dosage gradually. |
|
Carbamazepine (Tegretol)
Useful for almost all types of fits as a second choice, or in
combination. Especially useful for ‘psychomotor’ fits. High cost is a
disadvantage. (Unfortunately, many doctors prescribe it as first choice when
cheaper drugs such as phenobarbital or phenytoin are likely to work as well or
better.)
Usually comes in: tablets of 200 mg.
Dosage: 14 to 25 mg./kg./day divided into 2
to 4 doses. Start with 20 mg. each day for each kilogram the child weighs. For
example, a 30 kg. child 10 years old would start with 600 mg. a day, which she
could take in 3 doses, each of 200 mg. - or one tablet 3 times a day.
It is best to take it with meals.
The dose of carbamazepine should be adjusted to the individual
child. Depending on how well it controls the fits, it can be raised to 30
mg./kg./day (but no higher) or dropped to 10 mg./kg./day.
SIDE EFFECTS AND COMPLICATIONS
· Rarely causes
liver damage or reduces ability of blood to clot. |
|
OTHER DRUGS SOMETIMES USED FOR EPILEPSY
· Primidone
(Mysoline) For all fits. Start with low doses and gradually
increase to 10 to 25 mg./kg./day in 2 to 4 divided doses. May cause sleepiness,
dizziness, vomiting, or rash.
· Ethosuximide
(Zarontin) First choice for ‘minor fits’ with blank
staring, eye-fluttering, and perhaps strange motions - especially if the fits
occur in groups in the morning and evening. Give 10 to 25 mg./kg./day in 1 or 2
doses, with food to avoid stomach ache. Rarely causes liver damage.
· Valproic acid
(Depakene) Used alone or in combination with other anti-fit
drugs, for ‘minor fits’ with blank staring or ‘absences’,
especially when the fits occur in groups. Start with 5 mg./kg./day and increase
gradually to 30 mg./kg./day; never give more than 60 mg./kg./day. Few side
effects. Rarely causes liver damage.
· Mephenytoin
(Mesantoin) Used like phenytoin but much more dangerous. May
stop the body making red and white blood cells. Regular blood checks needed. 4
to 1 5 mg./kg./day divided into 2 doses. (We mention it here mainly to
discourage its use.)
· Corticosteroids (or
corticotropin) These are sometimes tried for ‘baby
spasms’ and ‘jolt fits’ that are not controlled by other
medicines. But long-term use of these medicines always causes serious and
possibly dangerous side effects. They should be used only with highly
skilled medical advice when all other possible medicines have failed.
· Diazepam
(Valium) Sometimes used for ‘newborn fits’ or
‘baby spasms’, but other medicines should be tried first. May cause
sleepiness or dizziness. Mildly habit forming. Give about 0.2 mg. for each
kilogram of body weight per day, in divided doses.
|
CAUTION DURING PREGNANCY: Many of the
anti-fit drugs, especially phenytoin, may increase the risk of birth defects
when taken by pregnant women. Also, some of the drug goes into breast milk.
Therefore, pregnant women should use these drugs only when fits are common or
severe without them. Women taking fit medicine should not breast feed if they
are able to feed their babies well without breast milk. Phenobarbital is
probably the safest anti-fit medicine during pregnancy. |
TREATMENT FOR A LONG-LASTING FIT
When a fit has lasted more than 15 minutes:
· if someone knows
how, inject IV diazepam (Valium) or phenobarbital into
the vein.
|

Figure
|
Doses for injectable diazepam: |

Figure
|
Doses for injectable phenobarbital: |
|
Adults .. 5 to 10 mg.
Children 7-12 years... 3 to 5
mg.
Children under 7... 1 mg. for every 5 kg. of body weight. |
|
Adults........ 200 mg.
Children 7-12 years.... 150
mg.
Children 2-6 years.... 100 mg.
Children under 2 years... 50 mg. |
· or put a
‘suppository’ of diazepam, paraldehyde, or phenobarbital up the rectum
(asshole).
|
NOTE: These medicines do not work as fast
or well when they are injected into a muscle. If you only have injectable or
liquid medicine, put it up the rectum with a plastic syringe
without a needle. Or grind up a pill of diazepam or phenobarbital, mix with
water, and put it up the rectum. |
Figure
|
Putting diazepam up the rectum works faster than injecting it
into a muscle. |
If the fit does not stop in 15 minutes after giving the
medicine, repeat the dose. Do not repeat more than once.
Types of epileptic fits
Note: This information is for rehabilitation
workers and parents because many doctors and health workers do not treat fits
correctly. With care, perhaps you can do better. However, correct diagnosis and
treatment can be very difficult. If possible, get advice from a well-informed
medical worker. Ask her help in using this chart. It is adapted from
Current Pediatric Diagnosis and Treatment by Kempe, Silver, and
O’Brien (Lange Medical Publishing), in which more complete information is
provided.
|
TYPE |
AGE FITS BEGIN |
APPEARANCE |
TREATMENT |
|
Newborn fits

Figure
|
birth to 2 weeks |
Often not typical of later fits. May show sudden limpness or
stiffness; brief periods of not breathing and turning blue; strange cry; or eyes
roll back; blinking or eye-jerking; sucking or chewing movements; jerks or
strange movement of part or all of body.
WARNING: Make sure spasms are not from
tetanus or meningitis.
With cerebral palsy in the newborn, the baby is usually limp.
Stiffness and/or uncontrolled movements usually appear months later, but the
baby does not lose consciousness. |
Phenobarbital or phenytoin. Add diazepam if not controlled.
(Fits due to brain damage at birth are often very hard to
control.) |
|
Baby spasms (West’s syndrome) |
3-18 months (sometimes up to 4 years)

Figure
|

Figure
Sudden opening of arms and legs and then bending them - or
repeat patterns of a strange movement. Spasms often repeated in groups
when waking or falling to sleep, or when very tired, sick, or upset.
Most children with these spasms are retarded. |
Corticosteroids may be tried - but are dangerous. Try to get
help from an experienced doctor or health worker. Valproic acid or diazepam may
help. |
|
Fever fits (fits that only occur when child has a fever)

Figure
|
6 months to 4 years |
Usually ‘big’ fits (see next page) that happen only
when child has a fever from another cause (sore throat, ear infection, bad
cold). May last up to 1 5 minutes or longer. Often a history of fever fits in
the family.
WARNING: Look for signs of meningitis.
|
A child who has had fever fits on several occasions should be
treated with phenobarbital continuously until age 4 or until one year after the
last fit. Fits usually do not continue in later childhood. |
|
Jolt or ‘lightening bolt’ fits (Lennox-Gastaut
syndrome)

Figure
|
any age but usually 4-7 years |
Sudden violent spasms of some muscles, without warning, may
throw child to one side, forward, or backward. Usually no loss of consciousness,
or only brief.
Many children also have ‘big’ or generalized fits.
May be a history of ‘baby spasms’ (see above) in
earlier childhood. |
Try phenobarbital, with valproic acid. If no improvement,
consider trying corticosteroids as in baby spasms, or other medicines with
medical advice.
Protect child’s head with headgear and chin padding.

Figure
|
|
Blank spells or ‘absences’ (petit mal). (This type of
fit alone is rare.) |
3-15 years

Figure
|
Child suddenly stops what she is doing and briefly has a
strange, empty or ‘blank’ look. She usually does not fall, but does
not seem to see or hear during the fit. These ‘absences’ usually
happen in groups. She may make unconscious movements, or her eyes may move
rapidly or blink. These fits can be brought on by breathing rapidly and deeply.
(Use this as a test.) Often confused with ‘psychomotor’ fits, which
are much more common. |
Valproic acid or ethosuximide. Since many children also have
‘big’ fits, add phenobarbital if necessary (or try it first if you
think the fits might be ‘psychomotor’ - see below). |
|
‘Marching’ fits (Focal fits) |
any age |
Movement begins in one part of the body. May spread in a certain
pattern (Jacksonian march) and become generalized.

Figure
Note: If fits that occur in one part of the
body get worse and worse, or other signs of brain damage begin to appear, the
cause might be a brain tumor. |
Phenobarbital or phenytoin (or both). If poor results, try
carbamazepine or primidone. |
|
Mind-and-body fits (psycho-motor fits)

Figure
|
any age |
Starts with ‘warning’ signs: sense of fear, stomach
trouble, odd smell or taste, ‘hears’ or ‘sees’ imaginary
things. Fit may consist of an empty stare, strange movements of face, tongue or
mouth, strange sounds, or odd movements such as picking at clothes. Unlike
‘blank spells’, these fits usually do not occur in groups but alone
and they last longer. Most children with psychomotor fits later develop
‘big’ fits. |
Try phenobarbital first - then phenytoin, or both together, then
carbamazepine, or all 3 together. Valproic acid may also be useful. Or primidone
instead of phenobarbital. Psychological counseling sometimes also helps. |
|
Generalized or ‘big’ fits (grand mal)

Figure
|
any age |
Loss of consciousness - often after a vague warning feeling or
cry. Uncontrolled twisting or violent movements. Eyes roll back. May have tongue
biting, or loss of urine and bowel control. Followed by confusion and sleep.
Often mixed with other types of fits. Often family history of fits. |
Try phenobarbital first. Then phenytoin. Then carbamazepine - or
combinations. Or combine primidone or methsuximide with one or more of the
others. |
|
Temper tantrum fits (not really epilepsy)

Figure
|
under 7 years |
Some children in ‘fits of anger’ stop breathing and
turn blue. Lack of air may cause loss of consciousness briefly and even
convulsions (body spasms, eyes rolling back). These brief fits, in which the
child turns blue before losing consciousness, are not
dangerous. |
No medical treatment is needed. Use methods to help the child
improve behavior (see Chapter 40). |
HELPING THE COMMUNITY UNDERSTAND EPILEPSY
Fits can be frightening to those who see someone having them.
For this reason, epileptic children (and adults) sometimes have a hard time
gaining acceptance in the community.
Rehabilitation workers need to help everyone in the community
realize that epilepsy is not the result of witchcraft or the work of evil
spirits. It is not a sign of madness, is not the result of bad actions
by the child or parents or ancestors, is not an infectious disease,
and cannot be ‘caught’ or spread to other people.
It is important that epileptic children go to school and take
part in day-to-day work, play, and adventures in family and village life. This
is true even if fits are not completely under control. The schoolteachers and
other children should learn about epilepsy and how to protect a child when she
has a fit. If they learn more about epilepsy it will help them to be supportive
rather than afraid or cruel. (See CHILD-to-child activities.)
Although children with epilepsy should be encouraged to lead
active, normal lives, certain precautions are needed - especially for children
who have sudden fits without warning. Village children can learn to help in the
safety of such a child - especially at times when danger is greatest.

Figure
PREVENTION of epilepsy
1. Try to avoid causes of brain damage - during
pregnancy, at birth, and in childhood. This is discussed under prevention of
cerebral palsy.
2. Avoid marriage between close relatives, especially in
families with a history of epilepsy.
3. When children with epilepsy take their medicine regularly to
prevent fits, sometimes the fits do not come back after the medicine is stopped.
To make it more likely that fits will not come back, be sure that the child
takes her anti-fit medicine for at least a year after her last fit. (Often,
however, fits will still return when medicine is stopped. If this happens, the
medicines should be taken for at least another year before you try stopping
again.)
Chapter 30: Blindness and Difficulty Seeing
Difficulty with seeing can be mild, moderate, or severe. When a
person sees very little or nothing, we say he is blind. Some children are
completely blind; they cannot see anything. However, most blind
children can see a little. Some can only see the difference between light
and dark or day and night, but cannot see any shapes of things. Others can see
shapes of large objects, but none of the details.
Many more children are not blind but do have some problem
seeing things clearly. For example, they may see fairly well for most daily
activities, but have trouble seeing details. The family may not realize that the
child has a seeing problem until they notice she has difficulty threading a
needle, finding head lice, or reading letters on the blackboard at school. Often
these children can see much better with eyeglasses or a magnifying glass.
(Children who are completely blind cannot see at all, even with eyeglasses.)
Some children are born blind. Others become blind during early
childhood, or later.

what a child with normal sight
can see

what a partly blind child may see
(large forms but no details)

what a child sees who can only
tell the direction a bright light is coming from

what a completely blind child
sees
|
CAUTION: Not all children who are blind have eyes
that look different. Their eyes may look clear and normal. The damage may be
behind the eyes or in part of the brain. So be sure to watch for other signs
that can tell you if a child has difficulty seeing. |
SIGNS THAT COULD MEAN A CHILD HAS A SEEING PROBLEM
· Eyes or eyelids
are red, have pus, or continually form tears.
· Eyes look dull, wrinkled, or
cloudy, or have sores or other obvious problems.
· One or both pupils (the black
center of the eye) looks gray or white.
· By 3 months of age, the
child’s eyes still do not follow an object or light that is moved in front
of them.
· By 3 months the child does not
reach for things held in front of him, unless the things make a sound or touch
him.
· Eyes ‘cross’, or one
eye turns in or out, or moves differently from the other. (Some eye-crossing is
normal up to 6 months.)
· Child squints (half shuts his
eyes) or tips head to look at things.
· Child is slower to begin using
his hands, move about, or walk than other children, and he often bumps into
things or seems clumsy.
· Child takes little interest in
brightly colored objects or pictures and books, or she puts them very close to
her face.
· Has difficulty seeing after
the sun sets (night blindness).
· In school, the child cannot
read letters on the blackboard. Or he cannot read small print in books, or gets
tired or often gets headaches when he reads.
If the child shows any of these signs, test her vision, and if
possible, see a health worker or eye doctor. Sometimes eyesight can be saved by
preventive steps or early treatment.
Methods for testing if a baby sees and for measuring
the vision of children are discussed with CHILD-to-child activities.
Blindness with other disabilities
Some children with cerebral palsy or other disabilities
are also partly or completely blind. Parents may not realize this and
think that the child’s slow development or lack of interest in things is
because he is mentally and physically handicapped. In fact, blindness may be a
large part of the cause.
Even if a child has no other disability, blindness can make
development of early skills slower and more difficult. If the child does not
look at, reach for, or take interest in things around him, check if he can see
(and hear).
|
Note: Some children with very severe brain
damage or mental retardation may seem blind. They may look at things without
really seeing them, because their brains are at the developmental level of a
newborn baby. With lots of stimulation, little by little some of these children
begin to become more aware Of things, to follow them with their eyes, and
finally to reach for them. |
Causes of blindness
Different people have different beliefs about what causes
blindness. In some parts of the world, people think a child is born blind as
punishment for something the parents have done. In parts of Latin America,
villagers believe that a bat’s urine fell in the baby’s eyes, or that
a ‘black witch moth’ flew by the baby’s face. These things do not
really cause blindness, and as people get new information, many are leaving
these older beliefs behind.
We now know that child blindness is usually caused by poor
nutrition or infection, and that most blindness in children can be
prevented.
COMMON CAUSES OF BLINDNESS IN CHILDREN ARE:
1. ‘Dry eyes’ (xerophthalmia, or nutritional
blindness) is the most common cause of child blindness. It is especially common
in parts of Africa and Asia. It results when a child does not get enough vitamin
A, which occurs naturally in many fruits and vegetables (and also in milk,
meats, and eggs). ‘Dry eyes’ develops in children who are not
regularly fed any of these foods. It often appears or quickly gets worse when
these children get diarrhea or have measles, whooping cough, or
tuberculosis. It is much more common in children who are not breast-fed.
Dry eyes can be prevented by feeding children foods with
vitamin A. Encourage families to grow and eat things like papaya, squash,
carrots, and leafy green vegetables in a family garden. Be sure the child
eats these foods regularly, beginning at 4 to 6 months old.
Vitamin A capsules can also prevent dry eyes, but should not
take the place of a well-balanced diet. Give 200,000 units (60 mg. retinol) once
every 6 months (or 100,000 units to babies less than 1 year old). Do not give
this large dose more often than 6 months, because too much vitamin A can
poison the child. For treatment, give 200,000 units (I.U.) of vitamin
A at once, 200,000 I.U. the next day, and 200,000 I.U. 2 weeks later. Give half
the dose to children under age 1. See a health worker.
|
SIGNS OF XEROPHTHALMIA
First sign may be night blindness. Child sees worse than others
in the dark.

Figure
Next the eyes look ‘dry’. The white part loses its
shine, begins to wrinkle, and forms patches of little gray bubbles (Bitot’s
spots). (1)

Figure
Later, the dark part (cornea) also gets dry and dull, with
little pits. (2)

Figure
Finally, the cornea may get soft, bulge, or burst, causing
blindness. (3)

Figure
FOODS THAT HELP PREVENT IT
· breast
milk
· dark green, leafy vegetables
· yellow, red, or orange vegetables
· whole milk
· egg
yolks
· liver and kidneys
· fish

Figure
|
2. Trachoma is the commonest cause of preventable
blindness in the world. It often begins in children and may last for months or
years. If not treated early, it can cause blindness. It is spread by touch or
flies and is most common in poor crowded living conditions.
Trachoma can often be prevented by keeping the child’s eyes
clean and keeping flies away. To prevent blindness from trachoma, treat early
with tetracycline eye ointment (see a health worker, or Where There Is No
Doctor).

Figure
|
SIGNS OF TRACHOMA
· begins like ‘red
eye’ with red, watery, sore eyes. Or in children it may develop for months
with few or no early signs.
· After a month or more small
lumps form inside the upper eyelids. (1)
· White of the eye becomes
inflamed or swollen. (2)

Figure
· Top edge of the cornea may
look cloudy. (1)

Figure
· After years the lumps inside
eyelids begin to go away, leaving whitish scars.

Figure
· The scars may pull the
eyelashes down into the eye, scratching the cornea and leading to blindness.
|
3. Gonorrhea in the eyes of newborn babies causes
blindness if not treated immediately. The baby gets the infection from his
mother at birth. The eyes get red, swell, and have a lot of pus. It can be
prevented by putting tetracycline eye ointment or a drop of 1% silver nitrate
solution in the eyes of all babies at birth. Gonorrhea,
which is a very common venereal (sexually spread) disease, can sometimes be
treated with penicillin (see Where There Is No Doctor).

Figure
4. ‘Chlamydia’ is a venereal disease caused by
the same virus as trachoma. It is similar to gonorrhea, both in the genitals and
the eyes, and is rapidly spreading worldwide. Putting tetracycline ointment in
the eyes of a newborn baby 3 times a day for 3 days usually prevents eye damage
from both gonorrhea and chlamydia.

Figure
5. River blindness (onchocerciasis) is a very common
cause of blindness in parts of Africa and Latin America. (See Where There
Is No Doctor.) It is spread by a kind of black fly that breeds in rivers
and streams. There is no cure.

Figure
6. Measles, which can injure the surface of the eyes, is
a common cause of blindness, especially in Africa and in children who are poorly
nourished.
7. Brain damage causes blindness in many children,
usually in combination with cerebral palsy or other disabilities. Brain damage
can happen before, during, or after birth. Causes include German measles during
pregnancy, delayed breathing at birth, and meningitis.
8. Eye injuries often cause blindness in children.
Pointed tools, fireworks, acid, lye, and homemade bombs to dynamite fish are
common causes.

Running with a pointed object is
DANGEROUS TO THE EYES.
9. Also, blindness in children is sometimes caused by other
problems such as hydrocephalus, arthritis, leprosy, brain tumors, or certain
medicines. Cataracts (clouding of the lens inside the eye) gradually develop in
about half of older children with Down Syndrome.
|
WARNING ON USE OF EYE MEDICINES
Only use modern medicines or ‘home cures’ that you are
sure cannot damage the eyes.
One modern medicine that should not be used often, and only with
great caution, is corticosteroid eye ointment. Some doctors and health
workers prescribe it for almost any eye irritation. This is a dangerous
mistake. If the irritation is caused by a virus (tiny
germ), this ointment could make the infection worse and lead to eye damage or
blindness!*
*Note: Corticosteroid drops or
ointment are important medicine for preventing blindness from iritis (see
“Arthritis” and “Leprosy”). But tests with
‘fluorescein’ should be done first to be sure there is not a virus
infection. Get medical advice.
Some ‘home cures’ for eye problems are safe and
effective. For example, in Mexico when villagers get a small piece of dirt
or sand in the eye, to remove it they put a wet chia seed under the
eyelid. The smooth seed has a layer of sticky mucus on it, to which the dirt
sticks. Then they remove the seed. This is a safe, good home cure.
chia seeds-a helpful home
cure
Some home cures are dangerous. Some villagers try to
treat ‘blurred vision’ by putting human feces (shit) around the eye.
This is unsafe and does not help. It could lead to dangerous infection. It is
also dangerous to put lemon juice, urine, pieces of abalone shell, or Vicks
ointment in the eye.

putting feces around the eye - a
dangerous home cure
|
What is the future for a blind child?
With help and encouragement from family and community, a child
who is blind can usually develop early skills as quickly and as well as other
children. He can learn to feed, bathe, dress, and care for himself, and to find
his way around the home and village without help. Although he cannot see well,
he develops an outstanding ability to use his sense of hearing, touch, and
even smell. If he can see at all, he can be helped to make the best use of
whatever vision he has. He can and should go to school. Although he may not be
able to read ordinary writing, he can develop his memory.
As he grows up, he can become a farmer, or a craftsperson. And
if he has the opportunity for training, he can learn any of a wide variety of
skills. Where blind persons are given a fair chance, they often take active part
in their communities and can live full, happy lives. In many countries, blind
people have been leaders in organizing disabled persons to become more
self-reliant and to work toward their rightful place in society.
Unfortunately, blind children often are not given a chance to
develop as quickly or as fully as they could. In some countries more than half
of the children who are born blind die of hunger or neglect before they are 5
years old. On the next page are 2 stories of blind children that will help you
realize the difference that understanding and help from family and community can
make.
|
SHANTI*
* Story adapted from How To Raise a Blind
Child.
Shanti is a little blind girl, who was born in a small village
in India. When they found that she was blind, her parents and grandparents tried
to hide the fact from the other villagers. They thought all blindness was sent
to a family as a punishment for sin, and that people would look down on them.
Secretly her parents took Shanti to an orphanage and left her
there.
Nobody in the orphanage had ever cared for a blind child, and
they did not know what to do. There were so many other children who needed care,
that there was no time left for her.
Shanti was kept alive, but that was all. Nobody talked to her or
held her lovingly or tried to stimulate her. Her blind eyes made the nurses
think she could not understand or recognize anything around her. So when other
babies began to reach out for objects they saw, and then to crawl toward things
they wanted, Shanti was left lying silently on her cot.
People got used to the blind child. She was picked up when
necessary, and cleaned and fed. They fed her with a bottle, or pushed food into
her mouth. But nobody tried to teach her how to feed herself or how to walk and
talk.
As she grew older, Shanti spent most of her time sitting on the
doorstep, rocking herself and poking her eyes. She never said a word and only
cried when she was hungry. Other children stayed away from her; they were afraid
of her dead eyes. Everyone thought she was mentally retarded and that nothing
could be done about it.

Figure
In time, Shanti did begin to talk and walk. But the sad, stony
look on her face never disappeared. Now, at age 7 she is in some ways still like
a 2-year-old. And in other ways she is no longer a child. We can only guess at
her future. |
RANI
Rani is also a little blind girl, born in another village in
India. Like Shanti’s family, when her parents learned she was blind, they
were worried about what the villagers would say. But the baby’s
grandmother, who had slowly lost her sight 5 years ago, said, “I think we
should do everything we can for the baby. Look at me. I, too, am now blind, and
yet I still have all the same feelings and needs as I did when I could see. And
I can still do most of the things I used to do. I still bring water from the
well, grind the rice, milk the goats,...”
“But you could already do all those things before you went
blind,” said the father. “How could a blind baby learn?”
“We must help her learn,” said Grandma. “Just as
I’ve learned to do things by sound and touch, so Rani must learn. I can
help teach her, since I know what it’s like. But we can also get advice
from the health worker.”
The village health worker came the next day. She did not know
much about blindness, but she knew a little about early child development. She
suggested they give the baby a lot of stimulation in hearing and feeling and
smelling things, to make up for what she could not see. “And talk to her a
lot,” she said.
The family took the advice. They put all kinds of things in
Rani’s hands and told her what they were. They gave her bells and
squeakers, and cans and bottles to bang on. Grandma, especially, took Rani with
her everywhere, and had her feel and listen to everything. She played games with
her and sang to her. At age 2, Grandma taught her to feel her way along the
walls and fence, just as she did. By age 3, Rani could find her own way to the
latrine and the well. When she was 4, the health worker talked with the
neighbors, and did some CHILD-to-child activities on blindness with their
children. After, a few children came to make friends and play with Rani.
Sometimes they would all blindfold their faces and try to find something or tell
different things apart. At these games, Rani usually won.
When she was 6, Rani started school. The neighbor children came
for her every day. When the villagers saw them all walking down the road
together, it was hard to guess which one was blind.

Figure
|
Early stimulation
As Rani’s grandmother realized, a child who is blind has
all the same needs as other children. She needs to be loved, not pitied. She
needs to get to know the members of the family, and other things, by touch,
sound, smell, and taste. The whole family can help her to become more aware of
her home, and the things that are going on around her.
|
A baby’s first plaything is her own body. Since she cannot
see her hands and feet move, you may need to help her to feel, taste, smell, and
explore them. |

Figure
|
Have him compare by touch and sound his own and other
people’s faces so that he begins to recognize different people. |
Figure
|
Activities to help a child develop early skills more quickly are
discussed in Chapter 35. Most of these activities can help a blind child. But
because he cannot see, he will need more stimulation in other areas,
especially sound and touch, and in beginning to reach toward things and move
about. Use toys and playthings that have many different shapes, feel
different to touch, and make different sounds.
|
At first you may need to place the toy in the child’s hand,
or guide his hand to it. Or hang different things near him so that when he moves
his hands they touch them. |

Figure
|
At each stage of the child’s development, attract her
attention with a noisy plaything. Have her reach for it and then try to move
toward it. |

Figure
Praise her when she does well or tries. |
In addition to special activities, be sure the child spends
most of each day in a situation where she can keep learning about people and
things. In everything you do, talk to her, tell her the names of
things, and explain what you and she are doing. At first she will not
understand, but your voice will let her know you are near. Listening to words
and names of things will also prepare her for learning language skills.
|
Talk to the child as you do housework. Tell her what makes the
sound she hears. |
Sing to the child and encourage him to move to music.
Also encourage blind children to make their own music. |
Figure
|
|
Figure
|
Figure
For ideas on homemade musical instruments. |
Take the child outside often: to the market, the river, the
cowshed, the village square. Show and explain different things to him, and tell
him what makes different sounds. |
For a blind child, it is important that special help and
stimulation start early - in the first months of life. Without this the
child will fall far behind in her development. She may become quiet, not do
much, and be afraid to move about. So her family does not expect much of her, or
provide many learning opportunities. As a result, she falls still farther
behind.
However, if a blind child has the stimulation and help she
needs from an early age, she will develop many skills as quickly, or nearly as
quickly, as a child who sees. So her family expects more of her and includes
her more in their activities. As a result, she may develop almost as quickly as
other children her age. She can probably enter school when they do.
Helping the blind child learn to move about
The child who is blind often is slow at learning to move about
and will need extra help and encouragement. Some of the activities in Chapter 35
for creeping, crawling, standing, and walking will help. Here are some other
suggestions.
|
When the child is beginning to scoot or crawl, you can leave
toys and other interesting things in different places where he will find them.
This will encourage him to explore and discover. |

Figure
|
But when the child begins to walk, try to keep everything in its
place, so that she does not bump into things unexpectedly and can gain more
confidence moving about. If you change the position of something, show her where
it is. |

Figure
|
|
Play games and do exercises that will help the child gain
confidence in moving and using his body |

Figure
|

Figure
|
Encourage the child to make adventure, explore, and do all the
things a child normally does. Protect her from hurting herself - but do not
protect her too much. Remember, all children learning to walk sometimes fall. A
blind child is no different.
|
Figure
|

Figure
|
Figure
|
Help the child find his way by following walls and fences. |
|
The child can learn to feel the edge of the path with her feet,
ana to feel plants or other objects with her hands. |

Figure
|
If the child does not start walking without help, let him start
by pushing a simple walker, chair, or cart.
Do not force the blind child to walk alone before he is ready.
One day he will start walking alone, first a few steps only, but finally with
confidence. |

Figure
|
Helping the blind child find her way without holding on
Outside the home, often a blind child will let you lead her by
the hand, but may be afraid to take steps or try to find her way alone.
To help her begin to walk alone, first lead her over the area
where you want her to walk. Show her and let her feel the different landmarks
(posts, trees, bushes, houses) along the way.
|
A good way to guide a child by the hand is to let her hold one
finger and walk a step behind you. |
Now walk over the same path, but this time walk backward in
front of her, and talk to her while you are walking. |
When she feels comfortable with your walking in front of her,
start walking behind her. Have her tell you the landmarks. |
|

Figure
|
Figure
|

Figure
|
Little by little make yourself less and less needed. Speak less
and let her go farther away from you.
Finally let her go the whole way alone. Start by having her walk
short distances. Then gradually go farther, with more turns and other things to
remember.
When she has progressed this far, the child will have the joy of
knowing she can solve some problems alone. She will be ready to learn new
things, meet other difficulties, and explore new areas.
|

Figure
|
Sometimes the child will fall. Have her practice this by falling
on soft ground. Teach her to put out her hands and bend her knees as she falls.
She will be less likely to hurt herself. |

Figure
|
|
The child needs to learn to ‘see’ with her feet, and
to be prepared for unexpected things in her way. Play games with her. Tell her
you have put some things in her path. See if she can get past them without
slipping or falling. |
Figure
|
Help the child to recognize how the sound of her footsteps (or
her stick) changes when she is near a house or wall and when there is open
space. With practice, she can learn to tell the distance from things by the
sounds. |
Learning to use a stick
Using a long stick can help a child find his way and give him
more confidence, especially for walking in places he is not familiar with. With
practice, it can also help him to walk in a faster, more normal way, with long,
sure steps. This is because he can feel farther ahead of him with his stick than
with his feet. The best age to start teaching a child to use a stick is probably
about 6 or 7.
|
The stick should be thin and light, and tall enough so that it
reaches half way between the child’s waist and shoulders. The top of the
cane can be curved or straight. |
Figure
|
At first just give the child the stick and have him lightly
touch the ground in front of him as he walks. His arm should be straight.
Play games letting him feel his way. But do not hurry him. Stop
before he gets tired of it. At first, 5 or 10 minutes is enough.
After he gets used to the stick, walk beside him and encourage
him to take smooth, even steps.
Have him swing the stick from side to side, and see if he can
find things in his path. |

Figure
|
After a time he can learn to use the stick better:
|
Move the stick from side to side, lightly touching the ground.
The width of the swing should be a little more than the width of
his shoulders.
As the stick touches to one side, move the foot on the other
side forward. |

Figure
|
On a narrow path or rough ground, someone can lead the child by
the stick.
Or the child can hold the person’s elbow or wrist. |
Figure
|
|
The child can learn to feel the height of steps and curbs, and
then to climb them. |
To go up steps, it is better to hold the stick like this to feel
the position of each step.

CORRECT
|
WRONG
|
Do not hold it like this. This can cause the cane to stop
suddenly and hit the child in the stomach. |
|

Figure
|
Putting posts or other marking where roads or paths cross can
help the child find his way or know where to turn. (1) |
Figure
|
|
Teach the child to listen carefully before he crosses a path or
road where cars or other traffic pass. |
But whenever possible, teach him to find his way using
‘landmarks’ that are already there. |
Sometimes putting a guide rope or rail can help the child find
his way. |
Helping the blind child to use his hands and to learn
skills
Help the child who cannot see well to do all kinds of things
with her hands, including daily care of herself: eating, dressing, bathing, and
toileting. Ideas for learning these skills are in Chapters 36 to 39.
|
At first you may need to help the child feel things by guiding
his hands. |

Figure
|

Figure
|
|

Figure
|
To help the child know where to look for the different foods on
her plate, try to always put them in the same place. As the child gets older and
learns to tell time, have her think of the plate or bowl as a clock. Tell her at
what time each type of food is put on her plate. Here the glass of water is at 2
o’clock. Always put it at 2 o’clock. |
|
Help the child learn to put in the same place glasses,
cups, bottles, and other things that can be easily spilled or broken. Teach her
to remember where she puts things, and learn how to reach out for something and
find it without knocking it over. Reaching out with the back of the hand
causes less spilling. (This will take practice and there will be accidents,
but that is the way she learns. Do not hand her everything or do everything for
her, just to avoid a mess. Making a mess is part of learning.) (1) |

Figure
|
|

Figure
|
Help the child learn to recognize different shapes, sizes, and
the ‘feel of things’ with her fingers. Let her play with toys and
puzzles so that she learns to put different pieces together in a certain pattern
or order. Ideas for toys and puzzles are. |
Teach the child about things he must be careful with or keep a
distance from, to not get hurt: things such as fire, hot pans and dishes, sharp
knives, dogs and mules that might bite or kick, deep holes, wells, cliffs, deep
ponds or rivers. Do not just tell him “No!” Help him to understand the
danger.

Figure
|
CAUTION: Whenever possible, keep dangerous things out
of reach or put fences around them, and take other precautions to protect the
child - especially until he is old enough to be careful. |
|
Give the child opportunities to begin to help in
different ways around the house. This will both increase her skills and give
her a sense of being part of the life and action of the family. |
Figure
Abdul helps rock his baby brother. |
Rani’s mother teaches her how to cook by guiding her hand
and explaining each step. |

Figure
|
When the child has learned to handle bigger things fairly well,
help her learn to feel and handle smaller things. For example:
|
She can help sister pick the little stones and bits of dirt out
of the rice. |

Figure
|
If someone takes the time to teach him, a child can begin to
help in a lot of things around the home, and also in village crafts. Weaving of
mats, rugs, clothing, and baskets are things many blind children can learn to do
well, and it helps them learn to use their hands skillfully.
Figure
|
Also, look for games and toys that help the child develop her
ability to feel fine details and small shapes with her fingers.
|

Figure
|
For example, you can make dominos and dice out of wood. For the
dots, hammer round-headed nails into the wood, so she can feel them. Or drill
holes.
The child can learn to feel the dots with her fingertips. At the
same time, she will begin to learn to count and use numbers.
You can start with ‘giant’ dominos and dice, and when
her fingers learn to feel more skillfully, change to small ones. This will be
good preparation for doing many kinds of fine work and perhaps for learning to
read braille. |
SCHOOL
Blind children should have the same opportunity as other
children to go to school. Ideas for how children in the community can help a
blind child get to school, and help her in the classroom and with her studies
are discussed in the CHILD-to-child activity on blindness.
In most countries there are special schools that teach blind
children to read and write ‘braille’. Braille is a system of
raised dots that represent letters and can be read with the fingertips. It was
invented many years ago by a blind boy from France named Louis Braille.
Most village children do not learn braille in school. However,
there are many other ways that they can learn in school.
For the blind village schoolchild, one of the best aids for
taking notes and reviewing lessons is a small tape recorder. The family
should try to save money to buy one. Or perhaps the schoolchildren can hold a
raffle or collect money to buy one. Other children can help record lessons from
school books, and stories and information from other books.

Figure
|
THE BRAILLE ALPHABET

Figure
Louis Braille invented this dot alphabet at age 14. The dots are
pressed into a thick paper from the opposite side with a pointed tool called a
‘stylus’. |
|
IMPORTANT: In order to keep up with her
studies a blind child will need help. In school another child can read to her
from her books. The child may also need extra help after school. An older
brother or sister, or another schoolchild, can perhaps spend time teaching her
at home. |
Remember, most ‘blind’ children have some useful
vision. Encourage the child to use whatever sight she has. If she can see
big letters on the blackboard, write big and clear, and be sure she sits in the
front. Be sure the light is good, and that dark letters and things stand out
against a light background.
|
If she can see at all, to help her learn the letters, make them
very BIG. Use white paper and dark ink. |

Figure
|
To help the child learn the shape of letters by feel, you could
make them in one of these ways. |
|
|

Figure
|

Figure
|

Figure
|

Figure
|
|
|
rope glued or pinned to wood or cardboard |
grooves cut into wood |
letter cut out of cardboard and glued to thick paper
|
letter in plaster or clay |
|

Figure
In the schoolroom, a pan with soft clay or mud is
helpful for learning to write and feel letters. |
Figure
Children can practice writing outside in sand, mud, or
clay. |

board with string stretched
through holes
When the child begins to write, you can stretch string lines
across the paper to help her write in straight lines. Or draw extra dark lines.
|
|
To help the child begin to count you can make a simple
‘counting frame’. The child can slide the beads or rings from
one side to the other to count, add, and subtract. |
When the child becomes more skilled with numbers, she can learn
to use a special counting frame called an ‘abacus’ which has
beads on wires. The beads slide up and down to form numbers. With practice, a
blind child can learn to add and subtract on the abacus as fast or faster than
other children can do it on paper. |
|

Figure
|
|
|
A pegboard like this can help a child learn numbers through
touch - and help him learn to feel small differences in things. |
Figure
|
AN ABACUS

Figure
|
(All the beads are really the same color. Here we have made some
black to make it clearer how to count.) |
Work
As a blind child grows up, he or she can learn to do many
different kinds of work. On page 509 in Chapter 54 we list many of the different
kinds of work that disabled persons can do. Those types of work marked with a *
have often been done by blind persons.
The village child who is blind should be given many
opportunities to help with work around the home and with farm work. The blind
child should be invited and expected to help in a wide range of daily
activities, just like the child who can see. What starts out as play and
imitation ends up as learning of useful skills.
A family that farms the land can begin to include a blind child
in gardening and farming activities from an early age.
|

Figure
|
Figure
|
|
To get an understanding of the whole process of growing the
family food, the child can start by planting seeds, watering them, caring for
them as they grow, and finally harvesting, cooking, and eating the product.
|
Later, the child can go with his father or mother to the fields
and help with the planting. With his feet he can follow the furrows, or grooves
made by the plow. |
Try to involve the child with each aspect of housework and farm
work. At first show her and guide her as much as is necessary. Then help less
and less until finally the child can do the whole job alone.
Social life
The blind child should have all the same opportunities in the
community as other children do. Take her with you, and then send her, to the
market, well, river, school, and temple. Introduce her to the people you meet.
Explain to them that she is an active little girl like any other, except that
she cannot see. Ask them, when they see her, to make a point of speaking to her
(since she cannot see them), of answering her questions, of helping her to find
what she is looking for. Ask them not to do everything for her, but
instead to help her figure out how to do more for herself. Little by little
people will begin to realize that a blind child can do a lot more than they
would ever have dreamed possible. And they will begin to respect and appreciate
her. For the next blind child in the village, it will be easier.
Take the child to meetings, movies, puppet shows, and town
events. Explain to her what she cannot see.
When children who are blind grow up, they can marry and have
children. They can be as good parents as persons who see.
PREVENTION of blindness
The best way to prevent blindness is to try to keep children
well fed, clean, and healthy. During pregnancy, mothers also need to eat
enough nutritious foods and to avoid medicines that might damage the baby.
Specific steps to prevent some causes of blindness have already been discussed.
In brief, steps to prevent child blindness include:
· When pregnant,
keep away from persons with German measles and other infectious diseases, avoid
unsafe medicines, and try to get enough to eat.
· Protect the eyes of all
newborn babies with tetracycline eye ointment or 1% silver nitrate drops at
birth.
· Vaccinate
children against all the infectious diseases you can.
· Breast feed the baby, and
continue to breast feed as long as possible.
· Good nutrition for mother and
child - especially foods rich in vitamin A. Children often get diarrhea and then
‘dry eyes’ after they are taken off the breast. So, when the baby
starts to eat other foods, give him mashed papaya, mashed cassava leaves, or
other foods with vitamin A, every day.
· Keep the home and child clean.
Build and use latrines, and keep them covered. Try to protect against flies.
Wash hands with soap and water, especially before eating and after using the
latrine (toilet).
· Keep the child’s eyes
clean. When they get infected or have pus, clean them often with a clean cloth
that is wet with clean water, and see a health worker.
· Give children with measles
vitamin A rich foods (or vitamin A capsules) because danger of ‘dry
eyes’ increases with measles.
· Treat all persons with signs
of trachoma early. For treatment of different eye problems, see a health worker
or get information from a book like Where There Is No Doctor.
· Keep sharp and pointed
objects, bullets, explosives, acids, and lye away from children and teach them
about their dangers. Warn them about the danger of throwing closed bottles,
cans, or bullets into the fire. Also warn them about local plants that can
injure the eyes. (For example, the juice of ‘hiza’, a poisonous fig
tree in Mexico, can burn the eyes like lye.) Get good early treatment for any
eye injury.
· Warn children about throwing
rocks and sticks, or shooting slingshots toward other persons.
· Check babies and children for
early signs of eye problems or difficulty seeing. Test how well they can see at
2 months of age and before they begin school.
· Organize children to test the
sight of their younger brothers and sisters (see CHILD-to-child).

Figure
· Help everybody
understand that most blindness in children can be prevented. Teach people
what they can do.
· For special precautions to
protect the eyes of persons who have a loss of feeling in their eyes, see
Chapter 26 on
Leprosy.
Chapter 31: Deafness and Communication
Different children have different amounts of hearing loss
A few children are completely deaf; they do not hear at
all. Parents often notice early that their child cannot hear, because she does
not turn her head or respond, even to loud sounds.
Much more often, children are partly deaf. A child may
show surprise or turn her head to a loud noise, but not to softer noises. She
may respond to a low-pitched sound like thunder, a drum, or a cow’s
‘moo’, but not to high-pitched sounds like a whistle or a rooster
crowing. Or (less commonly) a child may respond to high-pitched sounds but not
low ones.
Some children who are partly deaf hear a little when people
speak to them. They may slowly learn to recognize and respond to some words. But
many words they do not hear clearly enough to understand. They are slow to begin
to speak. Often they do not speak clearly, mix up certain sounds, or seem to
‘talk through their nose’. Unfortunately, sometimes parents, other
children, and teachers do not realize that the child has difficulty hearing.
They may treat her as if she is mentally slow, or
‘dumb’. This only increases the child’s problems.

The child who is completely deaf
does not respond even to very loud noises. (But he may notice movements or
vibrations caused by sudden loud noises. For example, clapping behind the
child’s head may move the air at his neck and cause the child to turn.)

The child who is only partly deaf
hears some sounds, but may not hear clearly enough to tell the difference
between certain sounds or words. Families are often slow to recognize that these
children have difficulty hearing.
Problems that may result
For most growing children, hearing and language are very
important for getting to know, understand, and relate to the people and things
around them.
|
COMMUNICATION is the way in which we understand what is
said to us and the way we say or express to other people our thoughts,
needs, and feelings. People who can hear communicate mostly through
speech. |
For a child with a hearing loss, the biggest problem is
learning to communicate. Because she cannot hear words clearly, it is
much more difficult for her to learn to speak. So she has trouble both
understanding what people want, and telling them what she wants. This can lead
to frequent disappointments and misunderstandings, both for the child and
others. It is no surprise, then, that children with hearing loss sometimes are
slow in learning to relate to other people, feel lonely or forgotten,
or develop ‘behavior problems’.
The exchange of ideas and information through some form of
communication is important for the development of any child’s mind. Most
deaf children are just as intelligent as other children. But for their mental
ability to develop fully, they need to learn to communicate well from an early
age.
How deafness affects a child depends on:
1. when the child became deaf. For a child
who is born deaf or becomes deaf before he begins to speak, learning to speak or
‘read lips’ will be far more difficult than for a child who loses his
hearing after he has begun to speak.
2. how much the child still hears. The better the
child hears, the more chance he has of learning to speak, understand speech, and
‘read lips’.
3. other disabilities. Some deaf children also have other
problems. A child who is mentally retarded, blind, or
‘multiply disabled’ will have a harder time learning to
communicate than a child who is deaf only. (See “Causes of Deafness.”)
4. how soon the problem is recognized.
5. how well the child is accepted, and how early he is helped
to learn other ways to communicate.
6. the system of communication that is taught to the
child (‘oral’ or ‘total’).
|
CAUSES OF DEAFNESS
Deafness is not caused because the child did
something wrong or because someone is being punished.
Common causes before a baby is born:
· hereditary
(occurs in certain families, although the parents themselves may not be
deaf). Usually a child has no other disability, and learns quickly.
· German measles during
early pregnancy. Often child also has brain damage and learning problems.
· Rh factor. Child often
has other disabilities also.
· Prematurity (born early
and small). Two out of 3 have other disabilities also.
· lack of iodine in
mother’s diet (common in areas where many people have goiters). May show
signs of mental retardation or cretinism.
· certain medicines
taken by the mother while pregnant, such as corticosteroids and phenytoin.
· difficult birth, baby slow to
breathe.
· dwarfism and brittle bone
disease.
Common causes after birth:
· ear infections
- especially long-lasting repeated infections with
pus.

Figure
· meningitis
(often child has other disabilities and behavioral
problems).
· certain medicines
(streptomycin, and related antibiotics).
· frequent very loud noise.
Other causes. There are many other less common causes of
deafness. In 1 out of 3 children the cause is not known. |
Importance of early recognition of deafness
During the first years of life, a child’s mind is like a
sponge; it learns language very quickly. If a child’s hearing problem is
not recognized early and effective help is not provided, the best years for
learning communication skills may be lost (age 0 to 7). The earlier special
training begins, the more a child can learn to communicate.
Parents should watch carefully for signs that show if a baby
hears or not. Does the baby show surprise or blink when you make a sudden
loud noise? As the baby grows, does he turn his head or smile when he hears
familiar voices? Has he begun to say a few words by 18 months of age? Does he
say a lot of words fairly clearly by age 3 or 4? If not, he may have a hearing
problem. As soon as you suspect a problem, test the child’s hearing.
Simple tests for hearing. If it seems the child does not
hear well, when possible, take him to a specialist for testing.
Unless a child is given a lot of understanding and help learning
to communicate from an early age, deafness can be one of the most difficult,
lonely, and misunderstood disabilities. The following 2 stories will help
show the difference that it can make to recognize a hearing problem early and
provide the extra help that the child needs.
|
TONIO
Although Tonio was born with a severe hearing loss, his
parents did not realize this until he was 4 years old. For a long time, they
thought he was just slow. Or stubborn.
Until he was one year old, Tonio seemed to be doing fairly well.
He began to walk and play with things. Then his sister, Lota, was born. Lota
smiled and laughed more than Tonio when their mother talked or sang to her. So
their mother talked and sang to Lota more.
By the time Lota was 1, she was already beginning to say a few
words. Tonio had not yet begun to speak. “Are you sure he can hear?” a
neighbor asked one day. “Oh yes,” said his mother. She called his name
loudly, and Tonio turned his head.
When he was 3, Tonio could only say 2 or 3 words. Lota, at age
2, now spoke more than 200 words. She asked for things, sang simple songs, and
played happily with other children. Tonio was more moody. Mostly he played by
himself. When he played with other children it often ended in fighting-or
crying.
Lota behaved better than Tonio. Usually, when her mother told
her not to do something and why, she understood and obeyed. Often, to make Tonio
obey, his mother would slap him.
One time in the village market Lota asked for a banana and her
mother bought her one. A moment later, Tonio quietly picked up a mango and began
to eat it. His mother slapped him. Tonio threw himself on the ground and began
to kick and scream.
When Tonio’s father heard what had happened in the market,
he looked angrily at Tonio and said, “When will you learn to ask for
things? You’re 4 years old and still don’t even try to talk. Are you
stupid, or just lazy?”

Figure
Tonio just looked at his father. Tears rolled down his cheeks.
He could not understand what his father said. But he understood the angry look.
His father softened and took him in his arms.
Tonio’s behavior got worse and worse. At age 4 his mother
took him to a health worker, who tested Tonio and found that he was deaf.
Now Tonio’s parents are trying to make up for lost time.
They try to speak to him clearly and slowly, in good light, and to use some
signs and gestures with their hands to help him understand. Tonio seems a little
happier and speaks a few more words. But he still has a lot of trouble saying
what he wants. |
SANDRA
When Sandra was 10 months old, her 7-year-old brother, Lino,
learned about testing for deafness as part of the CHILD-to-child program at
school. So he tested his baby sister. When he stood behind her and called her
name or rang a bell, she did not turn or even blink. Only when he hit a pan hard
did she show surprise. He told his parents he thought Sandra did not hear well.
They took Sandra to a small rehabilitation center. A worker there tested Sandra
and agreed she had a severe hearing loss.
The village worker explained what the family could do to help
Sandra develop and learn to communicate. He gave them many drawings of hands
held to make ‘signs’ for common words.
“Every time you speak, make ‘signs’ with your
hands to show what you mean. Include all the signs and gestures that people
already use in your village. Teach all the children to use them too. Make a game
out of it. At first Sandra won’t understand. But she’ll watch and
learn. In time she’ll begin to use signs herself”
“If she gets used to signs, won’t that keep her from
learning to speak?” asked her father.
“No,” said the worker. “Not if you always speak
the words at the same time. The signs will help her understand the words, and
she may even learn to speak earlier. But it takes years to learn to speak with
‘lip reading’. First, she needs to learn to use signs to say what she
wants and to develop her mind.”
Sandra’s family began using signs as they spoke to each
other. Months passed, and still Sandra did not begin to speak or to make signs.
But now she was watching more closely.
By age 3, Sandra began to make signs. By age 4 she could say and
understand many things with signs-even lip read a few words, like
‘Yes’, ‘No’, and ‘Lino’. By age 5 she had only
learned to ‘lip read’ a few words. But with signs she could say over 1
000 words and many simple sentences.
Figure
Sandra was happy and active. She liked to color pictures and
play guessing games. Lino began to teach her how to draw letters. One day she
asked Lino when she could go to school. |
WHERE CAN YOU GO FOR HELP?
A child who does not hear well needs extra help. Where you can
look for help depends on where you live and on what resources are in your
community and in your country. Here are some possibilities:
· Local deaf
persons as teachers. Even a small village usually has some persons who have
been deaf a long time. Probably they will have learned to communicate through
signs and gestures. If you ask some of them to become the friends and teachers
of a deaf child, and advisers to the family, often they will be glad to do so.
They may remember the difficulties and loneliness of their own childhood and
want to help provide the understanding and learning opportunities that the deaf
child needs.
Deaf persons can be especially helpful if they have learned the
‘national sign language’ and can communicate fully with other deaf
persons. If there is no such person in your village, but there is in a
neighboring town, perhaps the child can visit that person, or a group of deaf
persons.

Deaf persons who have learned to
communicate well are often the best teachers of a deaf child and his family.
· Other families
with deaf children. If several families with a deaf child can come together,
share experiences, and learn as a group, this can be a big help. The younger
deaf children can learn from older ones, or from deaf adults. Together they can
develop a form of communication so that all the children and their families can
understand each other.
· The National Association of
the Deaf (or other group run by the deaf). Most countries have
associations of deaf persons. These can give you information about the national
sign language in your country, and perhaps send books for learning it. They can
tell you about training programs for the deaf (government, private, and
religious) and can advise which are the best. They may even provide brief
training in basic communication skills to a local health worker, teacher, family
member, or disabled child - with the understanding that he or she then teach
others.
· ‘Special
education’ programs or schools for the deaf. Many countries have
schools where deaf children can live and receive special training. Some of these
are good and some are not. Good programs try different methods of communication
with each child and then focus on what will probably work best for that child in
his community. Bad programs try to make all deaf children communicate only by
lip reading or speech. For many children this can lead to failure, anger, and
emotional harm. Try to get advice from educated deaf persons.
At first it may be difficult for parents to let their child go
away to school. But learning to communicate well can be important to the
child’s life. Be sure to check the costs and plan ahead. Some schools may
be free or have low fees.
Deciding what to do for a deaf child
Not all children with hearing loss are the same. All need love,
understanding, and help learning to communicate. But different children need
different kinds of help, to communicate in whatever way works best for them. We
must adapt our methods to the needs of the particular child and to the realities
of the community where he lives.
· If a child is only
partly deaf, sometimes we can help her to hear more clearly, to
understand more speech, and perhaps learn to speak.
· A child who has no hearing
at all usually cannot be helped to hear. But if he became deaf after he
began to speak, perhaps he can be helped to ‘read’ people’s
lips and to improve his speech.
· If the child was born deaf
and has never heard speech, learning to lip read and speak is always very
slow and difficult, and is usually not very successful. It is better to help the
child learn to communicate in whatever ways work best for her: first with her
face, body, arms and hands, then possibly adding pictures, reading and writing,
finger spelling, and as much lip reading and speech as she is able to learn.
· If the child comes from an
area where there are many deaf people who communicate with each other in
a national sign language, it is probably best to have people in the deaf
community help teach the child and her family their language. That way, she can
learn to communicate with deaf people as fully and well as hearing people
communicate with each other.
· But if the child lives in a
small village where there are few deaf people, none of whom know the
national sign language, learning that language may not help the child much.
Probably it makes more sense for her to learn ways to communicate as best she
can with those who can hear. Again, this probably means a combination of
methods, based on the signs and gestures people already use in the village. With
these, the child can also use pictures, and later perhaps, reading and writing.
· Remember, most children with
hearing loss can learn quickly. But some may have brain damage or disabilities
that affect their ability to learn or to control their hands, lips, or voices.
You will need to figure out ways to help these children communicate in whatever
way they can: with sets of pictures, head movements, or eye
movements.
|
Note: Some children who hear perfectly well
do not develop the ability to speak. Some children with cerebral palsy do not
control their mouth or tongue movement well enough to speak. Other children are
mentally retarded and may be very late in learning to speak, or never learn.
Other children are intelligent in many ways, but for some reason cannot speak.
For all of these children, we need to look for ways to help them communicate as
best they can. |
Helping a child to hear better
Children who are not completely deaf can sometimes be helped to
hear better:
· When possible,
have the child’s hearing and ears examined by a specialist. A few children
are born with a closed ear tube or other defect in the structure of the ear.
Rarely these problems can be corrected by surgery, and the children
can hear better. (Note: For children whose hearing loss
comes from brain damage, surgery will not help.)
· Children who have hearing loss
because of ear infections may begin to hear better if the ear infections
are treated early and steps are taken to prevent more infections.
· Some children can hear better
with aids that make sounds louder. A ‘hearing aid’ allows some
children to understand words fairly well, and can make a big difference in
learning to listen and speak. For other children, an aid makes them more aware
of sounds (which helps) but does not help them to tell the difference between
words. If it appears the child will benefit a lot from a hearing aid, it helps
to begin as early as age 1 or 2.
|
The simplest aid is a hand cupped behind the ear. |
Better is an ‘ear trumpet’. You can make one
out of a cow horn, cardboard, or tin. |
Better still (for some children) is a ‘hearing aid’
with batteries. But ear usually these are very expensive. For best
results, it should be fitted by a specially-trained worker after the
child’s hearing has been carefully tested. |

Figure
|
|

Figure
|

Figure
|

Figure
|
(1) microphone
(2) batteries
(3) Piece that fits into ear (best if molded to fit the specific
child). In a growing child it will need to be changed often. |
|
CAUTION: If you get a child a hearing aid,
be sure to ask for instructions on keeping it clean, dry, and working well. Be
sure you have a supply of extra batteries and know how to get more. |
· Young children who
do not hear well can sometimes be helped to listen more carefully, and to
learn the difference between sounds:
Make different sounds and encourage the child to take notice.
When a donkey brays or a baby cries, say clearly and loudly, “Listen to the
donkey,” or “What was it?” If the child answers or points in the
right direction, praise him.
Have the child make different sounds-hitting pans, drumming,
ringing bells, and so on. See if he can move or dance to the beat of music or
drums.

Figure
Talk a lot to the child. And sing to her. Tell her the name of
different parts of her body, and other things. Ask her to touch or point to
them. Praise her when she does.
Experiment to find out how near the child’s ear you need to
be, and how loud you have to speak, to get the child’s attention, or for
him to repeat the sounds you make. Then try to speak near and loud enough. Speak
clearly, but do not shout.

Figure
DIFFERENT WAYS TO HELP A CHILD COMMUNICATE
|
COMMUNICATION BY SHOWING

Figure
|
HELP WITH HEARING AND SPEAKING
Figure
|
|
LIP READING

Figure
|
COMMUNICATION BY PICTURES AND POINTING

Figure
|
FINGER SPELLING

Figure
|
|
READING AND WRITING

Figure
|
SIGN LANGUAGE
“Talking with the hands”
Figure
|
Oral communication
Oral communication (communication by mouth) combines helping a
child use her limited hearing as much as possible, with lip reading,
and with learning to speak. In many countries, schools for deaf
children teach only oral communication. Unfortunately, oral communication
usually only works well for children who can hear the differences between
many words, or for children who became deaf after they learned to speak.
Total communication
Total communication is an approach that encourages a child to
learn and use all the different methods that work well for that child in her
particular community. This might include any (or all) of these:
· the child’s
own gestures
· sign language
· drawing, reading, and writing
· finger spelling
·
whatever hearing the child has, to develop lip reading and speech
IMPORTANT: Total communication’ as we
use the term, does not mean that all the above methods are used for every child.
It means that we try all the methods that might work for a child. Then we
work with whatever methods will help the child communicate as easily,
quickly, and fully as possible with her family and community. It is an
approach that is friendly, flexible, and adaptable to individual and local
needs.
|
WARNING: Beware of programs that teach only oral
communication
In many countries, schools for the deaf still try to make all
children learn only ‘oral communication’ (lip reading and spoken
words). The results are often disappointing, or even harmful, especially for the
child who was born deaf. Lip reading at best gives a lot of problems. A skilled
lip reader can only understand about 40 to 50 percent of English words, and has
to guess at the rest. (For example, “Mama” and “Papa” look
exactly the same on the lips.) Even if the child does learn to lip read and
speak some, often his words are unclear or sound strange. As a result, when he
grows older, often he prefers not to speak.
The biggest problem with teaching only oral communication is
that it slows down a child’s language development at the age when children
learn language fastest (age 1 to 7 years). A deaf child usually learns to lip
read and speak only 5 or 10 words by age 5 or 6. By that age, the same child can
easily learn over 2,000 signs - as many words as a hearing child speaks.
Studies have shown that deaf children who learn to use
gestures and signs can communicate easier, earlier, and more fully than those
who are taught only oral communication. Learning sign language and other forms
of communication first actually makes it easier for a child to learn to speak
and read lips.
For all these reasons, more and more experts and
organizations of deaf people recommend teaching most deaf children a combination
of communication methods, including some form of sign language.
Total communication’ is not new. In villages in many parts
of the world, deaf and hearing persons find imaginative and effective ways to
talk with each other. They figure out a system of hand signs, objects, face
movements, pictures, and certain sounds or words. As a result, deaf persons
often manage fairly well in the community. They can “say” and
understand a lot.
We know families from villages like these who took their deaf
child to ‘speech therapists’ in the city. Often
the parents and child had already begun to communicate with each other by using
the local signs and inventing more of their own. The child was happy and
learning, fairly well. But the therapists told the parents that they were wrong.
They told them that they must not let the child use signs, because if he got
used to signs he would never learn to speak. They said the child should be put
in a ‘special education program’ and taught ‘oral
communication’. But since the only programs of this kind are in the cities
(and often have a 3-year waiting list) the parents took their child back to the
village. Trying to follow the therapist’s orders, they tried not to use
signs with their child, and punished him when he used them. As a result, both
the parents and child felt frustrated, guilty, angry, and hurt. The child’s
learning and social development were held back. His chances of learning to speak
became less than they were when everyone happily used the village system.
Fortunately, most of these families in time realized that they
simply could not manage without using signs, and gradually went back to
accepting ‘total communication’.
In the richer countries more and more special educators and
speech therapists are beginning to favor total communication. They have changed
to this approach partly because deaf persons have organized and demanded it.
Disabled persons in poor countries, including deaf persons and their
families, also need to organize. They need to help professionals listen to them,
and to respond to their needs in more realistic ways. |
Helping a child learn ‘total communication’
· The learning place
should be well lighted, so that the child can see your hands, face, and lips.
· Face the child when you speak
to her, and be sure she is watching you.
· Talk to her a lot, even if she
does not understand. Talk with your hands, face, and lips, and encourage her to
watch them all.
· Speak clear and loud, but
do not shout and do not exaggerate the movement of your mouth and
lips. This will help her learn to recognize normal speech.

Figure
· Be patient and
repeat things often.
· Be sure to let her know that
you are pleased when she says something or does something well.
· Encourage her to make whatever
sounds she can. This will help her strengthen her voice for possible speech.
· Have a lot of toys, pictures,
and other things ready to use in helping her learn the signs and words for them.
· Make learning to communicate
fun. Include other children in games like ‘Simon says’ that help
children use their eyes, ears, and bodies, and copy each other.
· Play games that exercise the
child’s lips, tongue, and mouth muscles. In a deaf
child, these muscles can get weak. This not only makes speech more difficult,
but can make the child’s face look dull, or without expression. For
activities to strengthen and control the mouth and lips.
· Make a list of the words that
other children her age use, and that you most want the child to learn.
Include:
|
· useful words for learning
and games: yes, no, thank you, please, what, do, don’t, like, want
|
· common and interesting
things: body parts, animals, clothing, foods |
· action words: come, go,
eat, drink, sleep, give, put, see, hear, wash, walk, run, play, pee |
· people: you, I, he,
she, it, we, they, Mama, Papa, Juan, Maria, and other family members |
· description words:
small, big, up, down, fat, thin, good, bad, hot, cold, day, night |
Start with a short list and gradually make it
longer. Use the words often, in daily activities (feeding, bathing, dressing),
and in play. Have the whole family learn the words on the list and how to make
the signs for them. Encourage everyone to use the words and signs together, not
only when they talk with the child, but when they talk with each other, and for
all the things they do in the home. This way the child will learn about language
by playing, watching, listening (as much as he can), and finally by copying -
the way most children learn language.
· As the child gets a little
older, help her become familiar with letters and written words. You can write
the first letter or name of things on different objects around the home. Or make
pictures of things with their names in big, clear letters. Or make pairs of
‘flash cards’ so the child can match pictures with words. This will
help the child understand hand signs that are based on letters. It will prepare
him for learning the alphabet in writing and signs, and for learning to read and
write.

Figure
SIGN LANGUAGE
In most villages and communities people use and understand many
gestures or signs made with their hands. Most of these signs are ‘common
sense’, or look something like the things they represent. Some
children’s games use hand signs. For example:
|
“Here’s the church.” |
Figure
|
“And here’s the steeple.” |

Figure
|
“Open the doors.” |

Figure
|
“And see all the people.” |

Figure
|
When a family has a deaf child, they begin to use the local
signs and also to invent new ones of their own. For example, at a village
rehabilitation center in Mexico, a family arrived on muleback with their 6 year
old deaf son. The boy got nervous and wanted to go home. So he pulled on his
father’s shirt sleeve and made these sounds and signs:
|
YOU |
and |
ME |
LET’S GO (home) |
RIDING THE MULE, |
PLEASE! |
|
Figure
|
|

Figure
|

Figure
|

Figure
|
Figure
|
The family had begun to figure out its own sign language,
without having been taught it. The boy himself had made up the sign for
‘RIDING the MULE’.
The sign language that families develop with their deaf children
is usually not very complete. Communicating is often still difficult. However,
people have joined together to create sign languages which are much more
complete. There are hundreds of different sign languages, but there are 3 main
types:
· National and
regional sign languages. In nearly all countries, deaf people have created
their own sign languages, in which they can learn to communicate as well and
nearly as fast as hearing people. Different hand signs represent different
things, actions, and ideas. The structure (grammar) of these languages is
different from the spoken language, and therefore is difficult for hearing
people to learn. These languages are preferred by people who were born deaf.
Examples are American Sign Language (ASL), which is used in the USA and Canada,
and Mexican Sign Language.
Figure
· Sign languages
based on spoken languages. These languages have the same organization and
grammar as the local spoken language. They are easier for hearing persons to
learn and for persons who became deaf after they learned to speak. Sometimes
they use the first letter (finger spelling) of a word as part of the sign. This
is harder for children to learn who cannot read, but can make learning to read
easier and more fun. Examples are English Sign Language and Spanish Sign
Language.
· Finger spelling. Each
word is spelled out with hand signs that represent the letters of the local
alphabet. This method of ‘writing in the air’ is slow but exact. It is
easier for persons to learn who can already read and write. For English, the
British use a 2-handed system and the Americans use a one-handed system. Try to
learn the system that is most used in your country.

Figure
|
Many deaf persons combine these 3 systems. With other deaf
persons they use mostly the first, with hearing persons or a
‘translator’ they use mostly the second, and finger spell difficult
words. When ‘talking’ to someone who does not know sign language, they
can write down what they need to say - or use a letterboard. (1) |
Figure
|
Learning to sign
If possible, contact the Association of the Deaf in your
country, and see if you can get a guidebook to sign language adapted to your
local area or spoken language. If this is not possible, you can use the local
signs and gestures, and invent more signs of your own.
On the next few pages we give ideas for making up signs, and
examples for common words. Most are signs used in American Sign Language. You
will want to change them to fit the gestures, customs, and language of your
area. Here are some ideas:
· Choose signs
that will not offend the local people. (Deaf people already have a difficult
time being accepted.) Here are some examples:
|
In the USA a pointing finger is used to indicate different
persons (me, you, her, them).
Figure
|
In some countries it is not polite to point a finger, so an open
hand is used.

Figure
|
In other places even pointing with an open hand is not polite,
and people point with their lips. HFR
Figure
|
|
In the signed alphabet used in the USA and Canada the letter
‘T’ is made like this.

Figure
However, in many countries, this is an offensive gesture |
Therefore, in this book we also use the ‘T’ sign from
Spanish and Danish.

Figure
|
Also avoid confusion. For example, the sign for
“WHERE” in the USA is a common gesture for “NO” in Mexico.

Figure
|
· Use local
signs. If people in your area already have a gesture or sign for something,
use that instead of a new or foreign one. For example:
|
The American sign for NO is this: |
Some countries use this sign for NO: |
In Jamaica NO and NOT are often said by a negative look and
shake or tilt of the head. |
The American sign for SLEEP is this: |
In Nepal this sign is used for SLEEP. It is understood almost
everywhere. |
|
Figure
|

Figure
|

NO, NOT ME
|

Figure
|

Figure
|
· Use hand shape,
position, movement, and direction to make different signs. The expression on
the face also adds to meaning. For example, here are signs for
MOTHER:
|
in Brazil |
in Australia |
in Spain |
in Thailand |
|
Figure
|

Figure
|

Figure
|

Figure
|
· Try
to make signs look like the things or actions they represent. To do
this you can use a combination of hand shapes and
movements.
|
TREE |
DISH |
POCKET |
BABY |
TURTLE |
|
Figure
|

Figure
|

Figure
|

Figure
|

Figure
|
· Figure out
patterns and series of similar signs for related things and actions, and for
opposites. For example:
|
STAND |
SIT DOWN |
JUMP |
PUSH |
PULL |
|

Figure
|
Figure
|

Figure
|
Figure
|

Figure
|
See other signs with fingers as legs.
· Learn new signs by
pointing to things.
|

Figure
Or if you can read and write, use finger spelling.

Figure
|
· Combine signs for things
and actions to communicate ideas or sentences. The arrangement of
words does not need to be the same as in the spoken language - and you can leave
out ‘extra’ words like “the” and “a.” Also, words
like “to” or “from” can often be left out or can be
indicated by the direction of a motion.
|
Set the table. |
Will you give me a banana, please? |
|
Figure
|

Figure
|
· Decide whether or not to
use letters of the alphabet to make some signs. In some sign languages the
first letter of a spoken (written) word is used as the sign for that word. At
first this will mean nothing to a child who cannot read, and will be harder. But
it can help prepare the child for learning to read and to finger spell. Again,
be systematic:
|
The sign for ‘W’ is |
WALL |
WATER |
WATERMELON |
|

Figure
|
Figure
|

Figure
|

1.

2.
(Tap with finger.) |
|
Be sure that letter-based signs agree with the word in
your language. In Spanish, “watermelon” is
“sand�a,” so the English sign makes no sense. The Spanish sign is:
|
SAND�A
Figure
|
(Tap with fist.)
|
· You can make up
signs for people’s names by using the first letter of their name, by
showing something that stands for that person, or both.
|
If Mar�a a looks like this, |
you might sign her name like this: |

Figure
|
|

Figure
|
1.
|

2.
|
|
|
Sign ‘M’ for Mar�a, |
and then the sign for ‘glasses’. |
(Move hands in direction it should be taken.) |
HOW TO ASK QUESTIONS
|
WHAT?

Figure
|
What time is it?

Figure
|
What did you do last night?

Figure
|
|
WHERE?

Figure
|
WHEN?

Figure
|
WHY?

Figure
|
WHO?

Figure
|
WHICH?

Figure
|
HOW MANY, HOW MUCH?

Figure
|
|
What is your name?

Figure
|
IS
Note: ‘Is’, ‘are’, ‘am’,
‘was’, and ‘were’ are often not used, as in “What is
your name?”
Figure
|
QUESTION MARK
Use before or after a statement to turn it into a question.
(motion of milking cow)
Figure
|
EXAMPLES OF SIGNS
The signs shown here are mostly used in the United States
(American Sign Language). A few are from Nepal, Jamaica, and Mexico, because
these seem easier to understand. We have chosen signs for things and actions
that should be useful for early learning and group games with children. We
include them mainly to give you ideas. Change and adapt them to better fit your
area.
· Arrows
( ) in the drawings show the direction of hand movement
to make the sign.
) in the drawings show the direction of hand movement
to make the sign.
· Wavy lines ( ) used with a sign mean a shake of the hand or
fingers.
) used with a sign mean a shake of the hand or
fingers.
· Dotted lines (------) show
how the sign looks when it begins.
·
The darker sign is how it looks when it ends.
|
Note: A few signs shown here are based on letters
of the alphabet (for example, ‘it’ uses the letter 7, and
‘we’ the letter ‘W’). Change these signs if you speak a
different language, or if you want to avoid signs based on letters. |
|
I, ME
Figure
|
YOU

Figure
|
THEY, THEM

Figure
|
MALE (MAN)
Figure
|
FEMALE (WOMAN)
Figure
|
Note: The male and female signs are used as the
base to make signs for boy, girl, father, mother, etc. |
|
FATHER
Figure
|
MOTHER

Figure
|
BROTHER

Figure
|
SISTER

Figure
|
BOY

Figure
|
GIRL

Figure
|
|
GRANDFATHER

Figure
|
GRANDMOTHER

Figure
|
FRIEND
Figure
|
BABY

Figure
|
MY

Figure
|
YOUR

Figure
|
|
HE, HIM

Figure
|
SHE, HER
Figure
|
HIS, HER, THEIR, YOUR
Figure
Direct sign toward person. |
IT

Figure
Or point to object. |
WE

Figure
|
OUR
Figure
|
|
GOOD

Figure
|
BAD

Figure
|
HAPPY
Figure
|
SAD

Figure
|
CLEAN/NICE

Figure
|
DIRTY/PIG

Figure
|
|
HOT

Figure
|
COLD

Figure
|
SMALL

Figure
|
LARGE

Figure
|
DOWN

Figure
|
UP

Figure
|
|
UGLY
Figure
|
PRETTY
Figure
|
FAT
Figure
|
THIN
Figure
|
WEAK

Figure
|
STRONG
Figure
|
|
INSIDE

Figure
|
OUTSIDE
Figure
|
UNDER

Figure
|
TIRED

Figure
|
SICK

Figure
|
ANGRY

Figure
|
|
HUNGRY

Figure
|
EAT

Figure
|
FOOD

Figure
|
THIRSTY

Figure
|
DRINK

Figure
|
WATER
Figure
|
|
MILK (motion of milking cow)

Figure
|
SOUP

Figure
|
BREAD

Figure
|
BOWL

Figure
|
SPOON

Figure
|
TOILET

Figure
|
|
HOUSE

Figure
|
VILLAGE, COMMUNITY, CITY, TOWN
Figure
|
SCHOOL

Figure
|
MONEY |
|
|
|
in America

Figure
|
MONEY in Nepal

Figure
|
MONEY in Mexico
Figure
|
|
BLIND

Figure
|
DEAF

Figure
|
HEARING AID

Figure
|
FORGET

Figure
|
REMEMBER
Figure
|
UNDERSTAND

Figure
|
|
RED

Figure
|
GREEN

Figure
|
BLUE

Figure
|
YELLOW

Figure
|
BLACK

Figure
|
WHITE

Figure
|
|
COME

Figure
|
GO
Figure
|
BEGIN
Figure
|
STOP

Figure
|
GIVE

Figure
|
HAVE (POSSESS)

Figure
|
|
WANT

Figure
|
DON’T WANT

Figure
|
SEE

Figure
|
LOOK
Figure
|
HEAR

Figure
|
LISTEN
Figure
|
|
TALK
Figure
|
MAKE
Figure
|
WORK
Figure
|
USE

Figure
|
PLAY

Figure
|
GAME

Figure
|
|
TAKE (CARRY)

Figure
|
BRING
Figure
|
PUT

Figure
|
HELP (ASSIST)

Figure
|
TEACH

Figure
|
LEARN
Figure
|
|
STAND

Figure
|
LIE DOWN

Figure
|
WALK
Figure
|
RUN
Figure
|
SLIP

Figure
|
FALL

Figure
|
|
SIT

Figure
|
SQUAT

Figure
|
LIKE

Figure
|
LOVE

Figure
|
DRAW

Figure
|
WRITE

Figure
|
|
CHICKEN

Figure
|
GOAT

Figure
|
HORSE

Figure
|
COW

Figure
|
BULL

Figure
|
DOG

Figure
|
|
DAY

Figure
|
MORNING

Figure
|
AFTERNOON
Figure
|
NIGHT

Figure
|
YES Nod hand like head.

Figure
|
NO

Figure
|
|
HAT

Figure
|
SHIRT
Figure
|
PANTS

Figure
|
SKIRT

Figure
|
SOCK
Figure
|
SHOE/SANDAL

Figure
|
|
FUTURE

Figure
|
PAST
Figure
|
It is going to rain.

Figure
|
It rained.
Figure
|
|
NOW

Figure
|
It is raining.
Figure
|
Throw the ball to her.

Figure
|
As you sign ‘THROW, move your hand in ‘her’
direction. (Separate signs are not needed.) |
NUMBERS (one of many systems)
|
1

Figure
|
2

Figure
|
3

Figure
|
4

Figure
|
|
5

Figure
|
6
Figure
|
7
Figure
|
8

Figure
|
|
9
Figure
|
10

Figure
|
11

Figure
|
12

Figure
|
|
13

Figure
|
14

Figure
|
15
Figure
|
16

Figure
|
|
17

Figure
|
18

Figure
|
19

Figure
|
20

Figure
|
|
21

Figure
|
22

Figure
|
50

Figure
|
100

Figure
|
|
Plurals (more than one)

Figure

Figure
|
ONE-HANDED SIGN ALPHABET (American)
|
A
Figure
|
B
Figure
|
C

Figure
|
|
D

Figure
|
E

Figure
|
F

Figure
|
|
G

Figure
|
H
Figure
|
I

Figure
|
|
J
Figure
|
K
Figure
|
L
Figure
|
|
M

Figure
|
N

Figure
|
O

Figure
|
|
P
Figure
|
Q

Figure
|
R

Figure
|
|
S

Figure
|
T American

Figure
|
T Danish
Figure
|
|
U

Figure
|
V
Figure
|
W

Figure
|
|
X

Figure
|
Y

Figure
|
Z

Figure
|
Helping the child learn to make sounds and speak
1. If the child hears at all, encourage her to notice and
listen to different sounds, as discussed.
2. Play games and do exercises to help her learn to use her
mouth, tongue, and lips. Have her press her lips together as if saying
“mmm,”  make a circle like ‘O’
make a circle like ‘O’
 , and stretch her mouth and smile as if saying
“eee”
, and stretch her mouth and smile as if saying
“eee”  .
.
See if she can touch her nose, her chin, and her cheeks with her
tongue. Have her blow soap bubbles, or blow out candles. Give her foods to chew
and suck.

Figure
3. Encourage the child to begin to make sounds.
‘Mmm’ is good to start with because it is easy to make. If
necessary, show the child how he can hold his lips together to make it. Sit
close to him so he can see (and hear?) and copy you. Other sounds that are
usually easy to learn are ‘ah’, ‘ay’, ‘ee’,
‘aw’, ‘o’, ‘p’, ‘b’, ‘t’, and
‘d’. (Keep more difficult sounds like V, ‘w’,
‘j’, ‘s’, ‘n’, ‘r’, and
‘z’ for later.)
Figure
4. If the child uses his mouth and lips, but not his voice, have
him feel the ‘buzz’ or vibration in your throat when you make
different sounds. To get the ‘feel’ of different words, you can place
his hands on your cheeks, lips, throat, and chest. Then have the child feel his
own throat, as he tries to copy you.

Figure
5. Also have the child feel and compare the movement of the air
in front of your mouth and his mouth with sounds like ‘ha’,
‘he’, ‘ho’, ‘m’, ‘p’, ‘b’, and
‘f’.
In the same way, have him feel the air move when he ‘blows
his nose’ with his mouth closed. Using this, try to teach sounds like
‘n’ and ‘l’.

Figure
6. Begin to teach the child words using the sounds he is
learning. First separate the word into different sounds. To say “Ma,”
first get the child to say “m” with the lips closed. Then
“ah” with the mouth open. Then say the word “mah” and have
him try to copy you.
7. As the child learns words, teach him what they mean, and have
him use them. For example, to teach the child ‘nose’, have him make
the sounds ‘n’, ‘o’, and ‘s’. Then have him put
them together. Ask the child to touch his nose as he says the word. Have him
copy you. Praise him, and make it a game.

Figure
8. Little by little, help the child learn more words and
practice using them through games and daily activities. Have her learn her own
name and the names of family and friends. Build up a word list as explained. But
do not try to go too fast. Take time to help her say a few words fairly clearly
before going on to the next.
Lip reading
Children with a lot of hearing loss often depend partly on lip
reading to understand what people are saying. But lip reading is not easy to
learn. Do not try to hurry the child or she (and you) can easily get
discouraged. Do not start teaching lip reading until the child is at least 3
years old.
|
Sit in front of the child in good light, and show him something,
for example, a ball. Say “ball,” moving your lips clearly and speaking
slowly. Let the child see your lips move, and watch your face. Repeat the same
word many times.
Then have the child try to imitate you, and feel his own lips as
he does. |

Figure
|
|

Figure
|
Next, sit with the child in front of a mirror, so that he can
see both of your faces. Say the word ‘ball’ and then have him copy
you, watching both of your lips and faces in the mirror. |
|
In this way teach him different words. Start with words where
the lips move a lot, and that are easy to tell apart. Pick words that you can
use often with him in games and daily activities. When you speak to him, make
sure he is watching your face and mouth. Use hand signs when he cannot
understand a word. But use the sign after speaking the
word, not at the same time. He cannot watch both at once. |

Be sure the child is watching
your lips.
|
You can play games with the child together with children who
hear, using ‘mime’ - that is, acting things out and saying words with
the mouth, without making sounds.
Unfortunately, some sounds and words look exactly the same on
the lips - the sounds ‘k’, ‘g’, and ‘h’, look the
same. ‘P’, ‘b’, and ‘m’ look almost the same.
‘T’, ‘d’, ‘s’, and ‘z’ look the same.
And so do ‘ch’ and ‘j’. To help the child tell
similar words apart, use hand signs or give him small ‘clues’, like
touching parts of the body, clothes, or food. For example:
|
If mama wears a dot on her forehead, |
and papa has a scar on one cheek, |
when anyone at home speaks of them they can also give the
‘magic sign’. |
|

Figure
|

Figure
|
Figure
|

Figure
|
PREVENTION of deafness
· Take steps to
prevent ear infection (teach the child not to blow her nose hard when she
has a cold). Treat ear infections at once when a child gets them. If the
child has frequent ear infections, see a health worker or ‘ear
doctor’. Do not put leaves or plugs of cotton in an infected ear. Let the
pus run out. See in Where There Is No Doctor.
· During pregnancy, do
not take medicines that might harm the baby. Tell the health worker or
doctor you are pregnant, and ask him to check if the medicine he prescribes is
recommended during pregnancy.
· Vaccinate girls and
women against German measles (rubella) before they get pregnant (but
never when pregnant). Or let young girls catch German measles by letting them
play or sleep with a child who has them. This will give them a
‘natural’ vaccination. Pregnant women should avoid getting near anyone
with German measles.
· Have regular medical
check-ups during pregnancy.
· Eat as well as possible
before and during pregnancy, use iodized salt, and include foods
rich in iron and other vitamins and minerals.
· Look for signs of cretinism
in the baby, and treat it early.
· Vaccinate the baby
against measles (and, if possible, mumps),
· Take precautions to prevent
brain damage and cerebral palsy.
· Never put, or let the
child put, pointed objects in the ears.
· Avoid being near very
loud noises. When a child cannot avoid them, teach him to cover his ears,
or use ear plugs.
Figure
Words to the family of a deaf child
Deaf children can grow up to be loving and helpful sons and
daughters, like other children. Try to let your child grow up. Give him the same
rights and responsibilities as other children his age.
If there is a chance for your child to go away to a school for
the deaf, if it seems right, try to let him go. Deaf children learn in different
ways than other children. The special school may provide more opportunities.
However, if your child is doing well at the village school, has a teacher who
understands and helps him, and has many friends, he might do better there. Help
him understand the choices and see what he thinks would be best. Be sure he
knows he has a loving family to come home to.
After they finish school, deaf children can do many different
kinds of work. Deaf people have become accountants, teachers, lawyers, farmers,
health workers, clerks, skilled craftsworkers, and doctors. It is worth the
effort to see that deaf children and adults get training and find work.
Be careful that after he has grown up, you do not treat him as a
child. He might seem younger than his age. But the best way to help him grow up
is to expect him to grow up.
When deaf children grow old enough to marry, they often choose
to marry someone else who is deaf, for they can understand each other better.
They can have children, and raise them well. Usually a deaf mother and father
have children with good hearing.
It is difficult to be deaf. You can help persons who are deaf by
letting them communicate in ways they find easy, and by trying to learn to
communicate with them
yourself.
Chapter 32: Mental Retardation: Down Syndrome, Cretinism, and Other Causes
Down Syndrome, Cretinism, and Other Causes
Mental retardation is a delay, or slowness, in a child’s
mental development. The child learns things more slowly than other children
his age. He may be late at beginning to move, smile, show interest in
things, use his hands, sit, walk, speak, and understand. Or he may develop some
of these skills more quickly, but be slower in others.
Mental retardation ranges from mild to severe. The child who is
mildly retarded takes longer to learn certain skills. But with
help he can grow up to care for himself and take an active, responsible part in
the community. The child who is severely retarded, as he grows
older, may stay at the mental age of a baby or young child. He will always need
to be cared for in some ways.
Mental retardation cannot be cured. However, all mentally
retarded children can be helped to progress more quickly. The earlier special
help or ‘stimulation’ begins, the more ability the child is likely to
gain.
IMPORTANT: In this chapter we look at some of the
causes of mental retardation and briefly describe 2 common forms (Down
syndrome and cretinism). However, mental retardation is only one of the
reasons for slow development in children. A child who is blind will be slow
in learning to reach and move about unless he has extra help and
encouragement. A child who is deaf will be delayed in learning to communicate
unless he is helped to learn to ‘talk’ in other ways than speech. A
child who has a severe physical disability is often slow in
developing use of both his body and mind. Because ‘developmental
delay’ is common with so many disabilities, we include discussion of it in
several separate chapters.

With help, some retarded children
can learn to read and write, and do many of the things that normal children do.
(Photo of a child with Down syndrome in Indonesia, by Carolyn Watson, Christian
Children’s Fund.)
|
Information on helping a child who is mentally retarded
or developmentally delayed is in Chapters 34 to 40. Chapters 34 and 35
discuss early child development and ways to help or ‘stimulate’
a child to learn early skills (use of the senses, movement, and communication).
Chapters 36 to 39 discuss learning for self-care (feeding, dressing,
toileting, and bathing). Chapter 40 discusses child behavior, and ways to
encourage behavior that helps learning.
Other ideas for helping retarded children are in the
CHILD-to-child activity on pages 442 to 445. The needs and problems of mentally
retarded children as they become sexually grown up are discussed in Chapter 52.
|
One important need that we do not include in detail in this book
is education for retarded children. Some possibilities are discussed in
Chapter 53, on education. But often special teaching methods and materials are
needed. An excellent book is Special Education for Mentally Handicapped
Pupils. For toys that help a child learn, see Chapter 49.
CAUSES OF MENTAL RETARDATION
There are many causes.
· Often the cause is
not known.
· Some children are born with a
very small brain, or the brain does not grow or work normally.
· Sometimes there is a
‘mistake’ in the ‘chromosomes’ or the tiny
chemical messages that determine what a child will be like
(inheritance). This is what happens in Down syndrome.
· Sometimes a mother did not
get enough of a certain food or mineral during pregnancy. (See
“Cretinism,”)
· Brain damage can happen
either before, during, or after birth. In addition to being retarded, these
children may also have cerebral palsy, blindness, deafness, or fits. Common
causes of retardation from brain damage are discussed in Chapter 9, and include:
· German measles during
early pregnancy
· meningitis (brain
infection) from bacteria, tuberculosis, or malaria, most
often during early childhood
· hydrocephalus, often
with spina bifida
· head injuries
· other causes include
brain tumor, poisoning from lead, pesticides, certain medicines and food,
and some forms of muscular dystrophy or atrophy
A child with microcephaly (small
brain) is mentally slow and often also develops certain physical problems. For
measurements of head size.
In many parts of the world, the most common causes of mental
retardation are brain damage and Down syndrome. But in some mountainous areas,
it is very often caused by lack of iodine in food and water.
Usually there is no treatment for mental retardation.
Therefore, we often do not need to know the exact cause. Instead, we need to
help the child develop the best he can. However, in some cases, certain
medicines, changes in diet, or prevention of further poisoning can make a big
difference. If a child has any signs of cretinism or seems to be gradually
losing mental ability, try to get expert medical advice.
Prevention of mental retardation is discussed with its
different causes. See especially cerebral palsy, Down syndrome, and cretinism.
|
MENTAL ILLNESS is different
Some people confuse ‘mental retardation’ with
‘mental illness’. But they are very different. A person who is
mentally ill may have normal or high intelligence, and may be highly educated.
But because of stressful experiences, or some illness affecting the brain, his
behavior becomes strange. When a retarded person behaves in an abnormal way, it
is usually because he has not learned the correct way to behave; he needs to be
taught. The mentally ill person needs special help - perhaps from a spiritual
healer or ‘psychiatrist’ (soul doctor). Persons with mental illness
are like persons with any other illness. Often they cannot control their strange
behavior. We should not blame or punish them, but give them love, protection,
and understanding. |
DOWN SYNDROME
In many areas, Down syndrome - or ‘mongolism’ - is the
most common form of mental slowness, or retardation. These children are slower
than others in learning to use their bodies and their minds. There are also
certain physical signs or problems. (This combination of various signs is called
a ‘syndrome’.) The baby does not develop normally in the womb because
of an error in the ‘chromosomes’ (material in each cell of the body
that determines what a baby will be and look like).
These are the typical signs of Down (but not
all the children have all these signs):
|
· At birth, baby seems floppy
and weak.
· Baby does not cry much.
· The baby is slower than other
babies her age to: turn over, grasp things, sit up, talk, walk.
· When suddenly lowered, the
baby does not react by spreading her arms, as a normal baby does. |

Figure
|

Figure
|
· eyes slant upward; sometimes
cross-eyed or poor sight
· ears low
· small mouth, hangs open; roof
of mouth is high and narrow; tongue hangs out |
|
· A fold of skin covers the
inner corner of the eyelid. (1)
· Eyelids may be swollen and
red.
· The iris of the eye has many
little white specks; like sand. These usually go away by 12 months of age. (2)
|

Figure
|

Figure
|
· short wide hands with short
fingers. The little finger may be curved, or have only one fold.
· one deep crease across the
palm (sometimes in normal children, too) (1) |
|
· short or small head, wide and
flat in the back
· sometimes dislocated hips (1)
|
Figure
|
· flat face
· small nose, flat between the
eyes |

Figure
|
· short neck
· rounded shoulders
· short arms and legs
· kneecap slips to one side (1)
· ‘pigeon-toed’; flat
feet (2)
· big toe far apart from other
toes (3) |
Other possible signs:
· Elbow, hip, and
ankle joints may be very loose and flexible.
· One out of 3 has heart problems.
· May develop leukemia (blood cancer).
· Check older children for hearing and seeing
problems.
· One out of 10 has deformed neck
bones which can slip and pinch the nerve cord in the spine. This may cause
sudden or slowly increasing paralysis - or sudden
death.
Care of children with Down and other forms of mental
retardation
Mental retardation in children with Down syndrome can be mild,
moderate, or severe. Some children never learn to speak. Others talk (and often
love to talk). Many can learn to read and write. Most of these boys and girls
are very friendly and affectionate, and behave well with people who treat them
well. Even those who are more severely retarded, with help and good teaching
usually learn to take care of their basic needs, and to help out with simple
work. They can live fairly normally with their families and communities.
In rural areas particularly, they can learn to do many important
jobs. Sometimes they do repetitive jobs as well or better than other people.
But their physical and mental development is slower than normal.
So parents and all those who take care of these children must be very patient
with them and from a very early age do all they can to help them develop their
mental and physical capabilities. To avoid or solve behavior problems, parents
need to be very consistent in how they treat their children and in what they
expect of them. The child needs a lot of praise and encouragement for things he
does well (see Chapter 40).
In one village, a young man with
Down works hauling water from the river, a job he is happy and proud to do.
Some children with Down syndrome can go to school, but they will
need extra help. It is important that teachers understand their problem and help
other children to treat the retarded child with respect. Unless the child is
given understanding and extra help at school, in rural areas it may sometimes be
better for the child with Down syndrome to be educated at home through helping
his family around the house and in the fields.
There are 3 main concerns in caring for a child with Down
syndrome:
1. Help the child to develop her or his mental and
physical abilities.
2. Protect the child from infectious diseases.
3.
Prevent or correct deformities.
Here we will discuss the last 2 concerns. The first we will
cover in other chapters.

A child with Down syndrome learns
to remove pegs from a pegboard. Later she will learn to place the pegs. Photo
from Teaching Your Down’s Syndrome Infant by Marci J. Hanson.
|
IMPORTANT: For a child who has Down
syndrome, or is mentally slow, be sure to read all the chapters on early
child development and learning basic skills, Chapters 33 to 41. |
Protection from infections
Children with Down syndrome get sick more often than other
children. They can easily catch colds, bronchitis, pneumonia, and other
infections. So it is very important to protect their health.

Figure
· Breast feed
the child as long as possible. Breast milk has ‘antibodies’ that
help the child to fight infections. (If he cannot nurse well, milk your breasts
and feed him the milk, using a spoon or any way that works.)
· Like any baby, at 5 months
start giving her other foods such as fruit, beans, eggs, and rice, but also
continue to breast feed her. (Like any baby, weigh her each month at the health
center to be sure she is growing well.)
· Vaccinations can
protect her from many childhood diseases. A child with Down syndrome who catches
measles or whooping cough can easily get pneumonia.
· Early medical attention
When she gets a sore throat, earache, or bad cough, take her to a health
worker as soon as possible.
PREVENTION of foot deformities and other problems
· Check all newborns
for possible dislocated hip, so that it can be corrected as
soon as possible.
· For the child
whose big toe sticks out,

Figure
do not use hard shoes that bend the big toe inward
like this.

Figure
It is better to wear tennis shoes, or other soft
shoes, or sandals.
Figure
When the big toe sticks out a lot, its position can
sometimes be corrected with surgery, so that shoes will fit without problems.
· If the child has severe
flat feet, a special insole may help.
· If any sign of paralysis or
lack of feeling develops in the hands, feet, or body, get advice from an
orthopedist or a neurosurgeon.
PREVENTION of Down syndrome
One out of every 800 children is born with Down and it occurs
more commonly with mothers under 20 and over 35 years of age. Women over 40 (or
even over 35) may want to consider not having more children. Also, if a couple
already has one Down child, the chance of having another is higher than normal
(about one in 50).
In some countries a test (amniocentesis) can be done at about 4
months of pregnancy to see if the child will have Down syndrome. If so, the
family can consider abortion (in societies where this is permitted).
CRETINISM (Hypo-Thyroidism)
Cretinism is a delay in both mental and physical growth that
comes when a child’s body does not produce enough ‘thyroid’.
Thyroid is a substance, or ‘hormone’, that controls a child’s
growth and body functions. Without it, everything goes slower.
Thyroid is produced by a gland in the front of the neck. To
produce thyroid, the gland needs iodine. Most people get enough iodine from
water and food. But in some areas, especially in the mountains, the soil, water,
and food have very little iodine. In an attempt to obtain more iodine, the
thyroid gland sometimes grows very large, forming a swelling called a goiter.

Figure
In areas where there is little iodine and a lot of people have
goiters, cretinism is common. In these same areas, often many children have
difficulty hearing or are somewhat retarded mentally. Although
they do not show all the typical signs of cretinism, the cause is probably the
same. Occasionally, in areas where goiter is not common, cretinism occurs for
other reasons than lack of iodine.
SIGNS Below we show some of the typical signs of
cretinism and compare them with Down syndrome, which cretinism resembles in some
ways. It is often difficult to tell if a newborn baby has cretinism. She is
often born large and then fails to grow normally. The baby may have feeding
difficulties, or breathing difficulties or make noises because of the large
tongue. She moves and cries little. By 3 to 6 months the mother often becomes
worried because the baby looks dull, takes so little interest in things, sleeps
so much, and is slow in all areas of development.
|
Signs of CRETINISM

Figure
· temperature below
normal
· thick, dry, cool skin |
· hair low on forehead
· puffy eyelids
·
flat base of nose between eyes
· puffy face,
hands, and feet
· fatty swelling here
(1)
· grows very slowly.
Increasingly
short for age.
· severe constipation (may go
days without shitting)
· often
deafness
· As child grows, knees may get
large and painful. |
Signs seen in both CRETINISM AND DOWN
· slow mental and physical
development
· widely separate eyes
· round face, dull look
· tongue sticks out of open mouth
· short neck and limbs; wide, short hands
· big belly and swayback
· often hernia of the navel (1)

Figure
|
Signs of DOWN SYNDROME (that are most useful in telling it from
cretinism)
· hair starts high on
forehead
· slant eyes with lid fold over
inner corners
Figure
|
Chapter 33: The Child with Several Severe Disabilities
Some children have a combination of severe disabilities.
We say they are ‘multiply disabled’. For example, a child may
be severely mentally retarded, and have little or no physical
control of his body. He may also be blind or deaf, have fits, or have difficulty
swallowing. Or he may have any combination of these disabilities - and perhaps
develop severe behavior problems.

A child with severe cerebral
palsy, who is also blind, has fits, and is mentally retarded.
Caring for multiply and severely disabled children is never
easy; they need an enormous amount of time, patience, and love. In most
communities, parents and close family members will be the main care providers.
But parents will need a lot of support from the community in order to care
adequately for the child. Unless parents have help, they are likely to find
that the continual demands of caring for their child are too much. Even the most
loving parents, after months and years of continuously caring for a severely
disabled child, can easily become frustrated and angry. This is especially true
when the child shows little progress or response, and grows up to be a physical
adult with the needs of a young child.
It is not uncommon for a parent who for years has poured love
and attention into a severely disabled, retarded child, to suddenly hit the
child or in other ways begin to neglect or mistreat him.
Before we blame the parent for this, we should try to put
ourselves in her position. She has given the child her total love and attention
for years. She has waited for a change, for a smile, for some return of warmth
and love. But the child remains like a newborn baby, becoming stiffer, more
fussy, and more difficult to lift and care for as he grows. Any human being can
only give so much without receiving something in return, some sign of
recognition or appreciation. In time, the parent is overcome by the unfairness
of the situation: the lack of appreciation, the constant demands, the lack of
help, the hurt. She reaches her limit and hurts the child in return. Rather than
blame her, we should try to understand her. Above all, we should look for
ways to help both the family and child - if possible, long before the mother or
other family members reach their limit.
COMMUNITY SUPPORT
There are several ways in which the community can give
assistance to the family of a severely disabled child. In some countries
(usually wealthier ones), the most severely retarded, multiply disabled children
may be taken care of in special care centers, or ‘institutions’.
Although in many cases it is better for the disabled child to stay at home
with his own family, there are times when institutional care is needed. This may
be because of difficulties in the home situation. Or it may be because the
multiply disabled child requires more time and skill than the family can handle.
Institutional care, however, is very costly, and is usually
possible only if government pays for it. Few governments of developing countries
are willing or able to do that. This means that in poor countries - and
especially in the rural areas - most support and assistance for these families
must come from the communities themselves.
In areas where a community rehabilitation program exists,
the program can play an important role. It will usually be neither desirable nor
possible for the program to take complete or continual care of the severely
disabled child. Yet, the program may be able to help in several ways:
· The community
rehabilitation workers can regularly visit the home of the severely disabled
child and give suggestions, assistance, and friendship.
· They can help make or provide
special seating or equipment that can help the family to manage the child
more easily.
· They can teach the family
ways to help stimulate the child’s development and can plan with the
family a step-by-step approach toward reaching realistic goals.
· Perhaps they can start
something like a ‘day care center’ where the rehabilitation
workers, different parents of disabled children, other concerned parents in the
community, or unemployed young persons take turns caring for the disabled
children for part of the day. This could be done on a volunteer basis. Or money
to pay for caretakers could be raised by the community, either through
donations, raffles, bake sales, musical events or other fund-raising
activities.
It is very important that the mother and family have rest
periods from caring for their severely disabled child.
Such rest periods can often make the difference between whether
or not they can handle difficulties and keep treating the child in a loving,
supportive way.
In some cases it may be better to provide ‘day care’
in the child’s own home. Again, the community may be able to provide either
volunteers or paid care-providers.
Whatever the case, often it is too much to expect the family
of a severely, multiply disabled child to care adequately for the child, unless
the community offers generous help and support.

Figure
CARING FOR THE SEVERELY DISABLED CHILD
In deciding how to care for and work with the child who has a
combination of severe disabilities, it is important to evaluate as best you can
both her disabilities and possibilities. Especially in the very
young child, this may not be easy. You must be ready to see new signs and change
your evaluation. This, in turn, may change your plan for working
with the child, so as to best help her to develop whatever skills and responses
are possible.
In evaluating and planning activities with the child, try to be
realistic. Do not expect too much, because this can lead to disappointment. But
at the same time, do not expect too little.
For example, a child with a serious physical disability who is
also deaf and/or blind may appear to be mentally retarded simply because her
ability to experience and respond to things around her is very limited. The
child may, in fact, have a lot more mental capacity (or
possibility) than she appears to have. It would be wrong not to look for ways of
reaching, developing, and appreciating her mind. However, this may take great
patience and creativeness by those caring for her.
SOME GOALS IN CARING FOR A SEVERELY AND MULTIPLY DISABLED
CHILD:
1. To help her to be physically comfortable, clean,
safe, and well-fed.
2. To help her with positioning and
exercise to prevent further deformity, and to make caring for her easier.
3. To help her learn whatever basic skills she can - in
developing head and hand control, and in some form of communication. Also, help
her learn to interact with others in a way that her needs are met and her
behavior is acceptable.
4. To make caring for the child easier and more enjoyable for
those who are responsible for her.
Much of the information and suggestions in Chapters 34 and 35 on
early stimulation and development may be helpful for the multiply disabled
child. Look for areas of development where the child seems to be most ready
or to have possibilities. Then work out a plan of activity, stimulation, and
rewards that will take the child forward one small step at a time. Some of
the suggestions included in Chapter 40, “Ways To Improve Learning and
Behavior,” may also help. However, you will need to apply them with much
patience and repetition.
To help meet the needs of the multiply disabled child, you will
also find useful information in the chapters on the different disabilities that
affect the child.
Special seating and positioning, discussed in Chapter 65, may
help the child to have more control of her body. This can make feeding, basic
communication, and other activities easier.

Special seating can help the
severely disabled child by supporting him in a position where he has better
control.

A child who is slower than most
in learning to use her mind and body needs extra help. Learning to twist and to
roll, and to lift up On her arms and turn, are important early developmental
steps. Here a rehab worker first helps ‘loosen up’ a child by slowly
swinging her hips from side to side.

Then she encourages the child to
lift up and turn to follow an object she wants.
CAUTION: Breast feeding is healthier than bottle
feeding. It is usually better to use a toy or rattle to draw the
child’s attention rather than a
bottle.
C. Helping the Child Whose Mind and/or Body are Slow to Develop
Chapter 34: Child Development and Developmental Delay
In Chapter 32 we discussed some of the primary causes of
‘mental retardation’. Mostly we looked at disabilities
that come from inside a child’s head - conditions where the brain
has been damaged, is too small, or for other reasons is not able to work as
quickly as other children’s brains.
|
CAUSES OF SLOW MENTAL DEVELOPMENT

Figure
|
In this chapter we see how a child’s early development also
depends on factors outside the child’s head - on the
opportunities a child has to use his senses, mind, and body to learn about the
things and people around him. We look at the stages or steps of normal child
development, and at ways we can help or ‘stimulate’ a child to learn
and do things more quickly. Our concern is not only to help children who are
‘mentally retarded’, but those whose development is slow, or
‘delayed’, for whatever reason.
Usually children whose minds are slow to develop are also
slow in learning to use their bodies. They begin later than other children
to lift their heads, roll, sit, use their hands, stand, walk, and do other
things. They are physically delayed because of their delayed mental
development.
In other children the opposite is true. Their minds are
basically complete and undamaged, but certain physical disabilities make it
harder and slower for them to develop the use of their minds.
For example, a child who is born deaf but whose brain is normal
will have difficulty understanding what people say, and in learning to speak. As
a result, she is often left out of exchange of ideas and information. Because
language is so important for the full development of the mind, in some ways she
may seem ‘mentally slow’ for her age. However, if the child is taught
to communicate her wishes and thoughts through ‘sign language’ at the
age when other children learn to speak, her thinking power (intelligence) will
often develop normally (see Chapter 31).
|
Figure
|
A CHILD’S MIND, LIKE A CHILD’S BODY, NEEDS
EXERCISE TO GROW STRONGER |

Figure
|
On the next page is a true story that shows how a severe
physical disability can lead to slow mental development, and how a family found
ways to help their child develop more fully.
|
ENRIQUE’S STORY |
|
Enrique had a difficult birth. He was born blue and limp. He did
not start breathing for about 3 minutes. As a result, he developed severe
cerebral palsy. His body became stiff and made strange movements that he could
not control. His head often twisted to one side and he had trouble swallowing.
To protect him, his mother kept
him on the floor in a corner.
Enrique’s mother loved him and cared for him as best she
could. But as the years went by, he did not gain any control of his body. His
mother kept him on the floor in a corner so that he would not hurt himself. He
spent most of his young life lying on his back, legs stiffly crossed like
scissors, head pressed back, looking up at the roof and the mud brick walls. By
age 3 he had learned to speak a few words, but with great difficulty. By age 6
he spoke only a little more. He cried a lot, had temper tantrums, and did not
control his bowels or bladder. In many
ways he remained like a baby. A visiting nurse called him ‘retarded’.
Still lying alone in the corner, Enrique grew increasingly withdrawn. At age
seven - if his mother understood him correctly - he asked her for a gun to kill
himself.
Soon after this, Enrique’s mother and his older sister took
him to a team of village rehabilitation workers in a
neighboring village. The workers realized that he would probably never have much
control of his hands and legs. But he desperately needed to communicate more
with other people and see what was going on around him, to be included in the
life of his family and village. But how could he do this lying on his back? His
mother had tried many times to sit him in a chair, but his body would stiffen
and he would fall off or cry.
Figure
|
The village workers helped Enrique’s family make a special
chair for him, with a cushion and hip strap to help him sit in a good position.
They taught his mother and sister how to help him sit in a way that would keep
his body from stiffening so much.

special cushion

Later, they added wheels to the
chair.
With his new chair, Enrique was able to sit and watch everything
that was going on around him. He was excited and began to take more interest in
things. He could also sit at the table and eat with the family (although his
mother still had to feed him). Everyone talked to him and soon he began to talk
more. Although his words were difficult to understand, he tried very hard. In
time, he spoke a little more clearly. He also began to tell people when he had
to use his toilet. He discovered he was no longer a baby, and did not want to be
treated as one.

Figure
Every day Enrique’s sister and brother went to school. One
day Enrique begged to go too, and they pushed him there in his chair. Soon he
went every day, and began to learn to read. Enrique had begun to develop more
control of his head. The village workers helped the teacher make a book holder
attached to Enrique’s chair, and a head band with a wire arm so that he
could turn the pages.

Figure
A happier and fuller life had begun for Enrique. |
Enrique’s story shows how development of the body, mind,
and senses all influence each other. Enrique was slow to develop mentally
because he did nothing but lie on his back in a corner. His mind did not have
the ‘stimulation’ (activity, exercise, and excitement) it needed to
grow strong. He had almost no control of his body movements. However, his eyes
and ears were good. When at last his body was placed so he could see and
experience more of the world around him, and relate more to other people, his
mind developed quickly. With a little help and imagination, he learned to do
many things that he and his family never dreamed he could.
We saw how Enrique’s physical disability slowed down his
mental development. Similarly, a child who is mentally slow is often delayed in
physical development. Development of body and mind are closely joined. After
all, the mind directs the body, yet depends on the body’s 5 senses (sight,
hearing, touch, taste, and smell) for its knowledge of people and things.
Therefore:
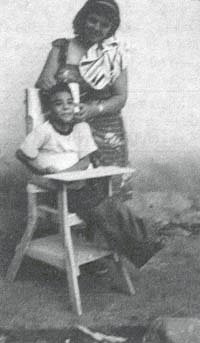
Enrique’s sister helps
position him in his new chair.

Figure
Each child, of course, has his or her own special
needs. Parents and rehabilitation workers can try to figure out and meet
these needs. (An example is Enrique’s need for special positioning
so that he can see and do things better.)
But all children have the same basic needs. They
need love, good food, and shelter. And they need the chance to explore their own
bodies and the world about them as fully as they can.
Early Stimulation
‘Stimulation’ means giving a child a
variety of opportunities to experience, explore, and play with things around
her. It involves body movement and the use of all the senses - especially
seeing, hearing, and touching.
Early stimulation is necessary for the healthy growth of every
child’s body and mind. For the non-disabled child, stimulation often comes
naturally and easily, through interaction with other people and things. But it
is often more difficult for the disabled child to experience and explore the
world around him. For his mind and body to develop as early and fully as
possible, he will need extra care and special activities that provide easy and
enjoyable ways to learn.
|
The younger the child is when a ‘stimulation
program’ begins, the less retarded or delayed he will be when he is
older. |
NORMAL CHILD DEVELOPMENT
In order to know how well a child is developing and in which
areas she may need special help, we can compare her development with that of
other children.
|
An understanding of normal child development can guide
us in planning activities that will help the disabled child progress. |
Every child develops in 3 main areas: physical (body),
mental (mind), and social (communication and relating to other
people). In each area, she develops skills step by step in a certain order.
During the first year of life, normally a baby gains more and more control of
her body.

A child’s abilities develop
in a particular order, one upon the other, like building blocks.
Body control develops progressively from the head down:
|
Development progresses from head to foot.

Figure
|
|
first, head and eye control
Figure
|
next, arm, and some hand control

Figure
|
then trunk (body) control, sitting, and balancing

Figure
|
and finally leg control

Figure
|
Before she can begin to walk, a baby needs to go through a
series of developmental stages, or ‘levels’. First, she has to be able
to hold up her head and see what is around her. This encourages her to use her
arms and hands so that she can then learn to lift herself to sit. While sitting,
she begins to reach, lean, and twist. All this helps her to develop balance and
to shift her weight from side to side - skills she will soon need for standing
and walking. Normally, the stimulation that a child needs to advance through
these stages comes from ordinary day-to-day interaction with people and things.
However, a child who has a disability may need special help to
keep progressing. Notice that in the above example, the child’s ability
to see makes her see things and want to reach for things and
explore. Seeing stimulates her to try to learn and do more. If a child
cannot see, this basic part of early stimulation is lacking. To prevent her from
falling behind, we must look for other ways to encourage her to learn and do
things. We can do this through touch and sound, adapting the type of
stimulation we use to the child’s particular stage of development. For
example, if a baby cannot see:
|
From the first we should hold her and speak to her a lot. Help
her to reach out to touch and feel different things.

Figure
|
Later, we can encourage her to lift and turn her head, and then
reach out, toward different sounds.

Figure
|
When she begins to sit, again we can help her to recognize
different sounds and reach toward them.

Figure
|
When she begins to walk we can help her find her way with guide
poles, and in other ways.

Figure
|
For more ways to help a child who cannot see well, see Chapter
30.
It is important for parents to realize that a child develops
control and use of her body in a certain order:
HEAD CONTROL ® TRUNK
CONTROL (SITTING AND BALANCE) ® STANDING
AND WALKING
This is true even for an older child. Often parents of an older
child who is delayed will try to help her learn more advanced skills (which
other children her age are learning) before she is ready. This often leads to
disappointment and frustration both for parents and child.
|
Trying to make your child walk before he is ready
is like telling him “JUMP NOW!”

Figure
when what you need to do is help him cross the gap-step by
step.

Figure
|
For example, Nina is a 3-year-old girl with cerebral palsy. She
still has trouble holding up her head or sitting without falling over.

Figure
However, her mother is sure she is ‘almost ready to
walk’. Several times each day she holds Nina in a standing position and
moves her forward, so that her feet take stiff, jerky steps on tiptoe. Her
mother does not know that this stepping is an ‘early reflex’ normally
only seen in young babies. It means that in some ways Nina’s development is
still at the level of a 1- to 3-month-old baby. She is not yet ready to walk.
Making her ‘take steps’ will only keep active the early reflex which
she needs to lose in order to learn to really walk.
‘stepping reflex’ in a
1-month-old baby
We must help Nina’s mother realize that Nina first needs
help with other important developmental steps before she will be ready to learn
to walk. To help her develop further, her mother will need to:
1. Figure out what developmental age or stage the
child is at.
2. Decide what are the next steps forward, so that the child can
build new skills on the ones she has now, in the same order in which a normal
child develops.
To do these things, Nina’s mother should first observe the
child carefully. In each area of development, she notes the different things
Nina can do, the things she cannot do yet, and the things she is
just beginning or trying to do, but still has trouble with. Next, her
mother compares what Nina can and cannot do with what other children Nina’s
age can do. She can then decide at what level her child is at in each area of
development, and what are the next steps to work toward.
THE CHART ON NORMAL CHILD DEVELOPMENT
The chart on the next 2 pages shows some of the steps or
‘milestones’ of normal child development. You can use it to figure out
where a child is in her development, and to plan the next steps that she needs
help with.
|
CAUTION: The development chart shows the average
ages when children begin to do things. But the ages at which normal children
develop different skills vary greatly. Just because a child has not
developed certain skills by the ages shown does not mean he is backward or has a
problem. Be sure to look at the whole child. |
EVALUATION OF A CHILD’S LEVEL OF
PHYSICAL DEVELOPMENT
Note: Although on these guides physical and mental skills
are separated, the two are often closely interrelated.
These charts show roughly the average age that a normal child
develops different skills. But there is great variation within what is normal.
Name: ____________________
Birth date:
_________________
Date: _____________________
Figure
EVALUATION OF A CHILD’S LEVEL OF MENTAL AND SOCIAL
DEVELOPMENT
Name: ____________________
Birth date:
_________________
Date: _____________________

Figure
Put a circle around the level of development that
the child is now at in each area.
Put a square around the skill to the right of the one you
circled, and focus training on that skill.
If the child has reached an age and has not mastered the
corresponding level of skill, special training may be needed.
How to use the Child Development Chart
The chart can be used to:
1. find and record a child’s developmental
level.
2. plan the next developmental steps or activities with which we
can help the child, and
3. and record in which areas the child is progressing, and how
much.
Let us suppose that a village health worker wants to help
Nina’s mother figure out what she needs to do next to help her 3-year-old
daughter develop early abilities. Together they look at the chart.
First they put a circle around each of the things that Nina can
do. Since she still has trouble holding her head up, they put a circle here. (1)
Nina needs help to roll from her belly to her back, so they put
a circle that goes part way around ‘rolls belly to back’. (2)

Figure
After they circle Nina’s level in each area of development,
they can see that in her general body movements and control, Nina is still at
the level of a 2- to 4-month-old baby. Her hand control is at about 6 months.
Her seeing and hearing seem about normal, and her mental development is at about
2 years.
Then they put a square around the next developmental step after
each circle. The squares show which developmental steps Nina now needs help
with. Because Nina’s poor head control is holding her back in other
areas, they decide to work mostly with this, and also to help her with rolling
and twisting her body. Perhaps they can begin to work with sitting and creeping,
but probably she will not progress much with these until she gets better head
control. The use of her hands is still somewhat behind for her age, but this may
partly be because of her poor head control. So they decide to have her sit for
short periods each day in a special seat. With her head supported in a good
position, they can give her games and things to do to help her develop better
use of her hands. But, they are careful not to keep her
head supported for long, because that will not help her to learn to support it
herself. Also, they are careful to provide only the least amount of support
needed to give her better control of other parts of her body. They will reduce
the support as her control improves.

Figure
Because Nina’s eyes, ears, mind, and speech seem to be
developing fairly well, these will probably be what she learns to use best as
she grows older. Therefore, her parents decide to do all they can to help her
improve these skills. They use pictures, songs, stories, play, and a lot of
stimulation to help her develop her mind. But they try to remember that she is
still only 3 years old. They must not push her too much. Sometimes it is better
to help her gain skill and confidence in only 1 or 2 areas at a time.
To use the Child Development Chart for recording a
child’s progress, every month or two you can add new circles to the
chart. Use a different colored ink each time, and mark the date in the same
color. Then add new squares to determine the developmental steps that are next
in line.
THE NEED FOR EARLY STIMULATION
The parents and family are the key to the development and early
learning of any child. Children who are developmentally slow need the same
stimulation (talking to them, music, games, adventure, and love) that any child
needs. But they need more. They need more help and repeated activities to use
their minds and their bodies.
|
When a child is delayed, he needs stimulation and activities
to help develop all areas of his body and mind. |
|
AREAS OF A CHILD’S DEVELOPMENT THAT CAN BE HELPED THROUGH
EARLY STIMULATION AND LEARNING ACTIVITIES |
|
1. Movement, body control, strength, and balance: these
will help the child move about, do things, play, and work. |

Figure
|
|
Figure
|
2. Use of the hands: increased hand control, and
coordination of the hands with what the child sees, allows the child to develop
many skills. |
|
3. The senses: especially seeing, hearing and feeling.
These will help the child recognize and respond to her world. |

Figure
|
|

Figure
|
4. Communication: listening, understanding what is said,
and learning to speak, or to communicate in whatever way is possible. |
|
5. Interaction with other people: smiling, playing,
behaving appropriately, and learning to ‘get along’ with others. |

Figure
|
|
Figure
|
6. Basic activities for daily living: eating, drinking,
dressing, and control of bowel and bladder (peeing and shitting). These
‘self-care’ skills help the child become more independent. |
|
7. Observing, thinking, and doing: to learn how to make
thoughtful, intelligent decisions. |

Figure
|
|
The goals of an early stimulation program are to help the
child become as able, self-sufficient, happy, and kind as possible. |
STEPS IN DESIGNING A PROGRAM OF SPECIAL LEARNING AND EARLY
STIMULATION
|
First: |
Observe the child closely to evaluate what he can and cannot do
in each developmental area. |
|
Second: |
Notice what things he is just beginning to do or still has
difficulty with. |
|
Third: |
Decide what new skill to teach or action to encourage that will
help the child build on the skills he already has. |
|
Fourth: |
Divide each new skill into small steps: activities the child can
learn in a day or two, and then go on to the next step. |

Figure
SUGGESTIONS FOR DOING LEARNING ACTIVITIES WITH ANY CHILD
(DELAYED OR NOT)
Be patient and observant. Children do not learn all the
time; sometimes they need to rest. When they are rested, they will begin to
progress again. Observe the child closely. Try to understand how she thinks,
what she knows, and how she uses her new skills. You will then learn how to help
her practice and improve those skills. When talking with the child, give her
time to answer your questions. Take turns speaking. Remember that practice and
repetition are important.
Be orderly and consistent. Plan special activities to
progress naturally from one skill to the next. Try to play with the child at
about the same time each day, and to put his toys, tools, clothes, and so on, in
the same place. Stay with one style of teaching, loving, and behavior
development (if it works!). Respond in a similar way each time to the
child’s actions and needs. This will help him to understand and to feel
more confident and secure.
Use variety. While repetition is important, so is
variety! Change the activities a little every day, so that the child and her
helpers do not get bored. Do things in different ways, and in various places
inside and outside of the house. Take the child to the market, fields, and the
river. Give her a lot of things to do.
Be expressive. Use your face and your tone of voice to
show your feelings and thoughts. Speak clearly and simply (but do not use
‘baby talk’). Praise and encourage the child often.
Have a good time! Look for ways to turn all activities
into games that both the child and you enjoy.
Be practical. Whenever possible choose skills and
activities that will help the child become more independent and be able to do
more, for himself and for others. To help prepare the child for greater
independence, do not overprotect him.
Be confident. All children will respond in some way to
care, attention, and love. With your help, a child who is delayed can become
more able and independent.
|
A special learning program, if well-planned and carefully
done, can help a delayed child progress much more than she would without
help. |
GENERAL GUIDELINES FOR HELPING A CHILD’S DEVELOPMENT
How a family member or rehabilitation worker relates to a child
when trying to teach her new skills can make a big difference in her whole
development. It can affect how fast or well she learns the new skill. More
importantly, it can influence the child’s confidence, behavior, and
readiness to learn.
There are a few simple methods that you can use to help a child
gain a better understanding of her own body, prepare her for learning
language, and help her relate to other persons in a friendly, cooperative
way.
These guidelines are especially helpful when doing early
learning activities with children who are developmentally delayed:
|
1. Praise the child a lot. Praise him, hug him lovingly,
or give him a little prize when he does something well (or when he makes a good
effort).

Figure

Figure
|
Explanation
Praising success works much better (and is much kinder) than
scolding or punishing failure. When the child tries to do something and fails,
it is best to ignore it or simply say something like: “Too bad, better luck
next time.”
CAUTION: Avoid giving sweets or food as prizes -
especially if the child is fat. |
|
2. Talk a lot to the child. Using clear, simple words,
say everything that you do with him.

Figure
|
Explanation
A child listens to and begins to learn language long before he
begins to speak. Although it may seem as though he does not understand or
respond, still talk to him a lot. If you think he does not hear, talk to him but
also use ‘sign language’. Make sure he looks at you as you speak.
|
|
3. When you are helping a child learn a new skill, guide her
movements with your hands.
For example, to teach a child to bring her hands to her mouth
(or to eat by herself) you can, |
Explanation
It usually works better to gently guide the child than to tell
her how to do something. If she tries to do something but has difficulty,
guiding her hands so that she is successful will make her a lot more eager to
learn the skill than if you say “NO-do it like this!” |
|
help her put her finger in a food she enjoys, |
and then to put her finger in her mouth. |
After the child has learned to do this, let her do it by
herself. |
|
|

Figure
|

Figure
|

Figure
|
|
|
4. Use a mirror to help the child
learn about his body and to use his hands.
Figure
|
Explanation
The mirror helps the child see and recognize parts of his body.
It is especially useful for children who have difficulty relating to different
parts of their body or knowing where they are. (This can happen in some forms of
mental retardation, cerebral palsy, spinal cord injury, and spina bifida.) |
|
5. Use imitation (copying). To teach a new action or
skill, do something first and encourage the child to copy you. Turn it into a
game.

Figure
|
Explanation
Many retarded children (especially those with Down syndrome)
love to copy or imitate the actions of others. This is a good way to teach many
things, from physical activities to sounds and words. |
|
6. Encourage the child to reach out or go for what he
wants.
Figure
When it gets too easy, put obstacles in the way - but do not
make them too difficult. |
Explanation
Even at early stages of development, it is a mistake to always
place in his hands what a child wants. Instead, use the child’s desire as a
chance to have him use his developing body skills and language skills to get
what he wants - by reaching, twisting, rising, creeping, or whatever he is
learning to do. |
|
7. Make learning fun. Always look for ways to turn
learning activities into play.
2 pieces of wood notched to fit
together crosswise
Figure
|
Explanation
Children learn best and cooperate more when they enjoy and are
excited by what they are doing. Keep doing an activity as long as it is fun
for the child. As soon as it stops being fun, stop the activity for a while, or
change it in some way, to put new adventure and excitement into it. |
|
8. Let the child do as much as she can
for herself. Help her only as much as is needed.
For example, if the child has trouble putting on clothes because
of spasticity, help by bending her shoulders and back forward, but
let her pull on her clothes herself.

Figure
|
Explanation
This is the “Golden Rule of Rehabilitation.” When a
child has trouble doing something or seems slow or clumsy at it, parents often
want to ‘help’ by doing it for her. However, for the child’s
development, it will help her more to let her do it herself - providing
encouragement but assisting only in ways that let her do more for herself. |
|
9. The child often learns best when no teacher is
present.
Figure
|
Explanation
Children often try hardest when they want something a lot, and
no one is there to help. Teaching is important, but so is giving the child a
chance to explore, test his own limits, and do things for and by himself. |
|
10. Get older brothers and sisters to demonstrate new
equipment.

Figure
|
Explanation
Some children may refuse to try, or will be afraid of new
playthings, aids, or special seating. If another child tries it first, and shows
he likes it, the child will often want to try it also. |
|
REMEMBER: Good teaching will make a difference.
How well you teach, play, and express affection is more important than
how much time you spend at it. |
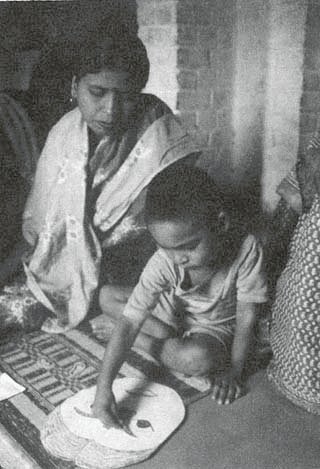
A mentally retarded child learns
the parts of a face by placing cut-out cardboard parts on a paper face.
(Samadhan, Delhi, India)
Puppets are used to teach
mentally retarded children in Samadhan (India). Each puppet wears clothes of one
color and has the name of that color. The children learn the puppets’ names
- and so begin to learn the
colors.
Chapter 35: Early Stimulation and Development Activities
On the next pages are activities to help young children’s
development. They are especially valuable for children who are mentally and
physically delayed. They are also useful for children who are mentally normal
but whose physical disabilities make both
physical and mental development slow
or difficult.
In this chapter we describe activities for early skills in the
order in which they usually develop. So we start with head control, then
progress to more advanced levels: reaching, grasping, sitting and balance,
scooting or crawling, standing and walking, and language. (Self-care activities
including eating, dressing, and toilet training are discussed in later
chapters.)
In any area of development, such as head control or use of the
hands, a child also advances through different stages of ability. For example,
in developing grip, first a child can grasp only with the whole hand, later with
thumb and finger.

Figure
To decide which activities to begin with, start by using the
charts on pages 292 and 293 to determine the developmental level of your
child. Then look through pages 302 to 316 and pick those activities that are
next in line for your child. After she learns these activities, go on to the
next.
A child advances in many areas of development at once.
Try to help her in several areas at the same time. In each area, pick
activities that help her do better what she already does, and then to take the
next step.
Often an activity that helps a child to develop in one area also
helps in others.
For example, we put the activity with this picture under
“head control.” But the activity also helps to develop use of
the senses (eyes, touch, sound), hand control, eye-hand coordination,
balance while sitting, and flexibility of the body (twisting to one side).
If done in a friendly way, with praise, it can develop confidence and
ability to relate to other people. And if father talks to the child as they
play, naming each object and action, it also prepares the child for learning
language.

Figure
When helping your child with these learning activities, remember
to introduce new skills in small steps that the child can easily learn.
Praise her each time she succeeds, or tries hard. Follow the suggestions
on pages 296 to 299 for helping the child develop these new skills.
|
CAUTION: Many activities in this chapter
are useful for children with cerebral palsy or other physical disabilities.
However, some must be changed or adapted. Read the chapters that apply to your
child’s disability. Above all: USE YOUR HEAD. OBSERVE
HOW YOUR CHILD RESPONDS. NOTICE HOW AN ACTIVITY HELPS-OR HINDERS-THE
CHILD’S WHOLE DEVELOPMENT. DO NOT SIMPLY FOLLOW THE INSTRUCTIONS. ADAPT
OR INVENT ACTIVITIES TO MEET YOUR CHILD’S NEEDS. |
1) Head Control and Use of Senses
1. Activities to help the child lift and control her head
(and use her eyes and ears)
One of the first skills a normal baby develops is the ability to
lift the head and control its movement. Head control is needed before a child
can learn to roll, sit, or crawl. Normally, a newborn child can lift or hold her
head up for a moment, and she develops fairly good head control in the first
months of life. Children with developmental delay are often slow to develop
head control. We need to help them to develop reasonable head control before
trying to help them to roll, sit, crawl, or walk.
|
To encourage the child to raise her head when lying face
down, attract her attention with brightly colored objects that make strange
or pretty sounds.
Figure
|
If she does not lift her head, to help her, put her like this.
Press firmly on the muscles on each side of the backbone and slowly bring
your hand from her neck toward her hips.

Figure
|
|
If the baby has trouble raising her head because of a weak back
or shoulders, try placing a blanket under her chest and shoulders. Get down in
front of her and talk to her. Or put a toy within reach to stimulate interest
and movement.

Some children can do more if they
lie on a ‘wedge’.
|
If the child has trouble lifting her head when lying face down,
lay her against your body so that she is almost upright. This way she needs less
strength to lift her head.
Figure
|
|
To help her develop head control when
lying face up, take her upper arms and pull her up gently until her head
hangs back a little, then lay her down again.
Figure
|
CAUTION: Do not pull the child up like this if her
head hangs back. As you begin to lift her, watch to see if her neck muscles
tighten. If not, do not pull her up. Also, do not pull the child up like this if
it causes her legs to straighten stiffly (see “Cerebral Palsy”).

NOT LIKE THIS
|
If a child with cerebral palsy stiffens as you pull his arms,
try pulling the shoulder blades forward as you lift him up.

Figure
|
|
If the child cannot lift his head as you pull him up, then do
not pull him up. Instead, sit the child up and gently tilt him back a little,
encouraging him to hold his head up. Repeat often, and as he gains strength and
control, gradually tilt him farther back - but do not let his head fall
backward. |

Figure
|
If the baby makes almost no effort to lift or hold her head when
you feed her, instead of putting the nipple or food into her mouth, barely touch
her lips with it, and make her come forward to get it. |

Figure
|
GOOD CARRYING POSITIONS
|
Carrying the child like this helps develop good head control,
when he is face down. |
Positions that keep the hips and knees bent and the knees
separate help relax and give better control to the child with cerebral palsy
whose body straightens stiffly and whose knees press together. |
Carrying baby like this frees his head and arms to move and look
around. |
|

Figure
|

Figure
|

Figure
|

Figure
|
|
As your child develops better head control, play with him,
supporting his body firmly, but with his head and arms free. Attract his
attention with interesting objects and sounds, so that he turns his head first
to one side and then to the other. |

Figure
|
2) Rolling and Twisting
2. Activities to encourage rolling and twisting
After a baby has fairly good head control, usually the next step
in development is to roll over. Rolling involves sideways twisting of the head
and body. Twisting, or rotation of the upper body on the lower body, must be
learned before a child can learn to crawl and later to walk.
Babies normally learn by themselves to roll over. But children
who are developmentally delayed will learn faster with special help and
encouragement. Help the child learn first to lift and turn her head to the side,
then her shoulders and body.
|
Attract the child’s attention by holding a rattle or toy in
front of her, |
Encourage her to reach sideways for the toy, |
|

Figure
|
|
then move the toy to one side, so the child turns her head and
shoulders to follow it. |
then move the toy upward, so that she twists onto her side and
back. |
|
If she does not roll over after various
tries, help her by lifting her leg.
Note: If the child has spasticity,
you may need to help position this arm before she can roll over. (1)
|
Also, help the child learn to roll from her back onto her side.
Again, have her reach for a toy held to one side. |
|

Figure
|

Figure
|
|
Note: If the child is very stiff, before doing
other exercises or activities, |

Figure
|
Or twist his body to one side and then the other. Have him help
by reaching for something he likes. Praise him when he does it. |
|
first help to relax him by swinging his legs back and forth,
|
or curl up the child in a ‘ball’ and slowly roll his
hips and legs from side |
|
|
|

Figure
|
Figure
|
|
|
Remember: THE FIRST RULE OF THERAPY:
HELP ONLY AS MUCH AS NEEDED, ENCOURAGING THE CHILD TO DO MORE AND MORE
FOR
HERSELF.
3) Gripping, Reaching, and Hand-eye Coordination
3. Activities to help develop gripping, reaching, and
hand-eye coordination
|
Most babies are born with a ‘grasping reflex’. If you
put your finger in their hand, the hand automatically grips it - so tightly you
can lift up the child. |

Figure
|
Usually this reflex goes away, and gradually the baby learns to
hold things and let go as she chooses.
Babies who are slow to develop sometimes have little or no
‘grasping reflex’ and are slow to learn to hold things. For such
children, these activities may help. |
|
If she keeps her hand closed, stroke the outer edge of the hand
from little finger to wrist. |
This often causes the baby to lift and open her hand, and to
grip your finger. |
|

Figure
|
|
CAUTION: In a child with
spasticity, stroking the back of the hand may cause her to
grip or open the hand stiffly without control. If so, do not do it, but look for
ways that give her more control. |

NO!
|
|
When the child opens her hands well, but has trouble holding on,
|
|
place an object in her hand, and bend her fingers around it. Be
sure the thumb is opposite the fingers.

Figure
|
Gradually let go of her hand and pull the object up against her
fingers or twist it from side to side.

Figure
|
When you think she has a firm grip, let go.
Repeat several times in each of the child’s hands.

Figure
|
|
After the child can hold an object placed in her hand, encourage
her to reach and grasp an object that just touches her fingertips. First touch
the top of her hand - then place it below her fingertips.

Figure
|
Encourage the baby to grasp by offering her rattles, bells,
colorful toys, or something to eat on a stick. |
|
Hang interesting toys, bells, and rattles where the child can
see and reach for them.

Figure
This way the child learns to move her hand forward to take hold
of a toy. |
If the child shows no awareness of her hand, hang little bells
from her wrist.

Figure
|
Also, for ways to help a child discover her hands by putting a
sweet food on her finger and helping her take it to her mouth.
|
At first a child can only grasp large objects with her whole
hand. As she grows she will be able to pick up and hold smaller things with
thumb and fingers. Help her do this by playing with objects of different sizes.

Figure
|
To help strengthen grip, play ‘tug-of-war’ with the
child - making it a fun game.

Figure
|
|
As the child gains more and more control, introduce toys and
games that help develop hand-eye coordination. For ideas. |

Figure
|
Make games of putting things in and out of boxes and jars. |
Playing with toys and imitating the work and play of others
helps the child gain more skillful use of his
hands.
4) Body Control, Sitting, and Balance
4. Activities for body control, balance, and sitting
After a child gains good head control; he normally starts
sitting through these stages.
|
sits when placed in a sitting position and held |
Figure
|
sits, keeping balance with arms |

Figure
|
balances with body while sitting, freeing hands for play |

Figure
|
sits up alone from a lying position |
Figure
|
In order to sit well a child needs to be able to hold her body
up, to use her hands to catch and support herself, and finally to balance with
her body so that she can turn and reach.
|
If the child simply falls over when you sit him up, help him
develop a protective reaction with his arms. Put him on a log, hold his hips,
and slowly roll him sideways. Encourage him to ‘catch’ himself with a
hand. |

Figure
|
Or do the same thing with the child on your belly.

Figure
|
|
After the child learns to ‘catch’ herself when lying,
sit her up, hold her above the hips, and gently push her from side to side.
|

Figure
|
and forward and backward so that she learns to catch and support
herself with her arms. |

Figure
|
|
CAUTION: The child must be able to raise and turn her
head before she can raise her body. |
|
To help your child gain balance sitting, first sit her on your
knees facing you. |
Later, you can sit her facing out so that she can see what is
going on around her. |
|
Figure
Hold her loosely so her body can adapt to leaning (1)
|

Figure
Slowly lift one knee to lean her gently to one side. Then the
other, so that she learns to bend her body to stay seated. (2) |
|
You can do the same thing with the child sitting on a log.
As he gets better balance, move your hands down to his hips and
then thighs, so that he depends less on your support. |

Figure
|
Give him something to hold so that he learns to use his body and
not his arms to keep his balance. |
|
With an older child who has difficulty with balance, you can do
the same thing on a ‘tilt board’. |
Or you can do the same on a large ball. |
|

Figure
|
Figure
|

Figure
|
|
At first let her catch herself with her arms. |
Later, see how long she can do it holding her hands together.
Make it a game. |
Tilt it to one side and the other and also forward
and back. |
|
Note: You can also do these exercises by sitting
the child on a table and gently pushing him backward, sideways, and forward. But
it is better to tip what he is sitting on. |
Figure
|
Pushing him causes him to ‘catch himself from
falling with his arms.
Tilting him causes him to use his body to keep his
balance, which is a more advanced skill. |
|
Help the child learn to keep her balance while using her hands
and twisting her body, |
|
sitting on the ground,

Figure
|
and sitting on a log or seat.

Figure
|
|
When the child can sit by herself, help her learn to sit up,
|
|
from lying on her back,

Figure
As the child starts to rise, push on the higher hip. |
and from lying on her belly.

Figure
First help her lift her shoulders. |
Press down and back on hip.
Figure
Help her roll to one side, rise onto one elbow, and sit. |
Help her to sit up herself. Do not pull her up. Praise her
each time she does well, or tries hard. Help her less and less until she can
sit up alone.
|
Some children will need seating aids to sit well. To help
improve balance, the aid should be as low as possible and still let the child
sit straight. Often, firmly supporting the hips is enough. Here are 2 examples:

Figure
|
For the child who needs higher back support, simple ‘corner
seats’ can be made of cardboard, wood, or poles in the ground.
Figure
|
For more ideas on special seating and
positioning, see Chapters 64 and 65. For sitting
aids.
5) Creeping and Crawling
5. Activities for creeping and crawling
|
To move about, many babies first begin to creep*,

Figure
|
and then to crawl*,

Figure
|
or to scoot on their butt.

Figure
|
*North American therapists use these terms in the
reverse way (creep for crawl and crawl for creep).
|
Note: Some babies never crawl but go
directly from sitting to standing and walking. Whether or not they crawl often
depends on cultural patterns and whether the family encourages it. |
If the child can lift her head well when lying on her stomach,
encourage her to begin creeping in these ways:
Put a toy or food the child likes just out of reach.
At first it may help to support his feet.

Figure
|
CAUTION: If the child has cerebral palsy,
supporting the feet may cause legs to straighten stiffly. If this happens do not
support her feet. |
If the child cannot bring her leg forward
to creep, help her by lifting the hip.
Figure
If the child has difficulty beginning to creep or crawl:
|
Let her ‘ride’ your knee. Play ‘horsey’.
Slowly move your knee up and down and sideways so that she shifts her weight
from side to side. |
Or put the child over a bucket or log. To help him bear weight
with his elbows straight, firmly push down on his shoulders and release. Repeat
several times. |
|

Figure
|
Encourage her to lift one hand off the ground and shift her
weight to the other. Then help her to move forward. |
Figure
|
|
If the baby has trouble beginning to crawl, hold him up with a
towel like this. As he gains strength, gradually support him less. |
Older brothers and sisters can help.
Encourage the child to first reach-and later crawl - for
something he wants. |
|
Figure
|
Move him from side to side so he shifts weight from one
arm and leg to the other. |
Figure
|
|

Figure
|
You can hang the child from a roof beam or branch, or a doorway,
like this. |
A child with spastic legs can hang with her legs supported to
allow moving about using her arms.
Or make a simple ‘creeper’. |
|
Figure
|

Figure
|
|
When the child has learned to crawl fairly well, have him play
crawling games. |
She can crawl up and down a small hill or pile of straw. This
will help improve her strength and balance. |
|

Figure
|

Figure
|
|
To help an older child with balance problems to prepare for
walking, encourage him to crawl sideways and backward. |
Also, have him hold one leg or arm off the ground and shift his
weight back and forth. |
|

Figure
|

At first, you may need to hold up
one limb while you slowly rock him from side to side.
|
|
Later, have him practice holding one arm and the opposite leg
off the ground at the same time. |
A ‘rocker board’ is fun and helps balance. |
|

Figure
|

Figure
|
|
After a child gets her balance on hands
and knees, you can help her begin to stand - and walk - on her knees. She can
walk sideways along the rope. |
Figure
|
There are many ways the child can practice standing on her knees
and shifting her weight-ways that are fun and include her in family activities.
|

Figure
|
|
CAUTION: Do not do this in a child with
spasticity whose knees bend a lot when she stands. |
6) Standing, Walking, and Balance
6. Activities for standing, walking, and balance
Normally a child progresses through these stages:
|
bears part of weight automatically when held like this (standing
reflex) |
automatically ‘steps’ if tilting forward (stepping
reflex) |
sinks down when stood up, |
stands holding on |
pulls up to standing |
steps sideways holding on |
steps between objects |
walks with 2 hands, 1 hand, and finally, no support |
|

Figure
|
Figure
|
Figure
|

Figure
|

Figure
|
|
0-3 months |
0-3 months |
3-6 months |
7-9 months |
|
You can prepare a child for walking by encouraging each of the
above stages as the child develops.
|
CAUTION: If the child cannot balance when sitting, do
not work on walking yet. Help her develop sitting balance first. |
Hold the baby so that she uses the early stepping reflex
to strengthen her legs. You can even bounce the baby gently.

Figure
|
CAUTION: In children with spasticity,
this activity may increase muscle stiffness. DO NOT DO IT. |
When the child begins to stand, support her hips with your
hands. Spread her feet apart to form a wide base. First do this from in front,
later from behind.

Move her gently from side to
side, so that she learns to shift her weight from one leg to the other.
As she gains better balance, you can
provide a light support at the shoulders.

Figure
Or have the child hold a hose or rope. Because it is flexible,
he needs to balance more.

Later, he can hold onto the rope
with one hand only.
To encourage a child to pull up to standing, put a toy he likes
on the edge of a table. (1)

Figure
To encourage him to take steps, put something he likes at the
other end of the table. (2)
When a child can almost walk alone but is afraid of falling, tie
a cloth around his chest
Hold the cloth, but let it hang
completely loose. Be ready to catch him if he falls
|
CAUTION: Do not let the child hang by the
cloth. Have him bear his own weight. The cloth is only to catch him if he falls.
|
Other activities for improving balance:
|
Hold the child loosely under the arms and gently tip him
from side to side and forward and backward. Allow him to return to a straight
position. Turn it into a game. |

Figure
|
At first support the child while you do this. When his balance
improves, do it without supporting him - but be ready to catch him if he falls.
|
|
Practice walking sideways and backward.
Note: Walking backward helps children who tend to walk
tiptoe to bring their heels down.

Figure
|
|
It is better to hold a child: |
|
LIKE THIS |
NOT LIKE THIS |
|
His balance is centered in his
body.
|

His balance is off center.
|
|
Support your child only as much as he needs, until he can
walk by himself. |
For the older child with poor balance, a homemade
balance board will turn developing better balance into a game. Move
slowly at first - especially with a child with cerebral palsy. |
|

Figure
Draw a square on the ground and help him to take steps forward,
sideways, and backward. Follow the 4 sides of the square, always facing the same
direction. Make it fun by having him collect a different colored tag or piece of
puzzle at each corner - or however you can. |
A balance board with a wide
rocker is better because it rocks more smoothly.
Blocks to prevent rolling sideways. (1)
Some children will need a pole to
hold onto.
|
|
Simple homemade parallel bars can help a child with weak
legs or a balance problem get started walking.

Figure
|
Homemade pushcarts or walkers can provide both
support and independence for the child who is learning to walk or who has
balance problems.

Figure
|

A simple wooden walker with
plywood wheels helps this developmentally delayed child begin to walk. (For
designs of walkers)
|
7) Communication and Speech
7. Activities for communication and speech
A normal child’s ability to communicate develops through
these stages:
|
expresses needs through body movements, looks on the face, and
crying |
makes ‘happy sounds’ - coos and gurgles |
babbles - listens to sounds and tries to imitate |
says a few words |
begins to put words (and ideas) together |
|

Figure
|

Figure
|
Figure
|

Figure
|

Figure
|
|
0-1 month |
1-2 months |
4-8 months |
8-12 months |
12 months-3 years |
|
Learning that prepares a baby for speech begins early, long
before she says her first word. Speech develops out of body movement, use of the
mouth and tongue in eating, and use of the senses - through interaction with
people and things. |
One of the early stages in a baby’s development of speech
is noticing and responding to different sounds. A delayed child may need extra
help and stimulation:
|
Make noises with bells, rattles, clickers, and drums, first
directly in front of the baby, then to one side, so that she turns her head.
|

Figure
|
If she does not turn her head, bring the toy back so she can see
it, and move it away again.
‘Or, gently turn her head so that she sees what makes the
sound. Help her less and less - until she turns her head alone. (1) |
|
Repeat the babble of the child: have conversations with
him in his language. But when he begins to say words, repeat and pronounce them
clearly and correctly - do not use ‘baby talk’. |

Figure
|
To get the child used to language, explain everything you do
with him. Use clear, simple words - the same ones each time. Name toys,
objects, body parts. Repeat often.
Figure
|
|
Understanding language depends not only on hearing, but also on
watching lips and looks. So speak to the child on her level. |
A child understands words before he can speak them. Play
question games to help him listen and learn; he can answer your questions
by pointing, nodding, or shaking his head.

Repeat words. Make small
requests. Reward successes.
|
|

Figure
|
Figure
|
|
|
Rhythm is important to language development. Sing songs, play
music, and have the child imitate body movements: clap your hands, touch
your toes, or beat a drum. |
Imitate the sounds that baby makes and have him copy the same
sounds when you make them. Then say words similar to those sounds.
Also, imitate use of the mouth: open wide, close tight, stick
out tongue, blow air, push lips in and out. |
|

Figure
|
CAUTION: Encourage use of gestures, but not
so much that the child does not feel the need to try to use words. |

Figure
|
SPECIAL PROBLEMS IN SPEECH DEVELOPMENT
A mouth that hangs open or drools is a passive (inactive) mouth.
It makes development of language more difficult. Often children with Down
syndrome or the floppy type of cerebral palsy have this problem.
Here are some suggestions to help correct the problem of
drooling and to help strengthen the mouth, lips, and tongue for eating and
speaking ability.
|
CAUTION: If the child’s mouth hangs open and she
drools, do not keep telling her to close it! ‘ This will not help and will
only frustrate the child.

Figure
|
|
Stroke or tap the upper lip, or gently press the lower lip
several times. |

Figure
|
Or, gently stretch the lip muscles. This may help the child to
close his mouth. |

Figure
|
|
To strengthen the tongue and lips, put honey or a sweet, sticky
food on the upper and lower lips. Have the child lick it off. |

Figure
|
Figure
|
You can also put sticky food on the inside of the front teeth
and roof of the mouth. Licking this food helps prepare the tongue for saying the
letters T, D, N, G, H, J, and L. |
|
Also have the child lick sticky food from a spoon and lick or
suck ‘suckers’ and other foods or candies. (1)

Figure
|

Figure
|
Put food into the side of the mouth and behind the teeth so that
the child exercises the tongue. Also, have the child try to take food off a
spoon with his lips. (1)
Begin to give the child solid foods, and foods she needs to
chew, as early as she can take them (after 4 months). This helps develop the jaw
and mouth. |
|
CAUTIONS: |
1. Do not do licking exercises in a child with cerebral palsy
whose tongue pushes forward without control. This can make the ‘tongue
thrusting’ worse.
2. After giving the child sweet or sticky food, take extra care
to clean teeth well. |
Play games in which you have the child:
|
suck and blow bubbles through a straw |

Figure
|
blow soap bubbles |

Figure
|
|
blow air |

Figure
|
blow whistles |
Figure
|
|
CAUTION: For children with cerebral palsy, these blowing
exercises may increase the uncontrolled tightening of muscles or twisting of the
mouth. If so, DO NOT USE THEM. |
Encourage mouthing and chewing on clean toys (but not thumb
sucking).
|
Help the child discover how to make different sounds by flapping
her lips up and down with your finger, |

Figure
|
or by squeezing them together as she makes sounds. |

Figure
|
For a child with cerebral palsy, you can help him control his
mouth for eating or speaking by stabilizing his body in a firm position. Choose
the position in which he is most relaxed (least spastic). This usually means
bending the head, shoulders, and hips forward. For this reason it is sometimes
said:
|

“WE CAN CONTROL THE LIPS
THROUGH THE HIPS.”
|
You can help the child make different sounds by pushing on and
jiggling his chest.
Imitate the sounds he makes and encourage him to make them by
himself. |
|
If the child has trouble with controlling his jaw when he tries
to speak, try using ‘jaw control’ with your fingers, like this.
Have him repeat sounds that require jaw movement.

Figure
|
When the child has difficulty pronouncing words, do not
correct her. Instead, repeat the words correctly and clearly, showing that
you understand.

Figure
|
REMEMBER - The child needs a lot of
stimulation of all her senses to develop language. Play with her, speak to her,
and sing to her often. Ask her questions and give her time to answer. Do not
try to ‘make her learn’, but give her many learning opportunities.
Ask questions that need words for answers, not just ‘yes’ or
‘no’.
Is your child deaf? If your child is slow to speak, check
his hearing. Even if he hears some noises, he may not hear well enough to
understand speech.
Also, some children who hear well may never be able to speak.
For example, certain children with cerebral palsy cannot control their mouth,
tongue, or voice muscles. For these children, as for young deaf children, we
must look for other ways to
communicate.
8) Early Play Activities and Toys
8. Early play activities and toys
Play is the way children learn best. So try to turn every
activity you do with a child into some kind of play or game.
It is not what you do, but how you do it that makes
something play. As long as it is fun and the child wants to do it, it is play.
But if it stops being fun, or the child does it only because ‘he has
to’, it stops being play. Small children (and big children who learn
slowly) only stay interested in the same thing for a short time. The child soon
gets bored and stops learning. Therefore, for activities to be play and stay
play,
1. continue with the same activity for a short time
only, and
2. look for ways to keep changing the activity a little so that
it is always new and interesting.
|
Figure
|
Both boys in these pictures are doing the same learning
activity. For one, it is play. For the other, it is not. Can you say why? |

Figure
|
Not all play has to be organized or planned; often the child
learns most when it is not. Play needs some aspect of adventure, surprise,
and freedom. It is important that a child learn to play with other
children. But it is also important that she be given the chance and
encouraged to play alone. She needs to learn to enjoy and live with other
people - and with herself.
We do not talk much about play separately, because mostly it is
not a separate activity. It is the best way to do almost any activity. For this
reason, in this whole chapter - and book - we often give ideas for turning
exercise, therapy, and learning into play.
Play activities, like other activities, should be picked so
that they ‘fit’ a child’s level of development and help him move
one step farther. They should be HARD ENOUGH TO BE INTERESTING, but EASY ENOUGH
TO BE DONE WELL. For example:
|
If the child is at the level of a very young baby, play games
that help him use his eyes and hold up his head. |
Figure
|
If the child is at the level where she sits, but finds it hard
to keep her balance or open her knees, look for play that helps her with these.
|

Figure
|
If in preparation for standing and walking the child needs
practice shifting weight from one knee to the other, you might try imitation
games. Here are 2 ideas:

Figure

Figure
TOYS AND PLAYTHINGS TO STIMULATE A CHILD’S SENSES
Play is more important than toys. Almost anything - pots,
flowers, sandals, fruit, keys, an old horseshoe - can be used as a toy, if it is
used in play.
Toys - or ‘playthings’ - offer stimulation for a
child, both when she plays by herself and when she plays with others. Many
simple things in the home can be used as toys, or can be turned into them.
|
Hanging toys for baby to admire, touch, and handle can be made
of many things

Figure
|

Figure
|
Caring for babies provides a learning experience that combines
work and play for the child who is gentle. |

Figure
|
|
CAUTION: Take care that toys are clean and safe for
the child. |
Here are a few examples of interesting toys. Use your
imagination and the resources of your family to make toys.
|
Toys for touching |
Toys for seeing |
|
soft clothes or blanket
baby animals
corn on the
cob
finger paints
inner tubes for swimming, bathing
nuts and
bolts
toes and fingers
seed pods
mushy food
cloth
doll
gourds
sand |
clay
string
chain
pulley
gears
rocks
beads
fruits
mud

Figure
|

Figure
flowers
dough |
mirrors
colors
colored paper or tinfoil
daily family
activity
puppets
old magazines with pictures
crystal glass pieces
(rainbow maker)
flashlight (touch) |
Figure
finger
puppets |
|
Toys for balance |
|
For children who have trouble controlling their movements, and
often drop or lose their toys, it may help to tie the toys with string, as shown
here.

Figure

Figure
|
swings
hammocks
seesaws
rocking horses |

Figure
|
|
|
Toys to taste or smell |
Toys for hearing |
|
foods
flowers
fruits
animals
spices
perfumes
|
Figure
|

Figure
rattles
guitar
flutes
drum
bells
bracelets on
baby’s wrist and ankles that tinkle when baby moves |
marimba or xylophone
wind chimes
whistles
pet
birds
animal sounds
seashells or other echo
toys
talking
laughing
singing |

Figure
a pan as
a drum |
|
tin can telephone

Figure
string or wire, stretched tight |
TOYS TO DEVELOP A CHILD’S MIND AND HAND-EYE
COORDINATION
Learning to fit things into things
|
Start simple - dropping objects into a jar, then taking them out
again. |
|
As the child develops, make things more complex. |
|

Figure
|
rings of wood, woven string, baked clay, old bones, or buckles
(1)
base of wood or several layers of cardboard (2)
wood or corncob (3) |
Figure
|
Note: Rings can be of different sizes,
colors or shapes so that the child can also learn to match these. |
|
To help develop controlled movement of the hands and arms, the
child can move beads or blocks along a rod or wire. |

Figure
|
Using animals or funny figures makes the exercise more fun.
Other children will be more likely to join in the game. |

Figure
|
Matching games
|
The child can match objects of similar shape, size, and color.

Figure
|
Small pegs glued onto cut-out pieces help develop fine hand
control.

Figure
|
|
|
|
Start with simpler games with square or round figures.

Figure
|
Then progress to more complicated games with different shaped
figures.

Figure
|
Puzzles
Jigsaw and block puzzles and building blocks also help a child
learn how shapes and colors fit together. Suggestions for making different
puzzles are on.

Figure
Many more ideas for simple toys are included in Chapter 49,
“A Children’s Workshop For Making
Toys,”.
D. Helping Children Develop and Become More Self-reliant
Chapter 36: Feeding
Feeding is one of the first abilities that a child develops to
meet her needs. Even a newborn baby has reflexes that cause her to:
|
turn her head to seek the breast when her cheek is touched.
|
suck and swallow, |
and cry when hungry. |
By a few months of age, the child learns to take solid
food in her mouth and eat it. |
|

Figure
|

Figure
|

Figure
|

Figure
|
Normally a child’s feeding skills gradually increase
without any special training. She learns first to use her lips and tongue to
suck and swallow liquids. Later she learns to bite and chew solid foods, and to
take food to her mouth with her hands. The early head-turning and sucking
reflexes gradually go away as she learns to control her feeding movements.
Some children, however, do not develop feeding skills easily or
naturally. This may be because the child’s whole development is slow
(retarded). Or, because the child has a particular physical
difficulty (such as a hole in the roof of her mouth - see “Cleft
Palate,”).
Children with cerebral palsy often have feeding
difficulties, which are sometimes severe. Difficulty with sucking (or being
unable to suck) may be the first sign in a child who later develops other signs
of cerebral palsy. Or the child may have trouble swallowing, and easily choke on
food. Uncontrolled movements of the body, pushing out the tongue, or floppy,
inactive lips may also be a problem.
One reason that some disabled children are slow to develop
self-feeding skills is that their families continue to do everything for them.
Because of a child’s other difficulties, her family may continue to treat
her as a baby. They may give her only liquids, and put everything into her
mouth, rather than encouraging her to do more for herself.
|
REMEMBER: Helping the child develop feeding
skills as early as possible is of special importance because good nutrition
is essential for health and life. The food needs of a disabled child are the
same as for any child.
Good use of the lips and tongue when feeding is also important
for future speech.

Figure
|
POOR NUTRITION IN DISABLED CHILDREN
Poor nutrition or ‘malnutrition’ usually results from
not getting enough to eat and is one of the most common causes of health
problems. With its signs of weakness, thinness, failure to grow, and reduced
ability to fight off illness, poor nutrition might be considered a
‘disability’ itself. It affects at least 1 out of every
6 of the world’s children, mainly those who live in poor countries.
In this book, we do not discuss the problems of malnutrition in
detail, because they are covered in most primary care handbooks (see Where
There Is No Doctor, Chapter 11). However, a special warning: is
called for.

A VICIOUS CYCLE
|
WARNING: Disabled children are often in greater danger
of malnutrition than are other children. |
Sometimes this is because the child has difficulty sucking,
swallowing, or holding food. Sometimes it is because the family gives more food
to the children who are stronger and more able to help with daily work.
Sometimes, however, it is because parents, although they treat their disabled
child with extra love and care, keep bottle feeding him (with milk, rice water,
or sugared drinks) until he is 3 or 4 years old or older. They keep treating -
and feeding - their child like a baby, even though he is growing bigger and
needs the same variety and quantity of foods that other children need.

This 4-year-old with spina bifida
has no difficulty eating any foods. Yet his family still treats him like a baby
- complete with a baby bottle filled with a sweet drink - just because he is
‘disabled’.
To give a child only - or mainly - milk and sweet drinks after 6
months of age may keep the child fat. But he will slowly become malnourished.
Milk and sweet drinks lack iron, so that the child may become more and more
pale, or anemic (weak blood).

Normal: Lips, tongue and
fingernails have a reddish, healthy color.

Anemic: Lips, tongue and
fingernails, pale. Lack of energy. Tires quickly.
|
CAUTION: It is important that disabled children
get enough to eat. It is also important that they do not eat too much and get
fat. Extra weight makes it more difficult for a weak child to move about. If
the child is getting fat, give him less fatty foods and sweets.

DO NOT LET A DISABLED CHILD GET
FAT!
|
|
REMEMBER: A disabled child needs the same foods that
other children of the same age need. |
THE BEST FOOD FOR YOUR YOUNG CHILD
THE FIRST 4 TO 6 MONTHS

Give breast milk and nothing
else.
BREAST IS BEST because breast milk contains the ideal
combination of foods that the child needs, is clean, and is always
the right temperature. Also, breast milk contains ‘antibodies’
from the mother that protect the baby against infections.

Figure
Therefore, breast milk is especially important for children more
likely to get infections, such as a child with Down syndrome or a
child who often chokes on her food and might get pneumonia.
|
Breast milk is healthier for babies than other milks or
‘formula’. |
If the baby cannot suck, a mother can milk her breasts:
Figure

And then give the baby her milk
with a cup and spoon.
|
WARNING:
Avoid baby bottles whenever possible. They often spread
infections.

NO

Cup and spoon feeding is
safer.
|
FROM 4 TO 6 MONTHS AND AFTER

Figure
Continue breast feeding and also begin to give the baby other
foods - juices and fruits rich in vitamins, mash of green leafy vegetables,
beans (boiled, skinned, and mashed), peanuts (skinned and mashed), egg yolks,
and other local staples such as rice, corn, plantains, or cassava.

Figure
|
Small stomachs need food often. Feed children under 1
year old at least 5 times a day - and give them snacks between
meals. |
If the child has trouble eating solid foods, do not keep giving
only milk or formula or ‘rice water’. Even mother’s milk alone is
not enough after 6 months.

Figure
Mash or grind up other foods to form a drink or mush.

Figure
|
By 8 months to 1 year of age the child should be eating the same
food as the rest of the family-even if it has to be mashed or turned into
liquids. |

Figure
Successful feeding involves the whole child
The more difficult it is for a child to control his body
movements, the more difficult it will be for him to feed himself. A child with
Down syndrome may have trouble feeding because of weak mouth and lips and poor
head control. But the feeding problems of a child with cerebral palsy are more
complex. They may include: lack of mouth, head, and body control; poor sitting
balance; difficulty bending hips enough to reach forward; poor hand-eye
coordination; and difficulty holding things and taking them to his mouth. We
must consider all these things when trying to help the child feed more
effectively.
It is not enough simply to put food or pour drink into the mouth
of a child who has difficulty sucking, eating, and drinking. First, we must look
for ways to help the child learn to suck, swallow, eat, and drink more normally
and effectively. Here are some suggestions.
POSITIONS FOR FEEDING
Be sure the child is in a good position before you
begin feeding her. The position will make feeding either easier and safer, or
more difficult and unsafe.
|
Do not feed the baby while she is lying on her back because this
increases the chance of choking.
In a child with cerebral palsy, it often causes backward
stiffening, and makes sucking and swallowing more difficult.

WRONG
|
Feed the baby in a half sitting position with her head bent
slightly forward.
In a child with cerebral palsy, to keep the head from pushing
back, hold the shoulders forward, keep the hips bent, and push firmly on the
chest.

RIGHT
|
Do not let the head tilt backward. It makes swallowing harder
and may cause choking.
In a child with cerebral palsy, avoid pushing the head forward
like this. It will cause the baby to push her head back more forcefully.
WRONG
|
Positions for feeding with a bottle, spoon, or finger are like
those for breast feeding.
|
If the baby does not suck and swallow well, the mother may think
she should put a bigger hole in the nipple, tilt the baby’s head back, and
pour the milk into the baby’s mouth.
WRONG
But this may choke him, and it does not help him learn to suck
well. |
Position the baby so that the head is slightly forward, and the
bottle comes from in front, not above.
Pushing gently on the chest helps stop backward stiffening so
the baby can swallow better.
RIGHT
If possible, have baby hold bottle. |
To avoid the backward stiffening, bend the shoulders and back
forward, keeping the hips and knees bent. Be sure the head bends a little
forward.
Place food below and in front of child, not above or behind him.

RIGHT
foot life to keep the baby’s knees higher (1) |
A simple ‘baby seat’ can help the baby hold a
good position while eating. Here is one idea using an old plastic bucket.
Figure
|
REMEMBER: When feeding a child with
cerebral palsy,
giving food from above often causes the head to press
back and body to stiffen. It makes swallowing difficult.
WRONG
Giving food from in front helps stop stiffness and makes
eating and swallowing easier.

RIGHT
|
For other seating ideas.
HELPING CONTROL MOUTH FUNCTION
The child may also need help in improving the
sucking-swallowing reflex, and her ability to eat from a hand or spoon
and to drink from a cup. Sometimes these can be improved by using
what is called ‘jaw control’.
Jaw control. Before giving the breast, bottle, spoon or
cup, place your hand over the child’s jaw, like this:
|
if you sit beside the child |
if the child is facing you |
|
Figure
|
|
At first the child may push against your hand, but after she
gets used to it, it should help her control the movement of her mouth and
tongue. Be sure not to push her head back, but keep it bent forward slightly.
While you feed the child, apply gentle, firm steady
pressure - not off and on.
Good positioning together with jaw control will help with
several problems common in cerebral palsy, such as pushing the tongue forward,
choking, and drooling (dribbling). As mouth control improves, gradually
lessen and finally stop jaw control.
For more suggestions for controlling drooling and improving use
of the lips and tongue, see the section on developing speech.
|
For the child who has difficulty breast feeding (or bottle
feeding), as you apply jaw control try bringing her cheeks forward with your
fingers. |
Figure
At the same time, push gently against the child’s chest
with your wrist. (This may help the child who tends to stiffen backward.) (1)
|

Figure
If you bottle-feed the baby, an ‘old-fashioned’ large
round nipple usually works best.
If the child still has trouble sucking, try making the hole in
the nipple bigger and thickening the milk with corn meal, gelatin, or mashed
food. |
|
CAUTION: Jaw control helps in many children
with developmental delay and cerebral palsy - but not all. After trying it for 2
or 3 weeks, if the child still resists it or shows increased problems, stop
using jaw control. |
Spoon feeding
The child who has no sucking-swallowing reflex needs to be fed
with a spoon.
|
Always give the spoon from in front, (1)

Figure
RIGHT |
not from the side, (1)

Figure
WRONG |
and not from above. (1)

Figure
WRONG |
|

Figure
|
YES |
|
The best spoon is rounded and shallow. |
|
|

Figure
|
NO |
|
Not deep because this makes it hard for the lips to get out the
food. |
|
|
Figure
|
NO |
|
And not long and pointed as this could cause choking. |
|
‘Tongue thrusting’
A baby sucks by moving her tongue forward and backward. For this
reason, when the child begins to eat from a spoon, her tongue will at first push
part of the food out of her mouth. She has to learn to use her tongue
differently - pushing the food between the gums to chew, and to the back of her
mouth to swallow. Children with developmental delay or cerebral palsy may have
trouble learning to do this, and continue to push or ‘thrust’ the
tongue forward for some time. Do not mistake this for meaning she does not
like the food.

Figure
Jaw control, although helpful, may not be enough to prevent this
tongue thrusting. It also helps to apply firm pressure with the back of the
spoon on the tongue as you feed the child. This helps keep the tongue from
pushing forward and lets the child use his lips and tongue better.
|
CAUTION: Better to use a strong (metal)
spoon and NOT a thin plastic one that might break when you push down the
tongue. |
Do NOT scrape the food onto the upper lip or teeth as you take
the spoon out. Instead, let the child try to get the food off the spoon onto her
tongue. To make it easier for her, start by putting only a little food on the
end of the spoon. As you take the spoon out, make sure the mouth is closed so
that the tongue can move the food inside the mouth and cannot push it out.
WRONG
If eating with fingers is the custom, or if spoon feeding is too
difficult, use your fingers.
Here a mother holds her child in a good position on her lap,
using her legs and body to give support.
With one hand she gives jaw control while she feeds him with the
fingers of the other hand. Place a little food on the side or middle of the
tongue - not on the front of it.
Figure
For spoon or finger feeding, it is best to start off with soft,
mushy foods rather than liquids. Milk (even breast milk) or egg yolk can be
mixed with rice paste, boiled corn, or mashed beans. You can also give small
pieces of fruit, mashed greens and vegetables, and yogurt or soft cheese.
Hardest for the child to eat are combinations of liquids and
solids - such as vegetable soup.
|
CAUTION: Remember to wash your hands before feeding
child with your fingers. |
Chewing
To help the child learn to chew, put a bit of firm food in
the side of her mouth between her teeth. Use very small pieces of bread
crust, tortilla, or chapati. Help her close her mouth using jaw control.
Biting off can be encouraged by pulling slightly on a long thin
piece of food. (1)
Or rub the piece of/food against the teeth before putting it
between them.

Figure
|
CAUTION: Do NOT open and close the
child’s jaw or help her chew. After she bites the food, her jaw must
stay closed or almost closed to chew. To help her do this, apply steady firm
pressure with jaw control. This should lead the child to make chewing motions.
Let the jaw move some on its own. But do NOT make chewing motions for the
child! This will only encourage abnormal movements. |
If the child has difficulty chewing and chokes on pieces of
food, try this:
|
Cut a piece of clean, soft cotton cord, or braid thin strips of
cotton cloth. Soak or cook the cord in a tasty good food and hold the end while
she bites and chews on it, squeezing out the nutritious juices. Help with jaw
control. |

Figure
|
|
This method is completely safe. Because you hold on to the cord,
the child cannot bite off pieces and choke on them. It is best to practice this
at the beginning of a meal while the child is still hungry. |

Figure
|
|
A finger-shaped piece of tough cooked or dried meat or very
tough chicken (old rooster) can be used instead of the cord. Be sure it is too
tough for the child to chew pieces off of it, but juicy or tasty enough to give
her pleasure. (1) |
|
CAUTION: If a piece of food slips back into
the child’s throat and gets stuck, bend the child far forward, and keep
calm. The food should drop out. Do NOT pat the child on the back as this could
cause the child to breathe in the food.
If the food does not fall out and the child cannot breathe,
suddenly and forcefully squeeze the child’s lower chest (see Where
There Is No Doctor). |
Drinking
Successful drinking, like eating, involves the whole child. Body
position is important. For example, in a child with cerebral palsy, to drink
from a regular cup or glass, his head must be tilted back. But this can cause
uncontrolled backward stiffening and possible choking.

Figure
However, if he uses a plastic cup with a piece cut out,
he can drink without bending his head back.
|
The cup should have a projecting rim. |
Figure
|
Cut out a-space to fit around the child’s nose. |

Figure
|
This way the child can drink in a better, more controlled
position. |
Figure
|
|
You can make a special cup from a plastic bottle. |
Figure
|
|
Cut it like this. |
Figure
|
|
Gently heat the rim and gradually bend it out with a round
smooth rod or stick. |
Figure
|
|
Figure
|
At first you may need to apply jaw control to help the child
close her lips on the rim of the cup. Tilt the cup so that the liquid touches
the upper lip and let the child do the rest. Do NOT take
away the cup after each swallow as this may trigger pushing the head back or
tongue out. It helps to start with thick liquids - like cooked cereals, maize
mush, or yogurt.
Self-feeding
To be able to feed herself, a child needs more than control of
her mouth, lips, and tongue. She also needs to be able to sit With her head
up, to pick things up, and to take them to her mouth.
To prepare for self-feeding, encourage the child to play, taking
his hands and toys to his mouth. Also, encourage him, when sitting, to balance
while he uses both hands.

Figure
A child with poor balance or uncontrolled movements will at
first need special seating adapted to her needs.
|
A HIGH CHAIR

Figure
Try one or more straps, to see what works best. (1) |
A CARDBOARD BOX SEAT

Figure
|
Figure
|
Some children with cerebral palsy may only need a foot strap to
stay in a good position (to keep the body from straightening stiffly as shown
above). |
|
CAUTION: Seats or straps that limit
movement should be used only until the child learns to control her position
without being tied or held. Special seating should help the child to do more
and to move more freely. It should not become a prison! For more seating
ideas, see Chapter 65. |
When a child is slow in using her hands to grasp things, or to
take things to her mouth, you can help her discover how to use her hands and
feed herself, like this:
|
Put the child’s finger in a food she especially likes.

Figure
|
Then lift her finger to her mouth.

Figure
|
Help her to do more and more, step by step, until she does it
alone.
Figure
|
Little by little help her less and less. Lift her hand to her
mouth and touch her lips with the food. See if she will then put it into her
mouth. When she has learned this, lift her hand near her mouth and see if she
will do the rest. Next just put her finger in the food and encourage her to lift
it to her mouth. Each time she does more for herself, praise her warmly.
This method is part of a ‘behavioral approach’ to
teaching new skills. The same approach can be used for teaching the child many
skills related to eating, such as using a spoon or drinking from a glass. To
learn more about this approach, see Chapter 40, “Ways to Improve Learning
and Behavior.”
|
IMPORTANT: Try to make mealtime a happy
time.
Remember that it takes time for any child to learn new skills,
and that a child learns best when he plays. When any child first learns to eat
for himself, he makes a mess. Be patient, help the child to become more skillful
at eating, praise him when he does well, but at the same time let him enjoy
himself and his food. Remember, even normal children often do not learn to eat
cleanly and politely until they are 5 or 6 years old - or even older.
A cover or ‘bib’ like
this, of plastic or waterproof cloth, is a big help. The pocket at the bottom
catches spilled food. (1)
|
While it is important not to push or hurry children too much in
developing feeding skills, the opposite is also true. Often parents wait too
long and do not expect enough from their disabled child. On the next page is a
‘trick’ that a rehabilitation worker uses to help parents awaken to
the ability of their retarded child to learn new skills.
|
THE 6 MINUTE BISCUIT TRICK FOR DEVELOPMENTALLY DELAYED
CHILDREN
by Christine Miles, Mental Health Centre, Peshawar, Pakistan
The ‘trick’ gets parents to open their eyes to what
their child actually can do and learn to do. I see many parents with
developmentally delayed children between 15 and 30 months. They have realized
that the child is not functioning at a level appropriate for his age. But often
they cannot describe what the child actually can do, and do not seem to realize
that children gain new skills by learning. Parents complain that “He
doesn’t speak. He can’t do this, he can’t do that,” as
though there is something wrong with the machinery or someone has failed to push
the correct button.
I ask them whether the child can eat a biscuit (cookie).
“No, he only has milk and mush. He can’t feed himself.” I get a
biscuit and put it into the child’s hand. I guide the hand up to the mouth.
Sometimes the child will bite on the biscuit; sometimes it needs to be tapped
gently against his teeth and wetted with his lips and tongue until a piece
breaks off and is eaten. I move the child’s hand away from the mouth, then
repeat the process. Usually by the time half the biscuit has gone, the child has
learned how to do it, and finishes the biscuit happily without help. The parents
usually say “Oooh!”

Figure
In 6 minutes the parents have watched their child learn
an important skill, by our using a simple directed action and a strong
reward (tasty food). Whether their child is temporarily delayed in development
or will be permanently retarded, the parents gain some vital information about
the child’s ability to learn. Whether or not they remember anything else
that I say to them, they go away with a whole new experience to think about.
Almost always they have consulted several doctors before coming here, without
gaining any useful advice.

Figure
Of course, it is not guaranteed to work. But it does work
surprisingly often. The 6 minute biscuit trick is a powerful stimulant to
parents to actually observe their child and to help the child learn. |
SELF-FEEDING SUGGESTIONS FOR THE CHILD WITH CEREBRAL
PALSY
|
COMMON PROBLEMS |
SUGGESTIONS |
|

Figure
|

Figure
|
Help him learn to hold the spoon firmly. |
|
|
WRONG
|
BETTER
|
|
|

Straighten his hand by turning it
out gently from the base of the thumb. (1)
|
|
Sometimes you can help her with head control by gently pressing
one hand flat against her chest. |
Raising the table may make it easier for some children. |
Where the custom is to eat sitting on the floor, a child may be
helped by making a low table out of a box. |
|

A child who has difficulty
controlling her hand for eating may gain better control by resting her elbow on
the table. (1)
|
Figure
|
Sometimes you can help the child
avoid twisting to one side by bending the less-used arm across the belly, and
turning the palm up. (1)
|
|
When head and body are difficult to control, it may help to sit
on a bench or log in a ‘riding’ position |
A child who has trouble controlling a cup with one hand can
often do better if the cup has two handles. |
|

If he sits with a rounded back,
it may help to support the lower back.
|

Ask a local potter to make
one.
|
Figure
|
Homemade equipment to help eating
A plate with steep sides makes eating easier for the child who
uses only one arm. When that arm is very weak, it helps if the dish is low on
one side and high on the other, to push food against.
|
This boy, whose arms and hands are paralyzed, lifts his spoon by
raising and lowering his shoulder. His forearm is on the table edge, so that
when he lowers his elbow, his hand lifts. (1) |

Figure
|
A non-slip mat under the plate can be made from strips of tire
tube woven over a stiff wire frame. (2) |
|
The spoon slips into a leather or rubber (tire tube) hand band.
|

Velcro (or buckle)
|

Figure

Figure
|
The special plate can be made from a small plastic bucket. (1)
To preventslipping, you can glue (with a waterproof glue) strips
of tire tube on the bottom. (1) |
|
A non-spill cup holder can be made using 2 plastic
bottles.

Figure
|

Figure
Fill space between containers with fine sand, plaster, or
cement. (1) |

Figure
Seal with wax or waterproof glue. |
Or, glue a plate or tin to the bottom of the cup.

Figure
|
|
Spoon handles for easy gripping |
Tortilla or chapati holder |
|
tortilla |
|

rubber tube
rubber ball
strip of tire tube (wrapped)
Figure

Figure
|

From UPKARAN Manual.
|

From UPKARAN Manual.
|
Swing-a-sling eating aid
|
This eating aid lets a child with very little strength in her
arm feed herself. However, it must pivot smoothly but firmly at 3 points. It
will take a skillful and imaginative craftsperson to make it. |

Figure
|
The spoon holder can also be adapted to hold a pen, brush, and
other things. (1) |
Arm rocker - for a child whose arm is too weak to lift
|
Carve it out of wood - or glue together layers of
‘Styrofoam’ (stiff foam plastic) or cardboard. |

Figure
|
|
Or make it from the bottom of an old plastic (or metal) bucket.
|

Figure
|
Figure
Heat the plastic along the lines with a hot strip of metal.
|
Straps may or may not be needed.

Figure
And bend it like this. |

A boy with muscular dystrophy,
whose arm is too weak to lift it to his mouth, eats with the aid of an arm
rocker. This arm rocker, cut out of Styrofoam, took about 5 minutes to make.
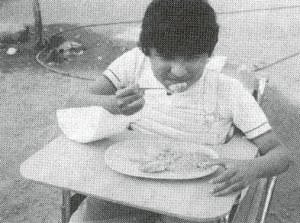
A boy with muscular dystrophy,
whose arm is too weak to lift it to his mouth, eats with the aid of an arm
rocker. This arm rocker, cut out of Styrofoam, took about 5 minutes to make.
Feeding aids for a child with no hand use
|
Put a ruubber band or clip on the spoon handle to keep spoon
from slipping in clothespin. (1) |
|
Figure
|

Figure
|
|
Pick up food holding spoon in mouth.

Figure
|
Slip spoon into clothespin.
Figure
|
With the lips, turn clothespin so that spoon enters mouth.

Figure
|
|
Note: If other children laugh at the child’s
awkwardness, let him practice alone until he gains some skill. |
Children with no use of their arms can feed themselves by
lowering their mouths to their food. It helps if the plate can be lifted nearer
to the face. A pot like this helps to stabilize the plate. If the plate has a
rounded bottom, the child can tip it bit by bit as it is emptied.
A rack allows the child to drink
from a cup that he can tip with his mouth.

Or simply use a straw.
|
Use your imagination to think of many other ways to
help the disabled child eat and do other things for herself. |
Chapter 37: Dressing
Children with disabilities, like other
children, should be encouraged from an early age to help with their own
dressing. It is important, however, not to push a child to learn skills that are
still too difficult for her level of development.
AVERAGE AGE WHEN NON-DISABLED CHILDREN DEVELOP DRESSING
SKILLS
|
under 1 year old Baby does not help at all. |
1 year old Cooperates when being dressed. |
2 years old Removes loose clothing. |
3 years old Puts on loose clothing. |
4 years old Buttons large buttons |
5 years old Dresses alone except for difficult steps. |
6 years old Ties shoe or adjusts sandals. |
|

Figure
|

Figure
|

Figure
|

Figure
|
Figure
|

Figure
|

Figure
|
Children may learn dressing skills at different ages depending
on local customs and on how much importance parents give to learning these
skills. Observe what other children in your village can do at different ages.
Children may begin to take off their clothes before they are 2 years old, yet
may not learn to put on all their clothes correctly until they are 5 or 6 years
old. Often a normal 6-year-old may put a shirt on backward, or the left sandal
on the right foot.
Children who are slow in their development or who have
difficulty with movements may be slower to learn dressing skills. It may seem
quicker and easier for mother or sister to simply put the clothes on her,
without interacting with the child. However, this will only delay the
child’s development more.
It is important to use dressing as an opportunity to help the
child develop in many areas at once: awareness, balance, movement, and even
language.
As you dress the child, talk to her. Help her learn her
body parts, the names of clothes, and the way these relate: “The arm goes
into the sleeve,” “The foot goes into the pants,” and so on. This
will help the child begin to learn language and connect parts of her body to her
actions and things around her.
Helping the child gain dressing skills takes time and patience.
Let her try to do as much as she can for herself. Be ready to help if it gets
too difficult, but only as much as is needed. It is not good to frustrate the
child so much that she will not want to try again. Be sure the task is not too
advanced for the child’s level of development.

Figure
POSITIONS FOR DRESSING
Try dressing the child in different positions, to see what works
best.
|
Body position is especially important when dressing a child with
spastic cerebral palsy. Often his body tends to bend stiffly backward if he is
dressed lying on his back.

A bad position: (child’s
body stiffens backward)
Hand bends tightly. (1) |
It often works better to dress a child with
spasticity with his body and hips bent forward.

A good position:
|
|
|
For changing that needs to be done face-up, try putting a
firm pillow under the head, and keep knees and hips bent. This may help the baby
relax and not stiffen up.

Figure
|
Lying on the side is often a good position for a child
with spasticity who is beginning to dress himself. He may need to roll from one
side to the other to pull on clothes - but he should keep his knees, hips, and
head bent to avoid stiffening.

Figure
|
|
|
To help the child dress while sitting, be sure he is in a
steady position. You can help him keep his hips bent and body forward like this.

first with help
|
If balance when sitting is still not good, or if the child tends
to stiffen backward, try sitting in a corner to dress.
then alone
|
Sitting with the feet forward and knees apart is a good position
for play and dressing. If legs press together stiffly, try pushing the knee (1)
out gently while you press under the big toe. (2)
Figure
|
|
|
When a child with athetoid cerebral palsy tries to raise her
arms or to speak, her feet may come off the ground or her legs spread.
Try pressing down over the knees, keeping them together. Or
press on top of the feet.

Figure
|
Help the child find the position that allows the best control
for dressing. |
|

Figure
|

Figure
|
Figure
|
SUGGESTIONS FOR DRESSING
· If one arm or leg
is more affected than the other, it is easier if you put the clothes first
· on the affected side. (1)
· Put the clothes where the
child can see and reach them easily, so he can help in any way possible.
(2)

Figure
· If the arm is bent
stiffly, first try to straighten it slowly, then put the sleeve on. (If
you try to straighten it forcefully or quickly, it may become more
stiff.)

This keeps the legs relaxed and
gives her better control.
· If the legs
straighten stiffly, bend them gently in order to put on pants or shoes.
· Begin any dressing activity
for the child, but let him finish it for himself. Little by little have him do
more of the steps. If he can do it all by himself, give him time. Do not hurry
to do it for him if he is struggling to do it himself. Praise him when he does
well or tries hard.
· Use loose-fitting,
easy-to-put-on clothing. Here are some ideas:
|

Figure
|

Figure
|
‘Tube socks’ (socks without heels, that stretch to fit
foot) are easier for the child to put on. |

Figure
|
|

Figure
|

Velcro
|
Figure
Press-together studs (snaps) are easier to open and close than
buttons. |
If buttons are used, use large buttons and make buttonholes
extra big.

Figure
|
· For children who
have poor finger control, make a simple tool to button and unbutton
buttons.
· For the child who
often puts her dress on backward, or her sandals on the wrong foot, try to build
in ‘reminders’ that will help her do it right. For
example:
|

Figure
|
Sew a colorful bow on the front of her dress. |
Figure
|
Draw half an animal on each sandal or shoe so that the 2 halves
make the whole animal when she puts them on right. |
· For the child who
has difficulty reaching his feet, a stick with a hook may
help.
|
Figure
|
An all-purpose tool

Figure
|
Ideas for shoes
· For toes that claw
up, or bend under, you can cut off the top of the shoe, or use a
sandal.
|

Figure
|

Figure
|
· Tennis shoes or
other shoes that open all the way down to the toes are easier to put on.
(1)
|
Figure
|
Figure
|
· If the foot
stiffens downward so much it is hard to get a shoe on, you can cut the back of
the shoe open and put the foot in from the back.

Figure
|
HOW TO TIE SHOES WITH ONLY ONE HAND
Figure
|
Chapter 38: Toilet Training
By ‘toilet training’ we mean helping a child
learn to stay clean and dry. A child is toilet trained when:
· He knows when he
needs to shit or pee (make stool or urinate) and has learned to ‘hold
on’ so he does not go in his clothing or on the floor (bowel
and bladder control).
· He tells people when he needs
to do his toilet, or (if he is physically able)...
· he takes himself to a special
place (pot, toilet, latrine, or at least outside the house), removes necessary
clothing, ‘goes’, cleans himself in the customary way, puts his
clothing back on, and does whatever may be necessary to get rid of the
waste.
Figure
‘Toilet training’ is important for the development
of a child’s independence and dignity. Yet it is very often neglected in
disabled and retarded children. Often we see children 5, 10, even 15
years old who are still in diapers (nappies) and who
are still completely dependent on their mothers for being changed and cleaned.
This situation is hard on both child and family. With a little instruction and
encouragement, we have found that many of these children have become
‘toilet trained’ in a few days or weeks. Many could have learned years
earlier.
The age when normal children become toilet trained varies
greatly from child to child. It also varies from place to place, according to
local customs, what clothes children wear (if any), and how much the family
helps. With training, many children can stay dry and clean by age 2 or 2½.
With little or no training, most normal children learn to stay clean and dry by
age 4.
Children who are developmentally slow, or physically
disabled, are often late in learning to stay clean and dry. This may be
partly due to their disabilities. But often it is because the parents
have not provided the opportunity, training, and help that the child needs.
For example, one mildly retarded deaf 10-year-old boy in Mexico still depended
on his mother to change his diapers. His mother had never seriously tried to
teach him and thought he could not learn. Yet with a little help from a village
rehabilitation worker, he became completely toilet trained
in 3 days!
Handicapped children should be helped to become as independent
as possible in their toileting. With help, most retarded or disabled children
can become completely toilet trained by ages 3 to 5.
Of course, children with severe physical disabilities
may always need help with clothing or getting to the pot. But they can
learn to tell you when they have to go, and do their best to ‘hold on’
until they are on the pot.
Children who lack bladder and bowel control because of spina
bifida or spinal cord injury have special problems. But even these children
can often learn some control and become relatively or completely independent.
The special problems and training of these children are discussed in Chapter 25.
WAYS TO MAKE TOILET TRAINING EASIER
1. Start when the child is ready
Just as training should not be delayed, it also should not be
started too early. If a child’s body is not yet able to control her bladder
and bowel, trying to train her can lead to failure and frustration - both for
the child and her parents. Normally a child is ‘ready’ by age 2 or
2½. But in some children, training may need to be delayed to age 3
or 4, or sometimes later.
Most children learn to keep clean a long time before they learn
to stay dry. However, because a child pees much more often than she shits, if
training aims at ‘staying dry’, ‘staying clean’ usually
follows.
There are 3 simple tests to check if your child is
‘ready’ for toilet training. These are: bladder control, readiness
to cooperate, and physical readiness.*
* These tests and many of these suggestions on
toilet training are adapted from Toilet Training in Less Than a Day.
Azrin and Foxx. Pocket Books, N.Y. 1974.
· Bladder
control
Does your child pee a lot at one time and not dribble every few
minutes?
Does he often stay dry for hours?
Does he seem to know when he is about to pee? (The look on his
face, holding himself between the legs, etc.) (1)

Figure
If the child does these 3 things (or at least the
first 2) he probably has enough bladder control and awareness of peeing to make
training possible.
· Readiness to cooperate.
To test whether the child has enough understanding and cooperation, ask her
to do a few simple things: lie down, sit up, point to parts of her body, put a
toy in a box, hand you an object, and imitate an action like hand clapping. If
she does all these things willingly, she is probably mentally ready for toilet
training.
· Physical readiness. Can
the child pick up small objects easily? Can she walk or move herself fairly
well? Can she squat, or sit on a stool, and keep her balance? If so, she is
probably physically able to do her toilet by herself. If not, she can probably
still be trained but may need physical assistance.

Figure
Most children more than 2 years old can pass these 3 tests. If
not, it is usually better to wait before trying toilet training, or to help the
child become more ready.
SPECIAL PROBLEMS
If the child still does not have enough bladder control or
awareness, it is best to wait until she is older. For example, some children
with cerebral palsy are slow in developing bladder control.
If the child does not hear or understand simple language,
or is mentally retarded, more of the training needs to be done by
showing and less with words. Special gestures or
‘signs’ need to be worked out for ‘wet’, ‘dry’,
‘dirty’, ‘clean’, and ‘pot’ or
‘latrine’. Instead of teaching by using a doll, it is more helpful to
have another child demonstrate toilet use.
If the child is stubborn, refuses to cooperate when asked
to do simple things, or often cries and screams whenever he does not get what he
wants, toilet training will be more difficult. Stubbornness and refusal to do
what they are told are common in many handicapped children - mainly because they
are often overprotected or spoiled. Before trying to toilet train such children,
it is wise to work first on improving their attitude and
behavior. This is discussed in Chapter 40.
If a child’s physical disability makes it difficult
for her to get to the toilet place, to lower her pants, to squat or sit, or to
clean her butt, various aids or ways must be looked for to help her become as
independent as possible. These will be discussed on the next pages.
2. Put the child on the pot at the times when she is most
likely to use it
Before beginning toilet training, for several days notice at
what time of the day the child shits and pees. Usually there will be
certain times when she usually does so - for example, soon after the first meal
of the day.
Begin to put her on the pot or latrine at these times,
encouraging her to make ‘poo’ or ‘pee’ (or whatever she
calls it).
Leave her on the pot until she ‘goes’ - or for no more
than 10 minutes.
If the child ‘goes’, clap your hands, kiss her, show
her what she has done, and let her know how pleased you are.

Figure
If she does not ‘go’, just ignore it. Do not scold or
make her feel bad, or she may begin to fear or dislike the pot, and refuse to
use it.
3. Reward and praise success
In toilet training - as in any form of education-it works better
to reward success than to punish failure. When the child shits or pees
where she should, give her praise, hugs, kisses and other signs of approval.
However, make sure that the child knows you are pleased with her, not
because she shits and pees, but because she is staying dry or dean. When
training, check the child often to see if she is ‘dry’ or
‘clean’. When she is, praise her. Also, teach her to check herself.

Figure
When the child has ‘an accident’ and wets or dirties
herself do not punish or scold her. It is better to quietly clean up the
mess or change her. At most, say something friendly (but not approving) like,
“Too bad! - Better luck next time!”
|
CAUTION: As a general rule, do not offer a
child candy, sweets or other food as a reward for doing something right. This
can lead the child to associate food with love or approval - and therefore to
make constant demands for sweets. Avoiding food rewards is especially important
for children whose disability makes them less active, so that they easily get
fat. Extra weight makes moving around harder for both child and parents. So...
DO NOT LET DISABLED CHILDREN GET OVERWEIGHT.

DO NOT GIVE FOOD AS A REWARD TO
CHILDREN WHO ARE FAT
For children who are thin and active, it may make sense to
sometimes give foods as rewards. But be sure to include healthful foods like
nuts and fruits - not just sweets. |
4. Guide the child’s movements with your hands - not
your tongue
When the child has difficulty carrying out a physical task - for
example, lowering his pants - do not do it for him (if it is something he can
learn to do for himself). And do not tell him his mistakes or how to correct
them. Instead, gently guide his hands with yours so that he learns how to do it
himself.

guiding the child’s
hands
5. Use models, examples, and demonstrations
Setting an example is one of the best ways of teaching -
especially if the example is set by persons the child loves, admires, and tries
to copy. Even before children are old enough to be toilet trained, help prepare
them by letting them watch their brothers and sisters use the pot or latrine.
Tell them that when they are big enough they will be able to do it that way too.

Figure
Using a doll that wets is another good way to introduce
toilet training. Dolls that ‘wet’ can be bought, or you can make one
out of,
|
a gourd |
or a baby bottle inside a homemade rag doll. |
|
|

Figure
|

when lying down, no pee
|

when sitting up, doll pees
|
Show the child how the doll pees in the pot. Or better, ask your
child to help you toilet train the doll. Be sure to include each step that will
be needed for the child to become as self-reliant as possible. For example:
|
First have the child show the doll how to get to the latrine or
pot - and then help the doll lower his pants.

Figure
|
Next have the child teach the doll how to get onto the pot, and
sit there until he pees. Try to make the situation as nearly like that of the
child as you can - using the same pot in the same place that he will use it.

Turn it into a game, but keep the
focus always on toilet training
|
|
|

Figure
|
After the doll has finished peeing, have the child pull up the
doll’s pants. Ask him to feel the doll’s pants and check whether they
are dry. If so, have him praise the doll. |
To repeatedly see real persons (not just dolls)
enjoy and be rewarded for using the pot or toilet is
especially important for a child who is retarded or who has language difficulty.
6. Adapt toileting to the special needs of the child
Many handicapped children can be helped to become independent in
their toileting if special aids or adaptations are made. Different
children will require different adaptations. However, the following are often
helpful:
· If the child has
trouble pulling down pants or panties - use loose fitting clothing with
elastic or ‘Velcro’ waist band.

Correct position of hands, for
lowering pants
for raising pants
· Use short
‘training pants’ made of towel-like material that will soak up
urine.
Figure
· For a child with
cerebral palsy or spina bifida, it may be easier lying down - you might provide
a clean mat.

Figure
· If people by
custom squat to shit, and the child has trouble, a simple hand support can
help.
Figure

Some children, like this girl
with cerebral palsy, need to sit. This potty seat was adapted from a
child’s wood chair.
· Latrines can also
be adapted
|

Figure
2-seater latrine with child-sized hole and step |

Figure
|
Make the outhouse (latrine) and its door big enough
so that a wheelchair can fit inside. Position the door so that the wheelchair
can enter right beside the latrine without having to turn around.
Be sure the path to the latrine is level and easy to get to from
the house.
· A simple pot or
‘pottie’ is one of the best aids for toilet training of young
children. It can be adapted in various ways for disabled children.
|
simple pot |
more complex pots sold in some countries
These give good back support. (1) |
‘Baby Relax Toilette’ with removable pot -
gives good back and side support. |
|

Figure
|

Figure
|
Figure
|

Figure
|
|
For the child severely disabled with cerebral palsy, the pot can
be placed between mother’s knees. This provides good back support. Mother
holds his shoulders forward, his hips bent and his knees separated.

Figure
|
Later it may be possible to put the child on a corner seat like
this - which also holds arms and shoulders forward and helps keep hips bent.

bucket
|
A cardboard box can also make a good sitting frame.

Figure
|
Use your imagination and whatever materials you can get to make
it easier for your child to do it by herself.
For severely handicapped children, ‘toilet seats’ can
be built into specially designed chairs.
|

Figure
shelf for pot (1) |

Figure
|

Put a shelf for the pot.
|
|

Figure
For the child who cannot sit up, you might make a wedge-shaped
toilet box like this. |

It works as a
‘bedpan’,
|
|

Figure
An old plastic bucket can be cut at the same angle as the bedpan
so that it fits snugly under the hole. |
or as a ‘floor pan’ for the child who can roll or
scoot but cannot sit or lift himself without help. This way the child can learn
to take care of his own toilet.

Figure
|
|
For the child who has
spasticity or poor balance, you can make a seat like this.
The bar can be put in after the child has been seated. |
Figure
|
The seat can be made to fit over a bucket, over a floor-hole
latrine, or over a standard toilet or on a wood or metal frame over a toilet
seat. |
Tire potty seat - soft, safe, washable*
* Ideas from India-UPKARAN manual.
|
Tire can be used alone,
Figure
|
or over a ‘hole-in-the-floor’ toilet,
Figure
|
or on metal frame over a toilet seat. |

Figure
|
Try to pick size of tires to match the size of the child. For
small children, scooter or very small car tires may work well.
|
Cane or rattan toilet seat with climb up bars*

Figure

Figure
|
Enclosed wood or plywood toilet*

Figure
|
REMEMBER: As the disabled child grows, she
will feel the same need of privacy as any child would for toileting and other
personal acts. Help the child to obtain the privacy she needs.
* Ideas from India - UPKARAN
manual.
Chapter 39: Bathing (includes Care of the Teeth and Gums)
Regular bathing is important for all children. Bathing
the severely disabled child, however, is often not easy. Children whose bodies
get stiff or whose knees pull together may be very difficult to clean. As the
child gets older and heavier, the difficulties often increase. Here are some
aids and ideas that may make bathing easier.
For the baby or small child, some kind of a tub may be a
big help.
|

Figure
A rectangular tub of the size you need can be made out of mud or
mud bricks (or dried bricks) and covered with a thin layer of cement. |

Figure
This is a good way to hold the child who
stiffens and bends backward, or throws open her arms when you pick her up. |
|

A mother bathes her child in a
cement wash tub. (PROJIMO)
|
A baby that tends to stiffen backward can sometimes be held like
this for bathing.

Figure
|
|
Gently spread the child’s legs as
wide as possible to clean between them. Also, lift arms high above the head. In
this way, bathing can be combined with range-of-motion exercises (see
Chapter 42).

Figure
|
|
IMPORTANT: Talk or sing to the baby as you
bathe her. Tell her each thing you do, and the name of each body part you wash,
even if she cannot understand. A child must spend a long time listening before
she can say her first words. So get an early start. |
As the child grows, make every effort to help her take
part in bathing herself. Help her do more and more until she can bathe herself
without help, if possible.
|
Our goal in bathing is SELF-CARE, even for the child who is
fairly severely disabled or retarded. |
For many children balance is a problem, even while
sitting. Anything that can help the child keep his balance, and stay in a
position where he has the most control, will help make bathing easier. Here
are some aids and suggestions for helping the child manage better.
|
The child who has trouble sitting because she stiffens backward
may need some kind of back support to sit while bathing. |

Figure
|
|
CAUTION: Be sure water is clean and does not
spread disease. |
|
2 old car tires (or inner tubes) tied together

Figure
|
Note: Anything that keeps the hips bent up
like this will help keep a child with spasticlty from
stiffening and bending backward. |
Especially for the child who does not have good
bowel or urine control, it is very important to carefully
clean her butt and between her legs. An inner tube on
poles, like this, holds her in a good position for washing.

Figure
|
|
a bath seat made from half a plastic bucket or laundry basket on
a tube frame

Figure
|
a stool with a seat woven from strips of car tire inner tube

Figure
From the UPKARAN Manual. |
a washing platform of wooden slats for the child who washes (or
is washed) lying down
Figure
Also see the bicycle inner tube mat. |
|
A soap mitt, made of a piece of towel and a tie string (or
Velcro straps), lets the child who has difficulty grasping
use both the washcloth and soap more easily. |
Figure
|
Bath time is a good time to help a child develop many
different skills. Encourage her to handle and play with toys in the water,
repeat words, and imitate actions. Let her feel the difference between a sponge
and a cloth, or dry and wet and soapy. To learn to use both hands together, let
her squeeze water out of the sponge.
To help the child learn how to bathe herself, let her first wash
her toys and dolls. Show her how and encourage her to copy you.
For a child who is afraid of the water, letting her bathe a doll
or toy first may calm her fears.
Toys that float in the water make bathing more fun. Use
corks, bits of wood, or plastic bottles with lids on them. Making little boats
with sails or ‘paddle wheels’ makes it more fun and helps the child
learn to use her hands better. The child with weak lips or who drools can play
by blowing the boat across the water.

Figure
For the child with limited control or strength, it is often
easier to play in the water with toys that float than it is to play with toys
out of the water.
|

Figure
|

Figure
|
Drying the child can also become a game that aids development.
Rub the child, sometimes gently and sometimes briskly, with a rough cloth or
towel. Name the different parts of her body as you rub them. Remember, as you
bathe and dry the child, talk about each thing you do - or sing a song about it!
Move the towel with the music, and encourage the child to move with you. Use
your imagination to make it more fun and to help her learn.
|
Use bath time as an opportunity for learning and play.
|
CARE OF THE TEETH AND GUMS
Many disabled children develop problems in their teeth and gums.
There are many reasons:
· In children who
have poor mouth and tongue control, food often sticks to gums and teeth and is
not cleaned away by the natural movement of the tongue.
· Many disabled children (even
those with no eating problems) are fed soft, sticky ‘baby foods’ long
after they should be eating rougher, more solid ‘adult foods’. So,
their gums get soft, weak, and unhealthy.
· Sometimes children with
disabilities are ‘spoiled’ by giving them extra
sweets - which increases tooth decay.
· Some medicines for fits
(epilepsy) cause swollen, unhealthy gums.
· Dental care is
more difficult in some disabled children - especially those with cerebral palsy.
(In some places, dentists refuse to care for these children.)
For these reasons, we must take care to keep the gums and
teeth of the disabled child healthy and clean.
STEPS IN CARING FOR GUMS AND TEETH:
1. Avoid foods and drinks with lots of sugar
- especially between meals.
2. Start child on solid food as early as he can take them.
Toast, crackers, carrots, raw fruit, and other foods that rub the teeth and
gums clean are especially helpful.
3. Clean the child’s teeth and gums, if possible
after every meal.
|
Before the baby has teeth, clean his gums with a soft cloth over
your finger. First, dip the cloth in boiled water with a little salt or baking
soda in it. |
After the child has teeth, clean them with a small, soft
toothbrush. Or use a piece of thick cloth or a bit of towel wrapped on a stick.
Figure
Or use a stick from a Neme tree or other non-poisonous plant.

Figure
|
Toothpaste is not necessary. Instead you can use salt, salt
mixed with baking soda, or a burned and powdered piece of bread, chapati, or
tortilla, or just water.
Clean all surfaces of the teeth well, and also rub or brush the
gums. |
|

RIGHT
|

WRONG
|
|
|
|
This is a good position to clean the child’s teeth and
gums. Be sure the head bends down. |
If his head bends up, he will be more likely to choke or gag.
|
|
|
4. Help the child learn to do whatever she can to clean her own
teeth and gums. At first you can guide her hand, then have her do a little more
each time, and praise her when she does it well.
The child will be more likely to clean her teeth regularly if
you have a special place, adapted to her needs.

Figure
|
REMEMBER: Brushing the gums is just as important as
brushing the teeth! |
For more information, see Where There Is No Dentist,
Chapter 5, “Taking Care of Teeth and
Gums”.
Chapter 40: Ways to Improve Learning and Behavior
“I still feed Ra�l myself because when I let him try to eat
by himself he throws his food all over the place. The more I punish him the
worse he gets.”

Figure
“Erica begins to cry and scream every time I put her down
for a minute. It’s worse when I take her out where there are other people.
At the river she has such tantrums that I can’t finish washing the
clothes.”

Figure
“Jorge is always starting fights with other children or
doing other bad things - at home and in school. He seems to enjoy making people
mad at him!”
Figure
These and other behavior problems can occur
in both non-disabled and disabled children. But some disabled children have
special difficulty learning acceptable and appropriate behavior. Children who
are mentally retarded may develop poor behavior because they are
confused by the unclear or conflicting messages they get from their parents and
others. Children who are physically disabled sometimes act in
‘naughty’ or self-centered ways because they have become dependent on
others to do things for them. They lack self-confidence, and are afraid of being
forgotten. On the other hand, children who are often neglected or ignored when
they are quiet and behave well, may learn to behave badly to get attention.
As a rule, if children repeatedly behave badly, it is because
they get something satisfying or rewarding from their bad behavior. Therefore,
to help children learn acceptable behavior, we need always to CLEARLY LET THEM
SEE THAT ‘GOOD’ BEHAVIOR IS MORE SATISFYING THAN ‘BAD’
BEHAVIOR.
In this chapter we explore ways to do this, using a
‘behavioral approach’ which you can divide into 5 steps:
1. Carefully observe the circumstances of your
child’s unacceptable behavior.
2. Try to understand why your child behaves as he does.
3. Set a reasonable goal for improvement based on his immediate
needs and his developmental level.
4. Plan to work toward the goal in small steps, always rewarding
‘good’ behavior and making sure ‘bad’ behavior brings no
pleasure, attention, or reward.
5. After the child’s behavior has improved, gradually move
toward a more natural (less planned) way of relating to him.
A BEHAVIORAL APPROACH TO LEARNING AND IMPROVED BEHAVIOR
Step 1. Observe the circumstances of your child’s
behavior.
To help your child to behave more acceptably, start by carefully
observing what is happening around and with the child when he begins his acts of
disturbing behavior. Observe carefully for a week or two. To notice
patterns more clearly, it helps to write down your observations. Try to
make your records clear, specific, and simple. Take note of everything
that might lead to your child’s acts of ‘bad’ behavior, and
what he seems to gain from it. For example, Ra�l’s mother might
write these notes:
|
Figure
|

Figure
|

Figure
|
|
“I put him in his chair, and gave him food.” |
“Then I got the older children ready for school.”
|
“He kept calling to me, but I was busy and told him to keep
quiet.” |
|

Figure
|
Figure
|

Figure
|
|
“Ra�l began to throw his food!” |
“I slapped him.” |
“He started crying. To quiet him, I fed him his
breakfast.” |
“Then I put him down to play with his toys.” |
Step 2. Based on your observations, try to figure out why
your child behaves as he does. Look for answers to these questions:
· What happens that
leads to or ‘triggers’ his unacceptable behavior?
· Is his behavior partly due to
confused or unclear messages from you or other persons?
· What satisfying results
does his behavior produce that might make him want to do it again?
· Is the child’s behavior
partly from feeling afraid or insecure?
By repeatedly observing what happened before Ra�l began to throw
food, his mother started to find some answers:
· “Ra�l throws
food most often when I leave him alone with it - especially when I am busy with
the other children.”
· “My own messages to Ra�l
are confusing and contradictory. At the same time that I scold him, I also give
him the attention and care that he wants - like feeding him as if he were still
a baby.
· By throwing food, Ra�l gets a
lot of satisfaction.
POSSIBLE EXPLANATION FOR RA�L’S FOOD THROWING
|
TRIGGERS
· Ra�l is being ignored. He is
left out while his mother is busy with the other children.
· He may be afraid that if he
feeds himself, he will be left out even more. He is very dependent on his
mother’s care and attention. |
WHAT HE LOSES BY THROWING FOOD
· His mother gets angry, slaps,
and scolds him.

Figure
|
WHAT HE GETS
· He gets the whole
family’s attention.
· His mother quickly leaves the
other children and goes to him.
· If he cries when she slaps or
scolds him, she quickly comforts him and cares for him like a baby.
· And then he gets to play with
his toys.
· By being fed like a baby, he
calms his fears of growing up and losing his mother’s care and attention.
|
Step 3. Set a goal for improvement of the child’s
behavior.
If the child has several different behavioral problems, it is
usually best to try to improve one at a time. Be positive. Try to set the
goal in terms of the good behavior that you want, not just the bad behavior
that you wish to end. For Ra�l, the goal might be ‘to learn to feed himself
quietly’ (not simply ‘to get him to stop throwing his food’).
Be sure that goals are possible for the child at his
developmental level.
Step 4. Plan a way to help the child improve his
behavior.
Consistently reward ‘good behavior’. Each time
the child behaves as you want, immediately show your appreciation.
Rewards can be words of praise, a hug, a special privilege (perhaps the
chance to play with a favorite toy). Or give the child a bit of favorite food.
However, food rewards should mostly be used only for very thin children or if
nothing else works. Avoid giving food as rewards to fat children.
As much as possible, ignore rather than punish
‘bad’ behavior. Rewarding ‘good’ behavior rather than
punishing ‘bad’ behavior brings improvement with much less bad feeling
for both parent and child.
Always reward ‘good’ behavior and never reward
‘bad’ behavior. This is the key to the behavioral approach.
For example, whenever Ra�l eats by himself, without throwing his
food, the whole family can applaud and praise him.

Ra�l finds that good behavior
brings rewards and attention.
But whenever he throws his food, the family ignores him, except
perhaps to say “I’m sorry you did that, Ra�l,” or, “Once
more and I’ll have to take your food away because I’m tired of having
to clean up the mess.” (Make this a result, not a punishment.) Always do
what you say you will do.
He quickly learns that throwing
his food now brings no reward.
ADDITIONAL GUIDELINES:
· Be consistent
in how you respond to your child’s behavior. If you sometimes reward
good behavior and at other times you ignore it, or if you sometimes ignore bad
behavior and at other times either scold or do what the child demands, this is
confusing. His behavior is not likely to improve.
· WARNING: When
using this approach, at first the child may actually behave worse. When
Ra�l does not get his mother’s attention by throwing his food, he may try
throwing his bowl too. It is very important that his mother not give in to his
demands, but rather be consistent with her approach. Only if she is consistent
will he learn that he gets more of what he wants with ‘good’ behavior
than with ‘bad’.
· Move towards the goal
little by little, in small steps. If steps forward are small and clearly
defined, often the child will learn more easily, and a beginning period of worse
behavior can sometimes be avoided.
For example, it would be too much to expect Ra�l to suddenly eat
by himself quietly when mother is busy with the other children. Instead, mother
can help him work toward this goal little by little.
|
A possible first step is for Ra�l’s mother to give him his
food after the other children have left for school. This way she can stay close
to him as he eats it. |
The next step might be for mother to do her work while Ra�l
eats, but to keep talking with him and praising him when he does well. |
|

Figure
|

Figure
|
In this way, Ra�l will learn that eating by himself does not
mean being left alone, but gets more attention from his mother than does
throwing food.
Step 5. After the child’s improved behavior has become a
habit, gradually move toward a more natural way of relating to the child.
To help the child improve his behavior, the ‘behavioral
approach’ just described often works well. Your responses to your
child’s acts are carefully planned and consistent. However, such a
controlled approach to person-to-person relationships is not natural. Parents
and children, like other people, need to learn to relate to each other not
according to a plan, or because each action earns a reward, but because they
enjoy making each other happy.

Figure
Therefore, the last step, after the child’s new behavior
has been established, is to gradually decrease immediate rewards while
sharing the pleasure of an improved relationship.
Setting reasonable goals - based on the child’s
developmental level
Be realistic when setting a goal for improvement in behavior, or
a new skill that you want your child to learn. First try to determine the
child’s developmental level, and set a goal consistent with that level. (To
determine the child’s developmental level, see Chapter 34, “Child
Development and Developmental Delay.”)
Consider Erica, the girl who has tantrums
(crying and screaming fits) whenever her mother puts her down. Erica is
retarded, which means she is developmentally slow for her age. Depending on her
developmental level (not her age), her mother can plan steps to
help her avoid tantrums:
|
Suppose Erica is at the development level of a very young
child.
She has poor hand control and no ability to play by herself, or
to imitate (to copy) others. She will need to begin with very basic steps and
clear, simple messages. Her mother can put her down briefly, then praise, talk,
or sing to her as long as she does not have a tantrum. When she does have a
tantrum, her mother should try to give her as little attention as possible, and
never give in to her demands. She can pay attention and reward her during those
moments when she stops screaming - if only to catch her breath. This way Erica
will begin to learn that she gets more of what she wants through good behavior
than through tantrums.
Figure
|
Now suppose that Erica is at a more advanced level of
development. She likes using her hands and imitating her mother. Steps for
improving her behavior can start from this level. Perhaps her mother can have
Erica sit at the river’s edge and pretend to help her mother wash clothes.
This way Erica will feel closer to her mother and will be less afraid of being
left alone. Her mother can talk to her and praise her all the time.

Figure
Note: At this level, Erica will not be able
to stay with one activity for very long. To avoid tantrums, her mother will need
to keep the activities interesting by changing them often, and talking to her a
lot. In all of this, other children can be a big help. |
Helping the child make sense of his world
The ‘behavioral approach’ to learning and
development that we have discussed is similar to what is called
‘behavior therapy’ or ‘behavior modification’. However, we
prefer to put the emphasis on improving communication to help the child
make sense of the world around him. Instead of our ‘changing the
child’s behavior’, we would rather help the child to understand
things clearly enough so that he chooses to act in a way that will make life
more pleasant for everyone.* To achieve this, parents first learn to
understand and change their own behavior in relating to their child. They look
for ways to communicate with the child that are consistent and supportive, and
that reinforce good behavior.
* This is the point of view in Newson and
Hipgrave’s Getting Through to Your Handicapped Child,
from which many ideas in this chapter are taken, and which we strongly
recommend.
A behavioral approach can often help children who are
mentally retarded or developmentally delayed, such as Ra�l and Erica, to
relate to other persons better and to learn basic skills more quickly.

Giving lots of attention,
encouragement, and praise when he makes an effort is one of the best ways to
help a child learn new skills. Photo by Sonia Iskov from Special Education for
Mentally Handicapped Pupils.
The approach can be used at almost any age. It is often
easier with younger children (developmental age from 1 to 4). Starting at a
young age can prevent small behavioral difficulties from becoming big problems
later. For the very young or severely retarded child, goals must be kept basic,
and progress toward the goals must be divided into small steps. To master each
step, much repetition may be needed with consistent praise and rewards
for each small advance.
Mentally normal children with physical disabilities
sometimes also develop unacceptable patterns of behavior. A behavioral
approach may help them also. The story on the next page tells how this approach
helped Jorge, to behave better.
|
THE STORY OF JORGE |
|
Jorge is an intelligent 10-year-old whose legs are paralyzed by
polio. He lives with his grandmother. He is noisy, rude, bad tempered, and
whenever he plays with other children, it turns into a fight. Jorge has caused
so much trouble in the classroom that his teacher recently told his grandmother
he will throw Jorge out of school if he does not change. Both his teacher and
grandmother have tried scolding him and whipping him, but it only seems to make
Jorge’s behavior worse. As his grandmother says, “He loves to make
people angry at him.”

Figure
Not long ago, Jorge’s grandmother took him to the village
rehabilitation center to ask for advice. A village worker helped her to observe
both Jorge’s and her own behavior more closely to better understand why
Jorge acts the way he does. She realized:
· When Jorge is
quiet and well-behaved (which is not often), everyone ignores or forgets him.
· As a result, Jorge feels
unwanted, unloved, and useless. Starved for emotional human contact, he gets it
by making people angry with him.
· Jorge’s bad behavior,
therefore, brings him a lot of person-to-person contact, even though it is
painful. The few times he tries to be good, he is made to feel unwanted and
unneeded.
“I really do love him,” said his grandmother.
“But I guess I don’t show it much. He makes me worry so much!”
To begin to behave better, Jorge needed to find out that
friendly and helpful behavior can bring him closer to people than bad behavior.
For this reason, the village worker - together with the grandmother, the
schoolteacher, the schoolchildren, the rehabilitation team, and Jorge himself -
helped figure out ways that would let the boy see that ‘good’ behavior
is better than ‘bad’ behavior. |
At home, grandma began to look for things Jorge could do
to help her, and to show him how happy she was when he did them. She made a
backpack, open at the sides, so that he could help bring firewood. Also, she
learned to quietly turn her back when he misbehaved, and to let him know how
happy she was when he would sit quietly doing his homework or shelling the
maize.

Figure
At school, the teacher discussed with the other children
ways to include Jorge in their games. When they all played football (soccer),
they let him be ‘goalie’. To everyone’s surprise, Jorge was an
excellent goalie. With his crutches he could reach farther and hit the ball
farther than anyone else. Soon all the children wanted Jorge to play on
‘their team’. At first Jorge started a few fights. But when he did, he
was quietly asked to sit on the sideline. Soon he learned to stop hitting other
children so that he could keep hitting the ball.

Figure
In the village rehabilitation center, the village worker
invited Jorge to help make educational toys for young and disabled children. He
helped Jorge get started and praised him for each toy Jorge completed. Soon
Jorge learned to make the toys by himself and took great pride in his work. When
he saw other disabled children playing and learning things with his toys, it
made him very happy. He decided he wants to be a rehabilitation worker when he
grows up.

Figure
|
Time Out’ or ‘non-reward’ instead of
punishment
The story of the way family and friends used the ‘behavior
approach’ to help Jorge sounds fairly straightforward and simple. But in
real life it is seldom that easy. ‘Bad’ behavior may sometimes be so
bad that it cannot be ignored.
In general, the best way to make ‘bad’ behavior seem
boring to the child and not worth the trouble is to give no rewarding response.
At the same time, make sure to reward ‘good’ behavior. This means
everything satisfying stops as a result of ‘bad’ behavior (instead of
the usual situation where everything satisfying starts).
For example, when Ra�l throws his food, instead of entertaining
him by scolding and feeding him, his mother should remove both the food and
herself for 3 or 4 minutes - making the situation as boring as possible.
Removing food may seem like punishment. But it is best to aim at
making the situation less interesting rather than making it unpleasant.
To make things less interesting, sometimes we may remove the child from the
situation for a brief time. This is often called ‘time out’.
For example, when Jorge’s grandmother first began using the
behavioral approach, to try to make her angry he would shout and hit the
chickens with his crutches. But instead of her usual scolding, grandma now
simply told him that if he did not quiet down she would ask him to take
‘time out’ in the corner. Then, if he continued to make trouble, she
would lead him to the corner and tell him that he would have to stay there for 5
minutes from the time he was quiet. She set an old alarm clock to ring in 5
minutes. At first Jorge would continue to shout from the corner, but each time
he did, grandma would set the alarm to ring in another 5 minutes from the time
he was quiet. Meanwhile she gave him no attention and continued her work.

Figure
In this way Jorge learned while he was in the corner that the
only way to make life interesting again was to stop making a disturbance.
Because he was clever, he learned fast. (Slower children often take longer.)
We should try to use ‘time out’ as a
‘non-reward’ and not a punishment. However, because time out is
something an adult makes a child do, it can seem like punishment. Try to use it
only when less forceful methods of avoiding rewards do not work. It is best to
start with a ‘time out’ period of no more than 5 minutes (less for a
very young child). If the child does not behave better in 5 minutes, consider
with the child adding another 5 minutes. Never leave the child in ‘time
out’ for more than half an hour, even if he has still not become quiet.
|
CAUTION: For a child who is younger than 5 years old
or severely retarded, do not extend time out to more than 15 minutes, checking
frequently with the child to see if he is ready to behave acceptably. |
A BEHAVIORAL APPROACH TO CHILD DEVELOPMENT AND LEARNING NEW
SKILLS
In this chapter we have talked mainly about correcting
‘bad’ behavior. However, the behavioral approach can also be used to
help children learn basic skills for their continuing development. The approach
is often useful for children who are slow to develop - for either mental or
physical reasons.
In Chapter 34 on child development, we introduced the key
features of a behavioral approach: (1) make messages clear, (2) consistently
reward things learned, and (3) advance toward new skills through small steps.
You will also recognize this behavioral approach in the chapters on
‘feeding’, ‘dressing’, and ‘toilet training’. Here
we would like to review ways of applying a behavioral approach to a child’s
basic development and learning.
Looking at the whole child to decide where to begin
In considering how to help a child’s development, start by
looking at what the child can and cannot do. In terms of behavior; we can group
our observations into 4 sections:
|

Figure
|
· Positive behaviors:
Skills and characteristics the child now has - particularly those that may
help him in learning something new. (For example, he enjoys being praised.)
|
|

Figure
|
· Negative behaviors:
Things he does that are dangerous, disturbing, or prevent his progress. (For
example, breaking things, hitting people, screaming when bathed, throwing toys
rather than playing with them.) |
|

Figure
|
· In-between behaviors:
These have both positive and negative aspects, and need to be worked with to
make them more positive. (For example, for a child who is beginning to feed
herself, but who smears food all over: we encourage feeding herself (which is
positive), but not smearing (which is negative). Even screaming or crying in
order to express a need might be considered positive for a child who has great
trouble communicating. We need to help this become more satisfactory
communication.) |
|

Figure
|
· Key needs: These are
problems in the child’s behavior that need to be solved to make progress
with learning. They differ depending on the stage of development. (For example,
for a child to learn from his mother, he needs to respond to his own name, to
look at her when she speaks to him, and to stay still and give attention for at
least a few seconds. These ‘key needs’ suggest the first steps in
learning to speak, play, or develop new skills.) |
It may help to write a list of these different behaviors. Here
is a list that a little girl’s mother made with the help of a village
health worker who studied this book.
Child: Celia
Age: 4

Figure
|
POSITIVE BEHAVIORS - ones she now has that we can build
on
· smiles when praised

Figure
· can feed herself with her
fingers
· can put 3 rings on a peg

Figure
· undresses herself
· enjoys rough play
· enjoys being bathed
· says 6 words: mama, dada,
bottle, sweets, pee-pee and NO! |
IN-BETWEEN BEHAVIORS-ones that have both good and bad
points
· plays only a moment with
toys-then throws them
· says ‘pee-pee’, then
wets her panties

Figure
· will not sit still for
a minute - except for food |
NEGATIVE BEHAVIORS-ones that prevent her progress or disturb
the family
· kicks people when she gets
upset
· carries around a baby bottle
all the time, and screams when it is taken away
· spits her food at others

Figure
|
|
KEY NEEDS (in order that new skills and behavior can
develop)
· sitting down and giving
attention for a longer time
· getting rid of
the baby bottle to free hands for other things |
Deciding where to begin
After they listed these behaviors and considered Celia’s
key needs, the health worker helped her mother plan where to begin. He explained
that, since we cannot change everything at the same time, we need to
decide what things need to be done first (choose priorities for action).
So we choose the behavior we most want to introduce or change.
· If we are trying
to introduce a new behavior or skill, we need to think of all the
different parts that make up the behavior. Next we plan the separate
small steps that lead to the skill. We encourage the child to advance
step by step, making clear what we expect for each step and consistently giving
praise and small rewards.
· To improve an
‘in-between behavior’, we can help the child by working with a
skill she has already developed a little. First we need to think about the
various parts of her behavior that concern us. Then we decide which
parts seem helpful and which do not. We then reward the good behavior and
ignore the bad. As the child gradually improves, we can expect more of her
before giving a reward, until the whole improved behavior is achieved.
· If we are trying to reduce
or stop an old behavior we need to do 2 things. First we note when and
where the behavior happens, and what happens before, during, and
afterward. We observe carefully both what the child does and what we
ourselves do. Second, we try to guess what the child gains from her
‘bad’ behavior. We can then try to change things so that
‘good’ behavior is more worthwhile than the ‘bad’. To do
this we reward the new ‘good’ behavior and refuse to give attention
for her ‘bad’ behavior.
Thinking about Celia’s behavior, her mother realized that
she already has the beginnings of many valuable skills. She uses her
hands well and has begun to develop skills for feeding and dressing
herself. She also speaks a few words - although it would be nice if
she could say “yes” as well as “no.”
It is important that she likes praise and hugs, and
bathing, and rough play. This means she will probably learn well with a
reward-based approach.

Figure
However, certain things seem to be stopping Celia from
developing her skills more. Not being able to sit still and give attention makes
it hard for her to learn from other people, or even to learn to enjoy her toys
(which she always throws). Also, her baby bottle is a big problem. She is
much too old for it, but her mother is afraid to take it away because Celia
screams. Her mother fills the bottle with sweet drinks (which have already begun
to rot Celia’s teeth). The biggest problem is that by always holding her
bottle, Celia’s hands are not free to do other things - such as play with
her toys or take down her panties when she has to pee-pee.

Figure
For these reasons, Celia’s mother decided that the
‘key needs’, which need to be solved in order to advance in other
areas, are:
· helping Celia
learn to sit quietly and give her attention to something
· helping Celia grow out of her need to always hold her
bottle
The health worker discussed with Celia’s mother what she
might do. To help Celia learn to sit quietly and pay more attention to things,
her mother decided to start with the times when Celia was already willing to sit
fairly quietly - which was mealtime and bathtime. For example:
|
After giving Celia her food, but before her final
‘sweet’, her mother or her older brother, Oscar, plays quietly with
her for 5 minutes or so, praising her whenever she gives attention.

Figure
|
Her mother also uses bathtime as an opportunity to help her
concentrate on toys and to give attention to words and sounds.

Figure
To make a paddle wheel boat. |
Celia’s mother decided to help her outgrow the bottle
little by little. For a start, she filled it with water only. After a few days,
she refused to fill it at all.
At first Celia screamed and kicked. But her mother did her best
not to give Celia any attention when she acted that way. As soon as Celia was
quiet, however, she would give her a tasty drink from a glass, or some other
reward.
Sometimes Celia would throw her empty bottle in anger. But after
a while she began putting it down, more and more often, to pick up other toys or
objects. Finally, her mother simply removed the bottle from sight.

Figure
After Celia had forgotten her bottle, she started to explore
more with her hands. When she needed to go ‘pee-pee’, she began to
lower her panties by herself; in a few weeks she was ‘toilet trained’.
She also began to play with her toys more, instead of just throwing them. As she
learned to give longer attention to things, she discovered lots of things that
gave her pleasure. Many of her behavior problems such as screaming, spitting
food, and kicking began to disappear. Her mother, father, and brother spent more
time playing and talking with her. They praised her when she behaved well, and
did their best to ignore her ‘bad’ behavior.
Where it seemed necessary, her mother began to use a behavioral
approach to help Celia develop other skills: dressing, eating, and talking. To
increase her language skills, together they looked at picture books and listened
to songs.

Figure
As a result of her family’s efforts, Celia has grown up a
lot, and is a much happier and more able little girl. Thinking about the changes
that took place, her mother said, “I think my behavior has changed as much
as Celia’s. I was still treating her like a baby - bottle and all! Now that
I expect more from her and show her how much I appreciate her effort, she has
developed a lot faster, and is a lot easier to live with. She and I have both
come a long way!”
Examples or methods for helping children develop basic skills
using a behavioral approach are discussed in other chapters: Feeding, Chapter
36; Dressing, Chapter 37; and Toilet Training, Chapter 38. We suggest you also
read again the chapter on child development, Chapter 34, and consider how a
behavioral approach can be useful for helping a child through many difficult
areas of development.
PARTICULAR BEHAVIOR PROBLEMS THAT OCCUR IN SOME DISABLED
CHILDREN
Tantrums
‘Tantrums’ are fits of crying, screaming, and angry or
destructive behavior. The child may try to break, throw, kick, bite, or in other
ways damage anything or anyone within reach - sometimes including himself.
Tantrums can be frightening, both to the child and the family.
After a tantrum begins, it is difficult to ‘reason’ with the child and
calm him. Punishment often makes it worse.
Children - including some retarded and physically disabled
children - may learn to use tantrums to get what they want. Erica, is one
example. Here is another:
|
Kwame has been left to play by himself. He tries to get Mama to
come give him attention.
Figure
|
So Kwame has a tantrum.

Figure
|
Afraid he may hurt himself, Mama comes running to the rescue.
Now Kwame has her full attention.

Figure
|
|
REFUSING ATTENTION HERE
|
AND GIVING IT HERE® |
ENCOURAGES
‘BAD’ BEHAVIOR |
In this way children discover that tantrums get them what they
want. To help a child have fewer tantrums, parents need to help the child find
other, more acceptable ways of showing his wants and fears. And most important,
parents need to reward the acceptable ways, and at the same time
refuse to give the child attention when he is having a tantrum.
Let’s look at how Kwame’s mother learned to do this:
|
When Kwame acts nicely:

Figure
|
But when he has a tantrum:
Figure
|

Figure
|
|
GIVING ATTENTION HERE
|
AND REFUSING IT
HERE® |
REINFORCES ‘GOOD’ BEHAVIOR
|
Thus, by rewarding Kwame’s good behavior and by refusing to
give attention to his demands when he does have tantrums, Kwame’s mama
helped him learn that tantrums do not get him what he wants. At first he
had more violent tantrums than ever. But when even these failed to give exciting
results, little by little he stopped having tantrums. He found that other forms
of communication gave more satisfying results.
Holding breath
“Not giving attention during a tantrum sounds very nice.
But my child gets so angry, he stops breathing and turns blue! I
can’t just do nothing!”
But doing nothing is often the best way to prevent your child
from holding his breath more often!

Figure
The child will not hurt himself by holding his breath. At
worst, he will lose consciousness and begin to breathe normally, long before the
lack of air causes any damage.
Once a child learns that holding her breath frightens and
confuses her parents, she is likely to repeat it every time she gets angry at
them. (Many completely normal children do this.) We need to try
not to show worry or concern when the child holds her
breath and turns blue. Instead, we should wait until she gives up trying to
frighten us and begins to breathe normally again. Then we can do something to
show her how much we love her. But not while she is holding
her breath!
Head banging, biting, and other self-damage
Children may do these things for the same reason they hold their
breath - to frighten and punish their parents.

Figure
Sometimes, however, children with brain damage, epilepsy or
severe mental problems may form habits of biting themselves, banging their
heads, pulling out their hair or other self-destructive behavior.
Whatever the cause, acts of self-destruction cannot be ignored.
Parents should look for the most simple and calm way possible to gently stop the
child from injuring herself. For example, they can hold the child’s arms to
keep her from biting herself.

To stop a child who is hurting
himself, hold him from behind tightly, but quietly, so that he does not see you
and gets as little response from you as possible.
However, often a behavioral approach helps solve these problems.
Take care not to get excited or give the child extra attention when she
hurts herself. At the same time, make every effort to reward positive behavior
and to help the child gain self-confidence, learn new skills, play with toys and
other children, and have friendly interaction with other people. Of course, some
children’s mental ability will not allow much learning or play. Showing
these children a lot of affection, hugging them, talking and singing to them,
and doing things with them that they like, at times when they are not harming
themselves, may help them to stop such acts. Rewarding a child when she
stops a self-destructive act may help a child to not act that way so often.
But be sure to reward and give the child even more attention at times she has
not been harming herself. When possible, get advice from a child psychologist.
STRANGE BEHAVIOR
Children with different disabilities sometimes develop unusual
habits or patterns of behavior. This is especially true for retarded or
brain-damaged children who may be confused or frightened because they have
difficulty understanding what goes on around them.
In helping children through such difficulties, first try to
understand what might ‘trigger’ or be the cause of the behavior. For
example:
Rocking
Figure
“Joel often starts rocking back and forth, and seems to
escape into his own world! He then shows no interest in anything that is
happening around him. Sometimes he rocks for almost an hour.”
“When does this happen most?”
“Mainly when he is with a group of other children, or when
there are guests. But sometimes when he’s just alone.”
Joel seems to withdraw into his world of rocking when things get
too confusing, frightening, or even boring, for him. To stop rocking he may need
to be helped, little by little, to discover that interaction and play with other
persons and things can be enjoyable. But to avoid confusing and frustrating him,
new people, toys, and activities will need to be introduced gently, a little at
a time, by the persons he knows and trusts most. You might praise or reward him
when he smiles or shows any interest in playing with other children, or with new
toys. When he starts to rock, try to interest him in things you know he likes.
(But make sure to spend more time doing things he likes with him when he is
not rocking. Otherwise you will be encouraging him to rock more often to get
your attention.)
Eye poking

Figure
“My 5-year-old daughter, Judy, is blind and somewhat
retarded. She has a habit of poking her fingers deep into her eyes. As a result,
her eyes often get infected.”
For Judy, who lives in the dark, life is not always very
interesting. She cannot see things to play with. When she tries to explore, she
bumps into things. She has found that poking her eyes causes flashes of light,
so she has made a game of this. Also, she has discovered that when she pokes her
eyes her mother comes running. Sometimes mother slaps her hands, but at least
she gets attention!
For Judy to learn not to poke her eyes, she will need a lot of
help to find things to do that are more interesting and rewarding:
· toys that have
interesting shapes and surfaces and that make different sounds.
· perhaps her own
‘space’ or part of the house where everything is always kept in the
same place so she can learn her way around and find her toys. (See Chapter 30 on
blindness.)

Figure
· giving her more
attention and praise when she does not rub her eyes than when she
does.
Whenever your child develops behavior that you have trouble
understanding, it may help to ask: What does the child gain from the
behavior? What are his alternatives and in what way do they offer him less
reward? And, how can we help provide alternatives that are more rewarding to
him?
Chapter 41: ‘Learning Disabilities’ in Children with Normal Intelligence
Some children, whose minds in most ways seem quick and normal,
have difficulty learning or remembering certain things.
For example, a child may have great difficulty learning to read,
often mixing up certain words, letters or numbers. Or he may have trouble
remembering names of persons, things or places. These ‘blocks’ to
learning may happen in a child who is as intelligent, or even more intelligent,
than most children the same age.

The child who has difficulty
learning or remembering certain things may show unusual skills or talents in
other ways. In some ways, he may prove to be more intelligent than average.
In developed countries at least one child in 30 is thought to
have a learning disability. In poor countries nobody knows how
many. Any child who in the first years of life seems to develop abilities and
understanding about as quickly as other young children, yet at a certain age
begins to show difficulty learning or remembering certain things, may have this
kind of ‘special learning disability’ (or call it what you like).
Often these children are unusually active, have a hard time sitting still, or
may develop certain behavior problems.
WHAT TO DO
· These children
(even more than most) have a great need for love, understanding, and
appreciation of the things they do well.
· It is very important not to
treat these children as stupid or ‘retarded’. Praise the child and
try to help her develop in areas where she shows interest or ability.
· Often the best way to help a
child learn in the area where she has special difficulty is to introduce it,
little by little, through activities the child likes and can do
well.
For example, a child who has difficulty learning and using
numbers, but likes building things, can gradually begin to take measurements for
cutting and shaping the pieces for the things he builds.
· Do not blame,
scold or punish the child for not learning, or for ‘not trying’. This
may only make things worse. A child can easily become frustrated with her
special learning difficulty. Trying to force or shame her into learning can make
her more restless, angry, or rebellious. Some children will not admit to
themselves and others that they have trouble learning something. Instead they
hide their difficulty by pretending they do not want to learn. Thus a child who
has a special learning disability may be mistaken for one who is simply
stubborn, lazy or a trouble-maker. The child may become defensive and
uncooperative. You will need to show a lot of understanding, patience, and proof
of your respect for the child in order to win his trust and cooperation. But
after trust and respect are established, he may become as eager and considerate
as he was stubborn and troublesome before.

Figure
· Special help with
learning may be needed. It often works best to move forward in small steps, with
much repetition, so that the child finds it easier and gains confidence. (See
Chapter 34.) Make study periods short and mix them with activities that the
child likes. And of course, try to make learning fun.
· Let the child learn, and use
what she learns, at her own speed. Do not hurry her. Help her to relax. It has
been found that when children who have difficulty with reading or writing are
given all the time they need to take tests, they often do as well as other
students.
· Some very intelligent children
never learn to read or write. Some of these children, if given a chance to study
with the help of tape recorders or other means, have completed university
degrees. Others have preferred to leave school and learn other skills. Many have
become leaders in their communities or work places. What is important is to help
and encourage these children to develop in the areas where they are
strongest.
|
WARNING: Some doctors are quick to treat
learning disabilities with medicines-especially when the children are very
active. Use of medicine is often not helpful, and may do more harm than good.
Try to get advice from several experienced persons before giving any
medicines. |
E. Exercises and Techniques
Chapter 42: Range-of-motion and Other Exercises
All children need exercise to keep their bodies strong,
flexible, and healthy. Most village children get all the exercise they need
through ordinary daily activity: crawling, walking, running, climbing,
playing games, lifting things, carrying the baby, and helping with work
in the house and farm.
As much as is possible, disabled children should get their
exercise in these same ways. However, sometimes a child’s
disability does not let him use or move his body, or parts
of it, well enough to get the exercise he needs. Muscles
that are not used regularly grow weak. Joints that are not moved through
their full range of motion get stiff and can no longer be completely
straightened or bent (see Chapter 8 on contractures). So we
need to make sure that the disabled child uses and keeps strong whatever muscles
he has, and that he moves all the parts of his body through their full range of
motion. Sometimes a child may need help with these exercises. But as much as
possible, he should be encouraged to do them himself, in ways that are useful
and fun.
As much as possible, disabled
children should get their exercise in ways that are useful and fun!
Different exercises for different needs
Different kinds of exercises are needed to meet the special
needs of different children. On the next two pages we give an example of each
kind of exercise. Then we look at some of the different exercises in more
detail.
|
Purpose of exercise |
Kind of exercise |
|
To maintain or increase joint motion |
1. range-of-motion exercises (ROM)
2. stretching exercises
|
|
|
3. strengthening exercise with motion: exercises that work the
muscles and move the joint against resistance |
|
To maintain or increase strength |
4. strengthening exercises without motion: exercises that work
the muscles without moving the joint |
|
To improve position |
5. practice at holding things or doing things in good positions
|
|
To improve control |
6. practice doing certain movements and actions, to improve
balance or control |
DIFFERENT KINDS OF EXERCISES AND WHEN TO USE THEM
1. Range-of-motion exercises (ROM)
|
Ram is 2 years old. Two weeks ago he became sick with polio and
both legs became paralyzed. |
Ram needs range-of-motion exercises to keep the full motion
of his joints, so they will not develop contractures. |
At least 2 times a day, his mother slowly bends, straightens,
and moves all the joints as far as they normally go. |
All these are exercises for his knee. For other ROM exercises he
needs. |
|

Figure
|
Figure
|

Figure
|

Figure
|
2. Stretching exercises
|
Lola, who is now 4, had polio at age 2. She did not have any
exercises to keep the range of motion in her joints, and now she has severe
contractures especially of the knees.

Figure
|
Lola’s mother does stretching exercises several times a
day, to straighten the joints a little more each day. Stretching
exercises are like ROM exercises, but the joint is held with firm, steady
pressure in a position that slowly stretches it.

Figure
|
3. Strengthening exercises with motion
|

Figure
|
Chon was 6 years old when he got his clothes and body wet with a
poison his father used to kill weeds. A week later his legs became so weak he
could not stand. Now, 2 months have passed, and Chon is a little stronger. But
he still falls when he tries to stand. |
To help strengthen the weak muscles in his thighs, Chon
can raise and lower his leg like this - first without added weight and later
with a sandbag on his ankle. As his leg gets stronger the weight can be
increased. |

Figure
|
4. Strengthening exercises without motion
|
Clara, who is 9 years old, has a very painful knee. It hurts her
to move it and her thigh muscles have become so weak she cannot stand on the
leg. She cannot do exercises like Chon does because it hurts her knee too much.
But Clara can do exercises to strengthen her leg without moving
her knee. She holds it straight and tightens the muscles in her thigh. |

Figure
|
For more information on ‘exercises without motion’.
5. Exercises to improve position
|
Ernesto is 8 years old and has early signs of muscular
dystrophy. Among other problems, he is developing a sway back. |

Figure
|
Ask Ernesto to stand against a wall and to pull in his stomach
so that his lower back comes as close to the wall as possible. Ask him to try to
always stand that way, and praise him when he does. |

Figure
|
Because swayback is often partly caused by weak stomach muscles,
strengthening the stomach muscles by doing ‘sit-ups’ may also help.
See if Ernesto can still do sit-ups - at least part way, and have him do them
twice a day.
It is best to do sit-ups with the knees bent. (With legs
straight, the hip-bending muscles may do more work than the stomach muscles.)

Figure
|
6. Exercises to improve balance and control
|
Celia is 3 and still cannot walk without being held up. She has
poor balance. Many exercises and activities might help her improve her balance
and control of her body. Here are 2 ideas for different stages in her
development. For other possibilities, see Chapter 35 on Early Stimulation. |
Play games with her to see if she can lift one leg, and then the
other.
Figure
This will help her shift her weight from side to side and keep
her balance. |
After Celia has learned to walk alone, if she still seems
unsteady, walking on a log or narrow board may help her to improve her balance.

Figure
|
COMBINED EXERCISES
Often several kinds of exercises, involving different parts of
the body, can be done through one activity - often an ordinary activity that
children enjoy.
|
For example, Kim, who is 8 years old, had polio as a baby. His
right leg is weak, his knee does not quite straighten, and the heel cord
of his right foot is getting tight. He is also developing a sway back.
Figure
|
Many of the exercises Kim needs he can do by riding a
bicycle.
Figure
Learning to ride improves his balance and his control, so
that all parts of his body work smoothly together. |
|
Note: Ordinary activities that exercise the whole
body, like riding a bicycle or swimming, can provide many of the exercises that
a child needs. But sometimes specific exercises using special methods are
needed. Some special exercises are included in this chapter. |
RANGE-OF-MOTION (ROM) EXERCISES
What are they?
Range-of-motion exercises are regularly repeated exercises that
straighten or bend one or more joints of the body and move them in all the
directions that a joint normally moves.
Why?
The main purpose of these exercises is to keep the joints
flexible. They can help prevent joint stiffness, contractures, and deformities.

Figure
|
Range-of-motion exercises are especially important for
prevention of joint contractures. This danger is greatest when paralysis
or spasticity causes ‘muscle imbalance’ - which means the
muscles that pull a joint one way are much stronger than those that should pull
it the other way, so that the joint is continuously kept bent or kept straight.
|
Who should do them?
Range-of-motion exercises are important for:
· babies born with
cerebral palsy, spina bifida, club feet, or other conditions that may lead to
gradually increasing deformities.
· persons who are so sick, weak,
or badly injured that they cannot get out of bed or move their bodies very much.
· persons who have an illness or
injury causing damage to the brain or spinal cord,
including:
· polio
(during and following the original illness)
·
meningitis or encephalitis (infections of the
brain)
· spinal cord injury
· stroke (paralysis from bleeding or blood clot in the
brain, mostly in older adults, see Where There Is No
Doctor)
· children with
parts of their bodies paralyzed from polio, injury, or other causes, especially
when there is muscle imbalance, with risk of contractures.
· children with
progressive nerve or muscle disease, including muscular
dystrophy and leprosy.
· children who have lost part of
a limb (amputation).
How often?
ROM exercises should usually be done at least 2 times a day. If
some joint motion has already been lost and you are trying to get it back, do
the exercises more often, and for longer each time.
at least twice a day
When should range-of-motion exercises be started?
Early! Start before any loss in range of motion begins. With
gentleness and caution, help a severely ill or recently paralyzed child to do
range-of-motion exercises from the first few days. Starting range-of-motion
exercises EARLY can reduce or prevent disability.
|

Figure
|
KOFI AND MEDA |

Figure
|
|
Kofi and Meda got meningitis on the same day. With quick, good
medical treatment both survived. But both had suffered brain damage that left
their bodies stiff and bent. |
|
From the time his fever dropped, Kofi’s mother did
exercises with him - 2 times every day.
As he got better, she also played with him a lot - in ways that
helped him stretch and bend all joints as much as possible.

Little by little Kofi’s body
began to loosen up.
|
Meda’s mother cared for her child as best she could, but no
one told her about exercises.

Meda’s body became more and
more tight and bent.
|
|
In both children the muscle spasms gradually went away. By 6
months both could control their body movements almost normally. |
|
Because Kofi’s joints were kept flexible, as his muscle
control came back he learned to use his body nearly as well as any child his
age. |
When Meda’s muscle control returned, his muscles had
shortened so much that he could not straighten his hips or knees enough to walk.
He could only crawl, and his body became more and more deformed. |
|
Figure
|
RESULTS WITH AND WITHOUT RANGE-OF-MOTION EXERCISES |
Figure
|
|
It is much easier to prevent these problems than to correct
them. |

Figure
|
For how long should range-of-motion exercises be
continued?
To prevent contractures or deformities, range-of-motion
exercises often need to be continued all through life. Therefore it is
important that a child learn to move the affected parts of his body through
their full range of motion as part of work, play, and daily activity. If the
range of motion remains good, and the child seems to be getting enough motion
through daily activities, then the exercises can be done less often. Or simply
check every few weeks to be sure there is no loss in range of motion.
Which joints?
Exercise all the joints that the child does not move through
normal range of motion during her daily activities. For a child who is very ill
or newly paralyzed, this may mean exercising all the joints of the body.
For a child with one paralyzed limb, range-of-motion exercises usually only
need to be done with that limb (including the hip or shoulder). Children with
arthritis may need range-of-motion exercises in all their joints, including the
back, neck, and even jaw and ribs.
GUIDELINES FOR DOING STRETCHING AND RANGE-OF-MOTION
EXERCISES
1. When doing these exercises, consider the position of the
whole child, not just the joint you are moving. For example:
|
The knee will often straighten more (and you will be stretching
different muscles) when the hip is straight, (1)

Figure
|
than when the hip is bent.

Figure
|
This is because some muscles go from the hipbone to below the
knee.

Figure
|
To prove this, try to touch your toes with your knees straight.
You will feel the muscles (1) stretch, and the cords tighten here. (2) |
In a similar way, movement in the ankle is affected by the
position of the knee, and movement of the fingers by the position of the wrist.
2. If the joints are stiff or painful, or cords and muscles are
tight, often it helps to apply heat to the joint and muscles before
beginning to move or stretch them. Heat reduces pain and relaxes tight muscles.
Heat can be applied with hot water soaks, a warm bath, or hot wax. For methods.
|
For a stiff, painful joint,

Figure
|
apply heat for 10 or 15 minutes

Figure
|
before doing the exercises.

Figure
|
3. Move the joint SLOWLY through its complete range of
motion.
If the range is not complete, try to stretch it slowly and
gently just a little more each time. Do not use force, and stop stretching when
it starts to hurt.
|
Hold the limb in a stretched position while you count to 25.
Figure
|
Then slowly stretch the joint a little more and hold it again
for a while.

Figure
|
Continue this way until you have stretched it as far as you can
without forcing it or causing much pain.

Figure
|
The more often you repeat this, the faster the limb will get
straighter.
4. Have the child herself do as much of the exercise as she
can. Help her only with what she cannot do herself. For example:
|
Instead of doing the child’s range-of-motion exercise for
her,

Figure
|
have her do the exercise using her own muscles as much as she
can.
Figure
|
Then have her help with the other hand (or you help her if
necessary).

Figure
|
|
Whenever possible, exercises that help to maintain or
increase joint motion should also help to maintain or increase strength.
In other words, range-of-motion, stretching, and strengthening exercises
can often be done together. |
THERE ARE 3 MAIN WAYS OF DOING RANGE-OF-MOTION EXERCISES
|
1. Passive exercise. If the child cannot move the limb at
all, either you can do it for him... |
or he can move the limb through its full range with another part
of his body.

Figure
|
|
Figure
|

Figure
|

Figure
|
|
2. Assisted exercise. If the child has enough strength to
move the affected part of her body a little, have her move it as far as she can.
Then help her the rest of the way.
|
Figure
|

Figure
|
3. Active exercise. If the child has enough strength to
move the body part by itself through its full, normal range of motion, then he
can do the exercises without assistance, or ‘actively’. When the child
can do it, active exercise is usually best, because it also helps maintain or
increase strength.
|
If muscle strength is poor, have the child move his limb while
in a position so that he does not have to lift its weight.
If necessary, support the limb with your hands, in a sling, or
on a small roller board.

Figure
|
If he can lift the weight of his limb through its full range of
motion, let him exercise in a position to do it. For example, he can lie on his
side and lift his leg up sideways.

Figure
|
If he can lift the limb’s weight easily, add resistance by
pushing against the limb or by tying a sandbag to it. This helps strengthen the
muscles for that motion.

cloth bag filled with sand
|
|
As the child gains strength, gradually increase resistance
(add more weight). |
|
For many exercises, resistance can be added with stretch
bands. Cut rubber bands from an old inner tube. The wider the band, the more
resistance it will give. |
Twist the leg in (and the hip out).
Figure
|
Twist the leg out (and the hip in).

Figure
|
|
This child is doing range-of-motion and strengthening exercises
at the same time. |
COMMON SENSE PRECAUTIONS WHEN DOING EXERCISES
Every child’s needs are different. Please do not simply do,
or recommend, the same exercises for each child. First THINK about the
child’s problems and needs, what exercises might help her most, and what
could possibly harm her. Adapt the exercises to the child’s needs, and
to how she responds. Here are some important precautions:
1. Protect the joint. Weak joints can easily be damaged
by stretching exercises, unless care is taken. Hold the limb both above and
below the joint that you are exercising. And support as much of the limb
as you can.
|
Hold the leg firmly just above the knee.

Figure
Hold the leg just below the knee and
support the whole leg with your arm. |
Do not push directly on the joint.
Do not pull far from the knee.

Figure
|
|
WARNING: Pulling here can dislocate the
knee (or break the bone). |
2. Be gentle-and move the joints SLOWLY - especially when
a child has spasticity, or when joints are stiff or painful.
|
WARNING: Moving spastic joints rapidly
makes them stiffer. SLOW DOWN! |
For example, Teresa has juvenile arthritis and her joints are
very painful. She holds them in bent positions that are leading to contractures.
Move the joints very slowly and gently, as far as you can without causing too
much pain. Straighten them little by little, like this:
|

Figure
|

Figure
|
|
A common mistake is to rapidly move the limb back
and forth like the handle of a pump. This does no good and can do harm. Go
slow, with gentle, steady pressure. |
3. Do no harm. In children who have recently broken their
neck, back, or other bones, or who have serious injuries, exercises should be
done with great caution. Be careful not to move the broken or injured part of
the body. This may mean that some joints cannot be exercised until the bones
have joined or wounds healed. (For broken bones, usually wait 4 to 6 weeks.)
4. Never force the motion. Stretching will often cause
discomfort, but it should not be very painful. If the child cannot tell you, or
does not feel, be extra careful. Feel how tight the cords are to be sure you do
not tear them.

Figure
5. Do not do exercises that will increase the range of motion
of joints that are ‘floppy’ or that already bend or straighten more
than they should.
|
If a child has ankles that already bend up too much, |
do not do ROM or stretching exercises that
pull the foot up. |
Or if a child’s foot bends in more
than normal, but does not bend out, |
do exercises to bend the foot
out, |
but do not do exercises that bend the foot
in. |
|

Figure
|

Figure
|
Figure
|

Figure
|

Figure
|
Do exercises in the opposite direction of the deformity or
contracture, so that they help to put the joint into a more normal position.
6. Before doing exercises to increase the range of motion in
certain joints, consider whether the increased motion will make it easier for
the child to do things.
Sometimes, certain contractures or joint stiffness may actually
help a child to do things better.
|
For example, a child with a short leg may walk better if a tight
heel cord keeps his foot in a tiptoe position.
Figure
|
Similarly, a child with paralysis in the thigh muscles may
actually walk better if a tight heel cord prevents his foot from bending up.
|
This foot does not bend up. The tight heel cord holds the leg
back and keeps the knee from bending. (1)

Figure
|
Stretching exercises to bend the foot up may cause the weak knee
to bend when the child tries to walk.

Figure
|
A child with cerebral palsy or arthritis often needs exercises
to maintain or improve the movement of the back. However, a child with spinal
cord injury or muscular dystrophy may do better if the back is allowed to stay
stiff - especially if it is in a fairly good position.
|
Because of their weak back muscles, these children often develop
a slouched or hunchback position. Range-of-motion exercise to increase
flexibility could make the posture worse! |

with ROM back exercise
|
Allowing the child’s back to stiffen in a good position may
help him to sit straighter. |

without ROM back exercise
|
In persons with quadriplegia or other paralysis that
affects the fingers, avoid stretching open the fingers with the wrist bent
back.
|
A quadriplegic person with no muscle power in his fingers can
often pick things up by bending the wrist back. Tight cords make the fingers
bend.

RIGHT
To keep this holding function, straighten fingers with wrist
bent down, |

Figure

WRONG
Do not stretch the fingers with the wrist bent back.
|
For the same reason, the quadriplegic child should also learn to
support herself on her hands with her fingers bent, not straight.

RIGHT

WRONG
|
7. In doing range-of-motion exercises for a stiff neck, caution
is needed to make sure the neck bones do not slip and cause damage to the
spinal nerves. This damage can cause total paralysis or even death. The
danger is especially great in persons with arthritis, Down syndrome, or neck
injury. Do not use any force to help the person bend her neck. Let her do it
herself, slowly, with many repetitions, and without forcing.
8. In children with cerebral palsy, sometimes the
standard range-of-motion exercises will increase spasticity and make
bending or straightening of a particular joint difficult or impossible. Often
the spastic muscles can be relaxed by positioning the child
in a certain way before trying to exercise the limb. For example:
|
When a child with spasticity lies straight, his back, his head
and shoulders may push back. His legs also stiffen and will be hard to bend.
Figure
It may be very hard to bend the spastic legs of a child in this
position. |
But if we position the child with his back, shoulders, and head
bent forward, this helps to relax his stiff legs and will make motion easier.
Figure
|
It may also help to rotate the leg outward before trying to bend
the knee. |
|
A hammock is good for positioning the child with cerebral palsy
who stiffens backward. |
|
REMEMBER: Fast movements increase
spasticity.
Do exercises VERY SLOWLY. |
|
CAUTION: Range-of-motion exercises are very important
for many children with spasticity, but special techniques are needed. More
examples of how to relax spasticity are given in Chapter 9 on cerebral palsy.
However, you can learn a lot by trying different positions until you find the
ones that help relax the spasticity. |
9. In joints where there is muscle imbalance, do
exercises to strengthen the weaker muscles, not the stronger ones. This will
help to prevent contractures by making the muscle balance more equal:
|
If the muscles that straighten the knee are weak, (1)

Figure
and the muscles that bend the knee are strong, (2) |
then do exercises that strengthen the weaker side.

Figure
This will make stronger the muscles that straighten the knee. It
helps prevent contractures. |
Do not do exercises that strengthen the
stronger side.

Figure
This will make the muscles stronger that bend the knee - and
make contractures more likely. |
In daily activities, also, look for ways to give weak muscles
more exercise than strong ones. This advice is discussed in more detail in
Chapter 16 on juvenile arthritis.
IDEAS FOR MAKING EXERCISES FUN
Exercises can quickly become boring, and the child will not want
to do them. So turn them into games whenever possible.
|
LOOK FOR WAYS TO MAKE IT FUN!
a good ROM exercise for
fingers
|

Figure
One good way is to involve the children in games with other
children. Try to think of ways to adapt games so that they help to stretch
the joints and exercise the muscles that most need it.
A boy with cerebral palsy rolls a ball so that a girl with
juvenile arthritis can kick it. This helps her to straighten her knees, and to
strengthen the muscles that straighten them.
Figure
In the picture below, children play ball to help Mar�a, a girl
with juvenile arthritis, stretch her stiff joints and muscles.

Figure
Can you see how the 2 children on the left are helping Mar�a
with ‘range-of-motion’ exercises?
Which of Maria’s joints are they exercising?
Answers:
The children form a triangle, so that to catch the ball Maria
has to twist her body to one side, and to throw it she has to twist to the other
side. This helps loosen her stiff back and neck. Also, sometimes they throw the
ball high so that she has to lift her head and raise her arms high to catch it.
This way Mar�a exercises her neck, back, shoulders, elbows,
wrists, hands, and fingers. And the play helps her forget the pain of movement -
pain that often makes range-of-motion exercises seem like punishment. But this
way she has fun.
Complete range-of-motion exercises - upper limbs*
* Drawings on pages 378 to 380 are adapted from
Range-of-Motion by Hewitt/Jaeger.
Do these exercises slowly and steadily. Never use force, as this
could damage a joint.
Do one joint at a time. Hold the limb steady (stabilize it) with
one hand just above the joint, and place your other hand below the joint to move
the part through its full range of motion. Here we show the basic exercises
only. But remember, try to do them in ways that make it fun!
|
SHOULDER: arm up and down |
SHOULDER: arm back and forward |
|
Figure
|

Figure
Raise arm straight forward, and up. |

Figure
Move arm all the way back, |

Figure
and then all the way forward over the chest. |
|
SHOULDER: rotation |
SHOULDER: out to side |
|

Figure
With elbow bent |
Figure
turn the arm all the way up, |

Figure
then all the way down. |

Figure
|

Figure
|
|
|
|
Raise arm straight out to side. |
|
ELBOW: straighten and bend |
FOREARM: twist |
|
Figure
Straighten the arm out from the side, |

Figure
then bend the elbow to bring hand up to shoulder. |

Figure
Holding the wrist twist the hand up, |
Figure
and then twist it down (gently). |
|
WRIST: up and down |
WRIST: side to side |
|

Figure
|
|
|
|

Figure
Bend wrist back, |
Figure
and then forward. |

Figure
Bend to outside. |

Figure
Bend to thumb side. (It will not bend very far to thumb side. Do
not force.) |
|
FINGERS: close and open |
FINGERS: spread |
|

Figure
Make a fist. |

Figure
Straighten gently. |
Figure
Spread each finger one at a time. |
|
FINGERS: straighten while bent at hand |
THUMB: for grasping |
|

Figure
|

Figure
|

Figure
Bend thumb toward base of little finger. |
|
THUMB: shut and open |
THUMB: up and down |
|

Figure
Bend the joints of the thumb in all the way, |

Figure
then open thumb all the way to the side. |

down
|

up
|
|
|
Move straightened thumb down and then up, with palm flat and
fingers open. |
Range-of-motion exercises - lower limbs
(Also see the exercise sheets)
|
KNEE |
|
HIP: straighten |
in an older child |
|

Figure
Bring heel back as far as possible, |

Figure
then straighten leg as much as possible. |
Figure
|
Figure
|
|
|
Be sure hip stays flat against a firm surface as you bend leg
up. |
|
HIP: bend |
HIP: spread |
|

Figure
Bend knee to chest. |

Figure
Straighten all the way. |

Figure
|

Figure
|

Figure
|
|
|
|
Spread hips open as far as you can by moving leg out to the
side. |
|
HIP: twist (rotation) - leg straight |
HIP ROTATION: leg bent |
|

Figure
|

Figure
|

Figure
then to outside. |

Figure
With knee bent, |

Figure
swing leg out, |

Figure
then in. |
|
Roll leg and foot to inside, |
|
|
|
|
|
ANKLE AND FOOT: down and up. |
IMPORTANT: To stretch a tight heel cord,
pull heel down as you push foot up. |
|

Figure
Bend foot down. |
Figure
Pull heel down and bend foot up. |
Pull heel harder than you push on foot - or you may dislocate
foot upward instead of stretching the ankle cord and muscles. |
Figure
|
|
ANKLE TWISTING: in and out |
TOES: up and down |
|

Figure
|

Figure
Twist in. |

Figure
Twist out. |

Figure
Bend toes up. |

Figure
Bend toes down. |
Range-of-motion exercises - neck and trunk
We show these as active exercises. Usually they should be done
by the person himself. If any help is given it should be very gentle, with no
force, especially when exercising a stiff neck. (See precaution.)
NECK
|

Figure
|

Figure
|

Figure
|
Figure
|
|
Turn head to left and to right, |
side to side, |
up and down, |
and back and forward. |
TRUNK
|

Figure
|
Figure
|

Figure
|
Figure
|
|
Bend back. |
Bend forward. |
Bend sideways. |
Twist. |
UPPER BACK (shoulder blades):
|

Figure
|

Figure
|

Figure
|
|
Bringing shoulders forward, pulls the shoulder blades wide
apart. |
Pulling shoulders back, pushes the shoulder blades close
together. |
Pull shoulders Push shoulders up toward ears down. |
RIBS
|

Figure
Breathe in deeply. |

Figure
Breathe out deeply. See how long you can whistle or blow.
(Blow a whistle or blow up a balloon.) |
JAW
|

Figure
Pull jaw back, |

Figure
and push forward. |

Figure
Open mouth wide. |
|
Move jaw to one side,

Figure
|
|
and then to the other side.
Figure
|
EXERCISE INSTRUCTION SHEETS-For Giving To Parents
If you give the family pictures of the exercises that their
child needs, they will be more likely to do them - and do them right.
On the next few pages are samples of exercise sheets that
you can copy and give to families. They show some of the home exercises that we
have found are needed most often.
However, these exercise sheets should not be a substitute for
hands-on demonstration and guided practice. Instead, give them to the family
after you teach them how to do the exercises. In teaching an exercise or
activity:
|
1. First show and explain.

Figure
|
2. Next have the family and child practice until they do it
right and understand why.

Figure
|
|
3. Then give her the instruction sheets and explain the main
ideas again.

Figure
|
4. For exercises to correct contractures, consider giving the
family a ‘flexikin’. Show them how to measure and record the
child’s progress. This lets them ‘see’ the child’s gradual
improvement, so they are likely to work harder at the exercises. (See
“Flexikins” in Chapter 5.)
Figure
|
You may want to prepare more sheets showing other exercises,
activities, or play ideas that are included in this book. Better still, make
sheets showing exercises and activities in ways that fit your local customs
and that help the child to take part in the life of the community. (See
Chapters 1 and 2.)
STRETCHING EXERCISE-TO HELP YOUR CHILD PUT HER FOOT DOWN FLAT
(TO CORRECT A ‘TIPTOE’ CONTRACTURE)
|

Figure
|
PROBLEM
The muscles at the back of the lower leg (calf muscles) that
hold the foot ‘tiptoe’, are too short and tight.
For this reason the child cannot put her foot flat on the
ground. |
Use your arm to hold the foot in position like this. Gently lift
but do not force the foot upward.

Figure
Pull down on the heel and push up on the foot, firmly and
steadily while counting slowly to 25. Relax, then do it again. Repeat this
exercise 10 to 20 times - in the morning, at noon, and in the evening.
|
WARNING: Pushing here can injure the knee of cause it to bend
backward - especially if the upper leg is weak.

WRONG
|
Pushing like this can hurt or dislocate the foot instead of
stretching the cord - especially if the foot is paralyzed or very weak.
WRONG
|
STRETCHING EXERCISE-TO STRAIGHTEN A STIFF KNEE (KNEE
CONTRACTURE)
|

Figure
|
PROBLEM
The muscle and cord here are too short and tight. For this
reason the knee will not straighten. |
Ask the child to straighten his knee as much as he can by
himself (if he can do it at all). Then help him slowly straighten it as far as
it will go.
Both of you keep working to hold the knee as straight as
possible while you count slowly to 25. Repeat several times. Do this exercise 3
times a day.
If the foot also has a contracture, try to hold or bend it up
while you stretch the cord behind the knee.

Figure

Figure
When you get the knee as straight as you can with the hip
extended, gradually lift the leg higher, keeping the knee straight.
|
LIKE THIS

Figure
|
NOT LIKE THIS

Figure
|
|
BE CAREFUL. Never try to straighten the leg by pulling
the foot. Instead of stretching the cord, this could dislocate the knee or break
the leg. The danger is especially great when the leg is very weak or when the
child cannot walk. |
STRETCHING EXERCISE-FOR A BENT-HIP CONTRACTURE
|
PROBLEM
The thigh is pulled forward by tight cords and cannot straighten
backward. |
Figure
|
Rest the thigh against your thigh, and support the leg with your
arm.
With firm and steady force, pull the leg up while counting
slowly to 25.

Figure
Rest the thigh against your thigh, and support the leg with your
arm.
With firm and steady force, pull the leg up while counting
slowly to 25.
Repeat several times. Do this exercise 3 or more times a day.
|
VIEW FROM ABOVE |
|
|
Do the exercise with the leg in a straight line with the body.
|
Make sure the hips are against the table and that they do not
lift up as the leg is lifted. |
|
Figure
|
LIKE THIS |

Figure
|
LIKE THIS |
|

Figure
|
NOT LIKE THIS |
Figure
|
NOT LIKE THIS |
EXERCISES AND POSITIONS TO HELP AVOID PRESSURE SORES AND
CONTRACTURES
Children who spend a lot of time lying or sitting, or have lost
feeling in their butts, should NOT SPEND ALL DAY SITTING DOWN. This can cause
pressure sores, contractures of the hips and knees, and back deformities.
|
PREVENT THIS |
PREVENT THIS |
|
Figure
Pressure sores |

Contractures
Hips and knees are contracted (cannot be straightened) from
sitting too much. (1) |
|
When you spend time sitting in a wheelchair (or any chair) lift
yourself up with your arms like this and count to 25 every 1 5 or 20 minutes.
|

Figure
Be sure to use a soft cushion. (1) |
Lifting up often is especially important for people who do not
have feeling in their butt, so that they do not get sores on their bottom. |
|
Spend a part of the day lying down with your shoulders up like
this. |

Figure
cushions or foam rubber wedges (1) |
|
You can do schoolwork lying down. Try to arrange things with the
teacher so that you can spend part of your day lying down.
Figure
|
If the child cannot straighten enough to lie on the floor, he
can lie on a table, and work or play with his hands at a lower level, as shown
here. |
|
BE CAREFUL: To avoid sores, it is important
to put foam rubber cushions to protect the body where bones press against
skin-especially if you cannot feel in parts of your body. |
EXERCISE FOR A STRAIGHTER BACK
|
PROBLEM
The upper back bends forward (in older persons this is a common
cause of high back pain). Often the shoulders and shoulder blades are also
stiff.

Figure
|
Lie face down and move the arms as shown. This helps keep the
shoulder blades and upper back flexible.

Figure

Figure

Figure
|
|
Put a strap around the upper body and bend backward as far as
you can.

Figure
Or put pressure against the middle of the upper back and have
the child try to straighten against it.

Figure
Stay in this position while you count to 25. Do the exercise 2
or 3 times a day. |
|
|

Figure
|
Also, for at least half an hour a day, lie with a rolled up
towel or cloth under the middle of the curve in your back. Breathe deeply, and
every time you breathe out, try to let your body bend backward over the roll.
|
|
Note: Some experts believe that the
exercises that bend the back up and back, as shown above, may also help keep a
mild sideways curve of the spine (scoliosis) from getting worse. But the
exercises will not help much if the curve is severe. |

Figure
|
|
CAUTION: Bending back like this usually
bends the lower back too much and does little or nothing to help straighten the
upper back. It may make the problem worse.
NO!
Figure
|
STRENGTHENING EXERCISES-TO GET ARMS READY TO WALK WITH
CRUTCHES
|
Figure
|
OBJECTIVE
These exercises help make your arms stronger so that you can
walk with crutches. |
Figure
|
|
Sit like this and lift yourself up with your arms.

Figure
|
Go up and down until your arms are so tired you cannot lift
yourself another time.

Figure
|
It is better to use bricks or books to lift yourself higher.

Figure
|
|
Note: If the child’s arms are too short to lift
himself up on open hands, he can use his fists.

Figure
|
Try to lift yourself with your elbows out, like this,

Figure
|
and not like this.
Figure
|
|
To practice for using crutches, make ‘handgrips’.

Figure
|
Or use a sawed-off crutch.

Figure
|
Or you can do these exercises in your wheelchair.

Figure
|

Weight lifting. Increase the
weight little by little as the arms get stronger.
|
|
Do these exercises 3 or 4 times a day. Every day try to lift
yourself more times without resting, until you can do it 50 times. |
|
STRENGTHENING EXERCISES-TO HELP YOUR CHILD HAVE STRONGER
THIGHS
|

Figure
|
PROBLEM
Weak muscles in the front part of the upper leg (thigh muscles)
make it difficult to support weight with that leg. |
|
Raise your leg and hold it up until you cannot hold it up any
longer. Then lower it as slowly as you can.

Figure
If the child cannot straighten her leg by herself, help her, but
ask her to use all her strength too.
Figure
|
Repeat as many times as possible (until you cannot lift the leg
more).
Do this exercise 2 or 3 times a day.

Figure
If her thigh is quite weak, have her straighten and bend her leg
lying sideways. She may need to have the leg supported. |
|
Figure
When his thigh is stronger, put a little bag of sand on his
ankle so that he will use more strength to raise it. |
It also helps to stand on the leg, then bend as far as possible
and straighten again. Repeat many times.

Figure
|
|
Figure
If the leg gets strong enough, practice going up and down steps.
Start with low steps and slowly progress to higher ones. |

Figure
|

homemade tricycle
|
|
Climbing hills or riding a tricycle or bicycle also helps
strengthen the thighs. |
STRENGTHENING EXERCISE-FOR THE MUSCLES ON THE SIDE OF THE
HIP
|
PROBLEM
weakness here causes the child to bend to one side when he
walks. (1)

Figure
|
|
Lie on your side and raise your leg as high as you can.

Figure
Keep your leg up until you get so tired that it falls by itself.
|
|
If the child cannot raise his leg by himself, help him a little,
but be sure that he uses as much strength as he can. |

Figure
|
|
Or have the child lie on his back and move his leg to the side.
You can hang the leg like this so that he can move it more easily. |

Figure
|
As he gets stronger, move the rope more to the other side to
make him work harder. |
|
Figure
|

Figure
|
Figure
|
|
If the child can raise her leg easily, add weight with your
hand, |
or with a little bag of sand. |
Think of ways to make the exercises fun. |
Repeat 3 times. Do this 3 times a day.
RANGE-OF-MOTION AND STRENGTHENING EXERCISES-FOR THE HAND AND
WRIST
These exercises can help bring back or maintain strength and
range of motion of the hand. They are useful after injuries (or surgery)
to the hand, after broken arm bones near the wrist have healed, and for
arthritis, or partial paralysis from any cause (polio, spinal cord
injury, stroke).
To do these exercises, the person should move the hand as much
as possible without help. Then, if motion is not complete, use another hand to
bend and straighten the fingers or wrist as much as possible without
forcing.
Repeat each exercise 10 to 20 times, at least 2 times every day.
|
1. Close and spread the fingers as much as possible.
Figure
|
2. Open.
|
Bend like this. |
Make a fist. |
|

Figure
|
|
3. Make ‘O’s with the thumb and each finger. |
|
|

Figure
|

After you can make the large
‘O’s, repeat making the ‘O’ as small as you can. (1)
|
|
4. Bend wrist forward and backward. (Backward is more difficult
but is especially important.)
Figure
|
5. Spread and close the thumb.
Figure
|
|
6. Bend the wrist from side to side.

Figure
|
7. Turn hands upward and downward-as far as you can.

Figure
|
MAKING HAND EXERCISES FUN OR USEFUL Look for ways to make
hand exercises fun.
|
For example, try to learn sign language from a deaf child. |
Figure
|
Or play ‘shadow puppets’ with a light. |

Figure
|
|
Aids for hand exercise |
|
|
Figure
|
|
You can buy a simple hand exerciser like this. |

Figure
|
Or make one like this. If the child makes it herself, that will
also be good exercise for her hands. (1) |
Move this post forward or back to make it harder or easier to
squeeze the aid. (2) |
This ‘acrobatic bear’ is more work to make, but
even more fun to exercise and play with.
|
Trace and cut out these pieces from wood or cardboard.
Fasten arms and legs loosely on body by putting a cord through
holes.
Figure
|

Figure
Squeezing the poles makes the bear ‘loop the loop’.
(1) |

Figure
“See if you can make the bear sit.” (1) |
|

Figure
|
To have the child squeeze harder, attach a piece of rubber hose
or car tire between the poles. (1)

Figure
|
|

Figure
|

Figure
|
view from above showing how string passes through holes in poles
and paws (1) |
A child can also get squeezing exercise with the hands by
milking goats, cutting with scissors or shears, punching holes in leather or
paper with a hand punch (while making things), by washing and wringing
clothes, and in many other ways.
For examples of how different kinds of exercises are used for
different disabilities, look under ‘Exercises’ in the
INDEX.
Chapter 43: Crutch Use, Cane Use, and Wheelchair Transfers
USE OF CRUTCHES
MAKING SURE THE CRUTCH FITS THE CHILD
|
When the child stands, the crutch should be 2 or 3 fingers’
width below the armpit. |
The elbow should be bent a little so that the child can lift
herself up to swing her feet through. (1) |
|

Figure
|
Figure
|
|
|
|
IMPORTANT
Teach the child not to ‘hang’ on the crutches with her
weight on her armpits. (1)

WRONG
In time, pressure on the nerves under the arm can cause
paralysis of the hands.(1)

Figure
|
Using elbow crutches is a good way to keep her from
hanging on her armpits. (However, these are more difficult to use for some
children.)
Figure
|
For designs and measurements of different crutches.
Walking with crutches
|
TAKING STEPS
Some children walk best by taking steps, one foot at a time.

Figure
|
For better balance and position, move the right crutch forward
together with the left leg, and then the left crutch together with the right
leg. (1)
Her ‘tracks’ should look like this. (2)

Figure
|
|
‘SWING TO’ WALKING
Many children who have difficulty taking steps use crutches by
pulling or swinging both feet forward to the level of the crutch tips. Then they
advance the crutches and pull themselves forward again.

This way is slow but sure.
|
‘SWING THROUGH’ WALKING
Although at first they may be afraid to try it, many of these
children can learn to ‘swing through’ between their crutches, like
this.

This way is fast and fun.
|
USE OF A CANE
|
It usually works best to hold the cane on the side opposite the
weaker leg. (1)
Move forward and put down the weaker leg and the cane together.
For different crutch and cane designs, see Chapter 63.
|

Figure
|
His ‘tracks’ should look like this.

Figure
|
WHEELCHAIR TRANSFERS
Persons who use wheelchairs become much more independent if they
can learn to transfer (get in and out of their wheelchairs) by
themselves, or with limited help. For those who need some help, it is important
to find ways to transfer that make it easiest both for the disabled person and
the helper.
Too often, as disabled children get bigger and heavier, mothers
and fathers hurt their own backs.
Different persons will discover their own ‘best way’
to transfer with or without help, depending on their own combination of
strengths and weaknesses.
Here we give some suggestions of ways to transfer that many
people have found to work well.
|
THE WRONG WAY TO TRANSFER

Figure
WARNING: One disability can lead to
another! |
Notice that it is often easier to transfer sideways out of a
chair, and also back into it. To transfer sideways, however, a
wheelchair without armrests, or with at least one
removable armrest, is needed. Therefore, for many disabled children,
make an effort to get or make wheelchairs without armrests or with removable
armrests. Unfortunately, most wheelchairs in many countries have fixed,
often very high, armrests. We therefore will give examples of transfers both
with and without armrests.
|
A good way to transfer the child who needs help is like this.
Put the child’s feet on the floor and lean her forward
against your body. Have her hold on as best she can.
Lift her like this and swing her onto the bed. |

Figure
|
To lift him, grip his pants or make a canvas or leather sling.

Figure
|
Ideas for wheelchair design, adaptation, and use are in
Chapters 64, 65, and 66.
Transfer from cot or bed to wheelchair without armrests
|
CAUTION: Make sure brakes are ‘on’ and
footrests are ‘up’ out of the way. |
|
To transfer from the wheelchair to the cot, follow the same
steps in reverse. |
|
Figure
|

Figure
|

Figure
|
|
1. Push yourself to a sitting position. |
2. Reach under knees one at a time. |
3. Move legs so that feet are on the floor. |
|
4. Make sure brakes are locked. Then push up on arms while
leaning forward with head facing down. Weight should be over knees. |

Figure
|
Figure
5. Move body into wheelchair. |
Transfer from cot or bed to wheelchair with armrests
|

Figure
|

Figure
|
Figure
|
|
1. Position your wheelchair so that you can swing body past
armrests. |
2. Place one hand on bed and one on the far armrest. Push
yourself up while leaning forward with head down, weight over knees. |
3. Swing body into wheelchair. |
Transfer forward from wheelchair to cot or bed (often works
well for children)
|
Figure
|

Figure
|
Figure
|
|
1. Lift feet onto bed and wheel the chair forward against bed.
Put on brakes. Then bend forward and lift butt forward on chair. |
2. With one hand on the cushion and one on the bed, lift the
body sideways onto the bed. |
3. Repeated lifts and lifting of legs may be needed. |
Transfer with sliding board - without help
For getting into and out of bed, a car, etc.

SLIDING BOARD
|
For getting into and out of bed, a car, etc. |
SLIDING BOARD |
|

Figure
|

Figure
|
|
1. Place board under hip by leaning to opposite side or by
pulling up leg. |
2. Lean forward, with your head and weight over knees. |
|
Figure
|

Figure
|
|
3. Push yourself along the board. |
4. When you are in the chair, remove the board and put it where
you can easily get it. |
Transfer with sliding board - with help
|
Figure
|

Figure
|
|
1. Lift leg and put board under hip. |
2. Have person put arms around neck (if possible) while you put
your hands under his butt, or grab his pants. |
|

Figure
|

Figure
|
|
3. Slide the person along board to bed. |
4. Lift legs onto bed. |
Transfer from floor to wheelchair - with help of a low
seat
|
Figure
|

Figure
|
|
1. Sit with legs straight. Pull seat to your side opposite the
wheelchair (a person’s knee can also be used). |
2. With hands on each chair, push up, with your head forward
over knees. |
|
Figure
|

Figure
|
|
3. Swing onto the seat. |
4. Now, with your head forward over your knees, swing body onto
the wheelchair. |
Transfer from wheelchair to floor - and back again - without
help of a stool
This woman, who has severe spasticity, transfers from
wheel-chair to bed using tin cans, ropes, and a wood frame over her bed. (Photo:
John Fago, PROJIMO.)

Figure

Figure

Figure